DESCRIPTION OF BLAST INJURIES: LITERATURE REVIEW, CASE REPORT AND PROPOSAL FOR A NEW CLASSIFICATION
Instituto Nacional de Medicina Legal y Ciencias Forenses, Suplemento
Mabel Zurbarán-Barrios1
Francisco José Calle Rúa1
Ricardo Alexis Restrepo2
1. Medical Pathologist.
National Institute of Legal Medicine and Forensic Science.
- Pathology Group -
Bogotá Office.
2. Physician.
National Institute of Legal Medicine and Forensic Science
- Pathology Group -
Bogotá Office
- Bogotá, D.C. - Colombia.
Correspondence to:
Mabel Zurbarán-Barrios.
Grupo de Patología,
Instituto Nacional de Medicina Legal y Ciencias Forenses.
Bogotá, D.C. Colombia.
Correo electrónico: mzurbaran@medicinalegal.gov.co
SUMMARY
After reviewing the medical literature of various classifications of blast injuries, we present a proposal called the Bogotá Classification, aimed at the study of cadavers with injuries present in cases of death caused by explosion. We also present a case that occurred in a residence in the city of Bogotá involving an improvised explosive device, resulting in three deaths.
Keywords: blast injuries, forensic pathology, autopsy, death.
THEORETICAL FRAMEWORK
Classifications of blast injuries: similarities and discrepancies
Blast injuries have generally been classified in clinical terms focusing on surviving victims, such as those laid out by the National Center for Injury Prevention and Control-NCIPC (1), De- Palma (2) and Wolf (3). Severe injuries resulting in immediate death were also included, as laid out by Carnicero (4), Patiño (5), Crane (6) and Saukko (7).
Medico-legal autopsies examine both the injuries of those who died immediately as well as of survivors who died a short time later; it is important to categorize these deaths in order to verify the cause of death, identify related injuries, document a sequence of events and the location of people at the scene, when possible. This helps establish the cause of death in relation to the explosion.
While injuries found on the cadavers are documented in the autopsy by describing their characteristics and mechanisms, there are discrepancies in the different classifications, either because injuries are classified among the groups differently or some injuries are not included. To provide a few examples, the classifications of the NCIPC, dePalma and Wolf don’t mention extensive and severe injuries such as decomposition and generalized bodily damage without disintegration. Carnicero, on the other hand, classifies burns and injuries caused by collapsed structures as secondary, while others (namely NCIPC and DePalma) describe them as tertiary.
The general mechanism for the production of blast injuries, caused by either high-order or low-order explosives, is the conversion of a solid or liquid to gas, and the rapid expansion of this gas with an increase in pressure and the formation of a blast wave that crosses through bodies and objects (5,8), with a subsequent blast wind displacing them. In this process, air is displaced (known as positive pressure), which forms a vacuum followed by negative pressure. This normalizes both pressures and fills the vacuum (3). The increase in positive pressure in particular is responsible for blast injuries. Gruss (8) and Marín (9) explain that the pressure that causes the injury is called effective pressure and that if an individual is against a wall, he or she will receive pressure both from the blast as well as that reflected off the wall, which causes a combination of pressures, or effective pressure.
Primary injuries: these have been defined by Bernal (10) as the most characteristic blast injuries and are a consequence of the path of the blast through the body, with disruptive effects on tissues of air/liquid or solid/liquid interfaces (2,8). They are also described by Shardin (11) and Benzinger (12) from 1950 as anatomical and physiological changes produced by the direct or reflected effect of impact force on the body’s surface.
Primary injuries that are broadly accepted in all classifications (1-7) are those that occur in the organs with air/liquid interfaces and are typically described in the ears as tympanic membrane rupture and damage to the middle ear; in the lungs as hemorrhaging, pulmonary contusions, barotrauma and air embolism; and in the gastrointestinal tract as hemorrhages and perforations of the intestines, predominantly in the colon. There is also often damage to the cecum and mesentery with hemorrhage, thrombosis or rupture.
Other primary injuries are not included in all classifications. NCIP and DePalma include ocular globe injuries and cerebral concussions without physical signs of head trauma. Marín (9) includes the atomization of extremities due to proximity to explosion and sudden death by myocardial depression. Wolf (3) considers injuries due to inertia similar to those caused by a deceleration of forces in traffic accidents, physiological shock , compartmental syndrome in extremities, orbital fractures and cardiac injuries. Uribe (13) adds traumatic amputations and a category called immediate causes of death (aortic rupture, cardiac lacerations, massive pulmonary contusion, tracheal rupture, serious fractures, compromised column and pelvis). Carnicero and Bernal include the fragmentation and projections of the body due to the generalized blast , as well as esophagus, heart, head and eye injuries. Patiño refers to major bodily destruction, traumatic brain injury and amputations. Crane includes the total destruction of the victim and blast injuries. Saukko includes bodily destruction due to non-identifiable flying fragments through a wide area (similar to that described by Carnicero and Bernal) and flash burns. The Institute of Medicine of the National Academies (IOM) (14) includes cardiovascular, ocular, musculo-skeletal and central nervous system injuries. Gruss does not include other injuries.
Some authors state, without undertaking a classification of blast injuries, that some injuries should be catalogued as primary. These include fractures in extremities that compromise the diaphysis and not the joints (15,16), cranial fractures around paranasal sinuses (16), cerebral pseudoaneurysms (17) and in the case of pregnancy, secondary abruptio placentae (18).
Secondary injuries: NCPIC, Wolf, De- Palma, Patiño, Uribe and Carnicero define these as injuries caused by secondary missiles originating from the bomb or surroundings. Saukko considers secondary injuries as those produced by structural collapse and places injuries caused by secondary missiles originating from the bomb or surroundings in a separate category, without specifying the method of differentiation. Furthermore, Carnicero includes thermal, chemical and nervous traumas, while Uribe includes thermal, chemical and mechanical traumas, accompanied by cerebral and neurological impact.
Tertiary injuries: These are defined by Wolf, Uribe, Patiño, the NCIPC and DePalma as a result of the displacement of the body by the blast wind. Wolf states that they are injuries of inertia and stretching that occur similarly to the deceleration effect in traffic accidents. The classifications of the NCIR and DePalma include fractures and traumatic amputations. Carnicero, Crane and Saukko do not consider them at all.
Quaternary injuries: in the classifications of the NCIPC, DePalma and Wolf, these are considered as any injuries caused by rupture and illnesses or conditions that are not described as primary, secondary or tertiary injuries. Uribe, on the other hand, calls them mixed injuries. Therefore, injuries are grouped by burns and crushing, closed and open brain injury, intoxication caused by gases, respiratory problems, angina, hyperglycemia and hypertension. Carnicero, Patiño, Crane and Saukko don’t consider them at all.
For additional clarification, a synoptic and comparative chart is provided of the eight classifications:
The classifications of Crane and Saukko are not included in the table because they use a different framework described as follows:
Crane’s Classification:
A. Total destruction of the victim.
B. Injuries due to explosives (body with multiple spots, abrasions and lacerations between 1 and 3 cm)
C. Injuries due to bomb fragments (secondary missiles)
D. Injuries due to the collapse of buildings or structural components.
E. Burns.
F. Blast injuries.
Saukko’s Classification:
A. Effects of the blast wave.
B. Secondary projectiles of an explosive device.
C. Secondary projectiles of the surroundings.
D. Burns caused by hot gas or incandescent objects.
E. Injuries caused by fallen structures, beams and displaced furniture in an explosion
|
Classification/ category |
NCIPC |
De Palma |
Wolf |
Uribe |
Carnicero |
OIM |
Patiño |
|
Primary: gas-filled structures (lungs and Gitract) and middle ear |
Yes, and others |
Yes, and others |
Yes, and others |
Yes, and others |
Yes, and others |
Yes |
Yes |
|
Secondary: secondary projectiles |
Yes |
Yes |
Yes |
Yes, and others |
Yes, and others |
Yes |
Yes |
|
Tertiary: displacement trauma and structural collapse |
Yes, and others |
Yes |
Yes |
Yes |
No |
Yes |
Yes |
|
Quaternary: injuries related to the explosion, different from aforementioned conditions. |
Yes |
Yes |
Yes, and psychological trauma |
Yes, and others |
No |
Yes, and others |
No |
|
Quinary |
No |
No |
Hyperinflammatory state |
No |
No |
“Dirtybombs” and others |
No |
|
Burns |
No |
No |
No |
No |
No |
|
Flash |
|
Crushing |
No |
No |
No |
No |
No |
|
Yes |
|
Inhalation of smoke or toxic gases |
No |
No |
No |
No |
No |
|
Yes |
|
Emotional shock |
No |
No |
No |
No |
No |
|
Yes |
Table 1. Comparison of classifications.
Source: I. (1-5,13,14).
DISCREPANCIES AMONG AUTHORS OF CLASSIFICATIONS
Injuries such as the amputation of extremities are not considered as primary lesions by Urbine, Hull, Cooper (19) and Marín, although the latter two state that traumatic amputations of the extremities are caused by shock wave. Likewise, Guermazi consider the injuries to extremities of the victims of the Boston marathon bombing in 2013 as primary injuries.
Ritenour et al. and Cernak (20) state that compartment syndrome can occur in extremities that don’t appear to be injured during an explosion, raising the possibility that they are a product of the force of the shock wave, which has not been contemplated by other authors.
Villalaín (21) mentions an additional category characterized by the absence of external injuries but with generalized capillary hemorrhages, (in particular thoracic-abdominal, pulmonary and pleural), aortic ruptures, fat and air embolisms, and up to 70% quantity of carboxyhemoglobin. This categorization has not been considered by other authors.
Armstrong et al. (22) are the only ones that consider subarachnoid hemorrhages, edema and diffuse axonal injury as primary injuries and explain that they are caused by the excess pressure produced by a blast wave.
Within the category of primary injuries, Carnicero includes the fragmentation and projection of the body, generalized blast and other primary injuries to hollow or solid organs; Crane and Saukko consider them as the total destruction of a victim. These injuries are not included by NCDC, Wolf, DePalma, Patiño nor Uribe.
Saukko, in his classification, separates injuries caused by secondary missiles originating from the bomb and those originating from the surroundings, without specifying the means of differentiation. The other authors do not make this difference.
As for secondary injuries, Carnicero groups together all those that are not primary, which includes the so-called mechanical, thermal, chemical and neuro-psychic injuries; this author does not include the tertiary, quaternary, and quinary categories of the other authors.
The definition of quaternary injuries used by the NCIPC, DePalma and Wolf as those that are not primary, secondary or tertiary but nonetheless related to the explosion is not considered by the other authors.
Other differences are as follows: the NCIPIC includes open or closed encephalic injuries in the category of tertiary or quaternary injuries, without establishing a clear difference between them; Patiño outlines 7 categories, with the first 3 corresponding to primary, secondary and tertiary injuries in the classifications of NCIPC, DePalma, Wolf and Uribe. The others are categories used only by this author. Crane describes a category as blast injuries not considered in other classifications; likewise, Saukko places burns in a separate category. Quinary injuries such as hyper-inflammatory reactions of survivors and injuries with multi-dimensional patterns, defined by Kluger (23), are only considered by Wolf and OIM.
PROPOSAL OF A NEW CLASSIFICATION FOR FORENSIC USE
We put forth a new system of classification that allows for the grouping of anatomical-pathological injuries in a systematic and documented way that will be of great use to doctors in diagnosis and evaluation in forensic pathology.
To clarify, the categories of moral, psychosocial and psychological harm have not been taken into account in this proposal because it is limited to physical bodily damage, which is the pillar of medical-forensic thought in autopsies. Therefore, no aspects related to the mental health of survivors have been included.
The Bogotá Classification categorizes injuries according to the phases of a blast: firstly, the effects of shock wave, secondly, the injuries caused by propulsion of secondary missiles, thirdly, the injuries produced by the projection of animated bodies and the collapse of non-animated bodies and fourthly, injuries that occur with later onset and injuries related to pre-existing conditions.
The proposal emphasizes the categorization of primary injuries, grouping together all the injuries caused by blast wave, which refers to both generalized body injuries and those accepted by all or only a few authors. This grouping is important since it includes injuries that explain tissue loss and other traumas that are present due to proximity to the center of the blast and the destructive power of the explosive agent.
The Bogotá Classification is organized as follows.
A. Injuries due to explosive wave (primary or blast)
Blast wave injuries are classified as those caused by the path of the wave through the body and the subsequent destruction associated with this mechanism, without any particular relation to air-liquid/solid interface. Injuries include as follows:
1. Generalized injuries described in the literature as bodily disintegration and generalized damage to the body without disintegration. These injuries cause great bodily harm and instant death (whole or partial cadavers recovered at the scene).
2. Organ injuries with air/liquid or solid/ liquid interface: lungs, ears, GI tract, facial fractures affecting the paranasal sinuses and cardiac rupture.
3. Amputations and fractures of the extremities produced by blast wave (described by Uribe, Guermazi, Hull and Marían) due to proximity to the explosion.
4. Burns caused by heat or radiation, commonly known as flash burns.
5. Injuries to solid organs such as subarachnoid hemorrhages, diffuse axonal injury, contusions and hemorrhages of unrelated internal organs and external injuries with blunt or penetrating trauma. Muscular and vascular injuries are also included here with or without compartmental syndrome, as described by Wolf.
B. Secondary injuries
These are caused by secondary missiles projected by the blast wave as either bomb fragments or flying debris from the surroundings. They are generally small injuries such as abrasions, hematomas and lacerations of tissues with fragments found in the body.
C. Tertiary injuries
These injuries are related to the propulsion of the body through the air and include traumas caused by acceleration-deceleration and/ or secondary crushing due to structural collapse. These consist of blunt traumas and are generally severe.
D. Quaternary injuries
These injuries are caused by events triggered by the explosion after the blast wave and destruction of bodies and objects. This category includes fires that cause burns and damage due to the inhalation of toxic gas and smoke, medical complications of injuries initially caused by the blast, the exacerbation of pre-existing conditions, and infections caused by “dirty bombs” or radiation (24). Quinary and multidimensional injuries are included in this category, which are identified in the clinical setting and require a period of survival.
CASE REPORT
Background
“Potato bombs”, as they are commonly known in Colombia, are improvised explosive devices created with the purpose of producing a big rumbling noise, though in some cases are also used as a weapon that mutilates extremities and can be fatal (25). The bombs use an impact or contact mechanism and are made with potassium chloride (the combustible product), sulfur and powdered aluminium (both are inflammable solids with the capacity to produce an explosion with an increase in temperature), aluminium paper (the container), and a stone that pulverizes and sprays upon impact. Nails and knives that act as shrapnel are sometimes included.
In a neighborhood in Bogotá, in the early hours of the morning, an explosion occurred that affected 109 adults and 51 children, according to a report of the Fondo de Atención y Prevención de Emergencias (Fund for the Attendance and Prevention of Emergencies)1 made to the newspaper El Espectador (26). This report states that the incident occurred when a group of 4 students - 3 men and 1 woman between 19 and 24 years of age - were handling 10 kilos of explosives to fabricate an improvised explosive device under the influence of alcohol. There was extensive material damage, as the walls of the home where the incident occurred (on the third floor of a residential compound) collapsed and a fire broke out, which firefighters later extinguished. Structural damages were incurred to approximately 65 homes and 25 vehicles in the neighborhood (27-30); the facades of three homes were also destroyed with damages to windows and walls.
Approach
In the early morning, 3 cadavers were brought in to the National Institute of Legal Medicine and Forensic Sciences in Bogotá. According to the information available, one person died at the scene and the other three were relocated to medical centers. Two of them later died and one survived.
Before conducting an autopsy of the 3 corpses, an approach was planned based on the methodological guidelines for medico-legal autopsies in cases of death resulting from blast injuries (Guidelines for the procedures of medico-legal autopsies, second edition). The procedures for identifying corpses were also followed (Manual for the identification of cadavers in forensic practice and the Manual for the practice of medical-legal autopsies)2, and an approach was planned for the the individualization of body parts and the collection of samples for further laboratory examination.
Detailed descriptions of the injuries of the individuals (named 1, 2, and 3) were made. The injuries were then classified according to the parameters established by the National Center for Injury Prevention and Control (NCIPC). Samples were taken and reports were written, and the injuries were subsequently reclassified according to the new classification proposal presented here and compared with classification systems of other authors.
Results
• The 3 cadavers were definitively identified using fingerprint data as a woman aged 24 and two men aged 20 and 22.
• The causes of death of the three people were found to be directly related to the explosion.
• The time of death was established as early morning, according to the available information of the incident.
• The three cadavers presented with blunt trauma caused by the blast wave and burns that compromised their bodies extensively. The injuries were characterized as typical injuries caused by explosive devices, along with explosive blast trauma, burns, and blunt and penetrating trauma.
• Cadaver 1 sustained the most burn injuries while 2 and 3 presented predominantly blast injuries and multiple blunt traumas.
Presentation of injuries involved in the case
1. Lamellar subserosal hematomas in hollow abdominal viscera (colon) in all 3 cadavers.
2. Bilateral globe rupture in two of the bodies.
3. Pulmonary hemorrhages in all 3 individuals.
4. Injury in the left forearm in individual 2 from a wooden shard measuring 2.5 x 0.5 cm as a missile or secondary projectile.
5. Lacerations, fractures and avulsion of hand tissue.
6. Fracture compromising the paranasal sinuses: in individuals 2 and 3, fractures of the middle part of the face compromising the glabella, malar and maxillary bones, orbits and nose.
7. Jaw fracture in left horizontal line corresponding to a fracture of the lower third of the face.
8. Subarachnoid hemorrhage in patches of the surfaces of the brain.
9. Hemorrhagic contusions at the base of the frontal lobes caused by frontal cranial fossa fractures.
The hemorrhages in Figure 10 are related to the cranial fractures in Figure 11.
10. Deceleration injuries: adventitious hematoma of the descending thoracic aorta, along with subpleural hemorrhage in the posterior wall and thoracic paravertebral space
11. Rupture of right atrium documented in individual 1.
12. Presence of flash burns in the face, neck, anterior thorax and forearms of individual 2 (female), who, at the time of the incident, was wearing a sleeveless shirt.
13. Extensive burns leading to 90% carbonization of the body.

Fig 1. Lamellar subserosal hematomas typical of blast injuries, individual 2.
Source: INML/CF.

Fig 2. Bilateral globe rupture in two of the bodies.
Source: INML/CF.
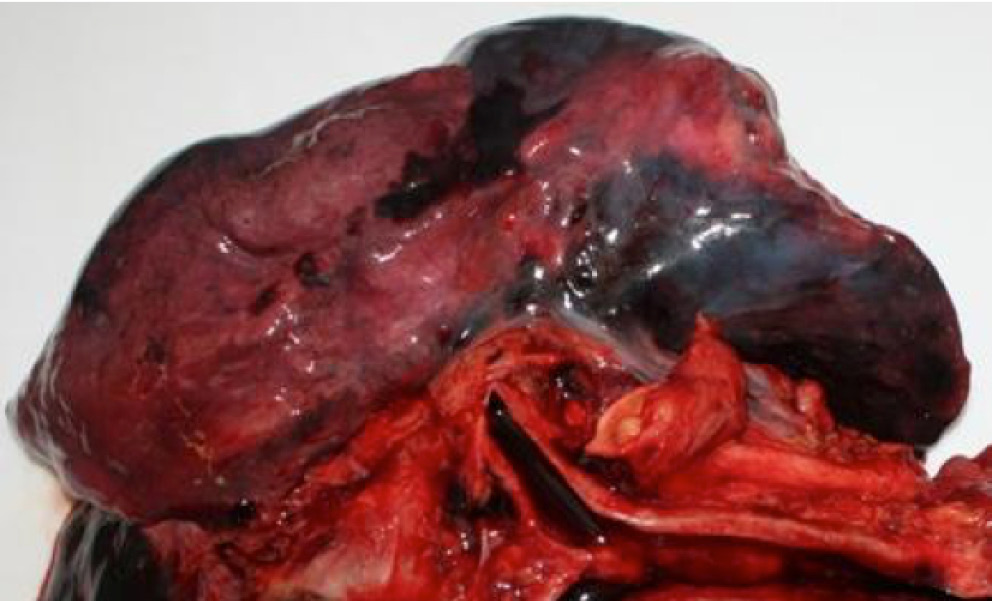
Fig 3. Pulmonary hemorrhages in subserosal and intraparenchymal areas, compromising all lobes, individual 3.
Source: INML/CF.

Fig 4. X-Ray of left superior extremity with opaque mass (see arrow) corresponding to a secondary projectile, individual 2.
Source: INML/CF.

Fig 5. Partial avulsion of the right hand, individual 2..
Source: INML/CF.

Fig 6. Partial destruction of the left hand with multiple fractures, lacerations of the skin, muscles, tendons and veins, and loss of soft tissue and bone fragments, individual 3.
Source: INML/CF.
Following this initial classification, the injuries were then categorized according to the Bogotá classification and compared with other classification systems:
This case deals with blast injuries of people in close proximity to an explosive device that was handled in a confined space. The findings of the autopsy are concordant with this view since the bodies display signs of multiple primary injuries.
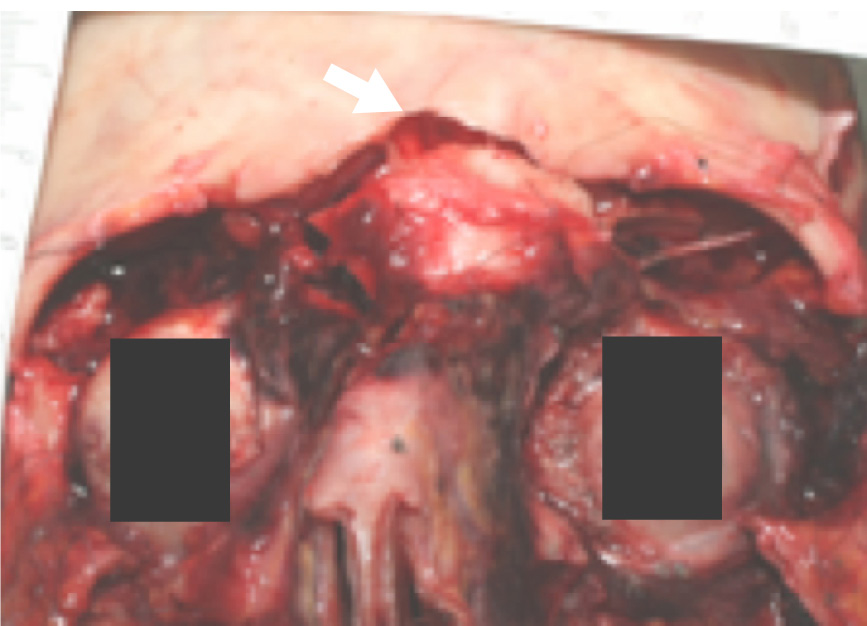
Fig 7. Dissection of the face showing total displaced fracture of the glabella and frontal and nasal bones, individual 2.
Source: INML/CF.

Fig 8. Total and displaced fracture of the maxillary line, individual 2.
Source: INML/CF.

Fig 9. View of the convex surfaces of the brain hemispheres with lamellar subarachnoid hemorrhages most prominent in the left occipital lobe and in the juncture of cerebellar lobes (see arrows), individual 3.
Source: INML/CF.
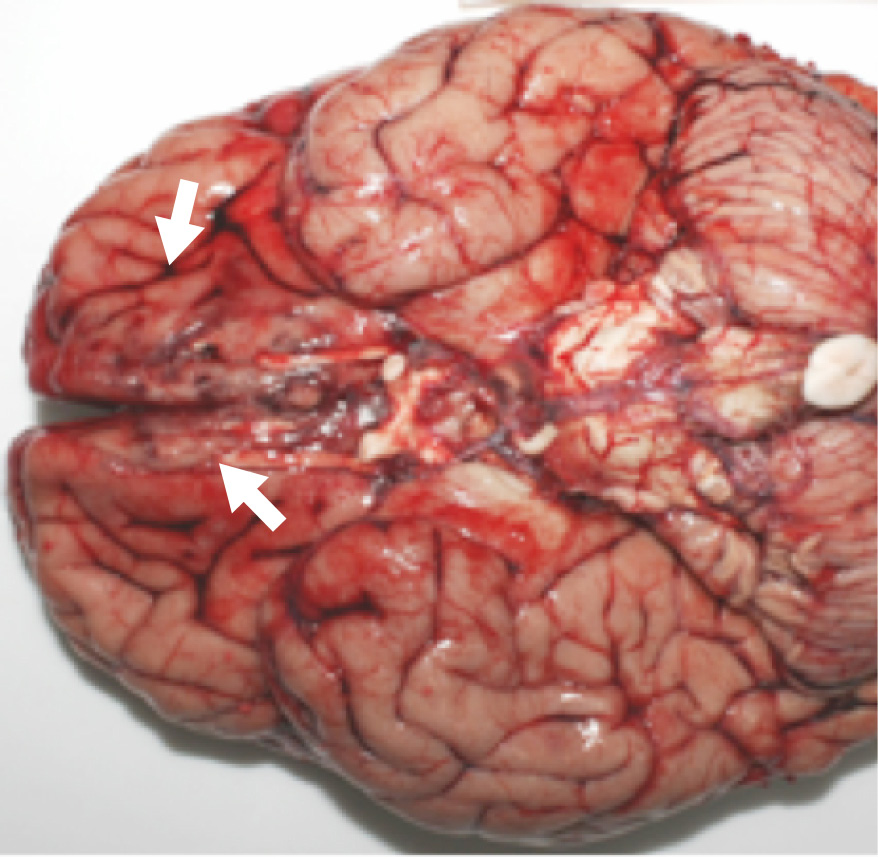
Fig 10. View of the base of the brain with hemorrhagic contusions in medial areas at the base of frontal lobes (see arrows), individual 2.
Source: INML/CF.

Fig 11. Cranial base with total and displaced fractures in the frontal fossa, individual 2.
Source: INML/CF.
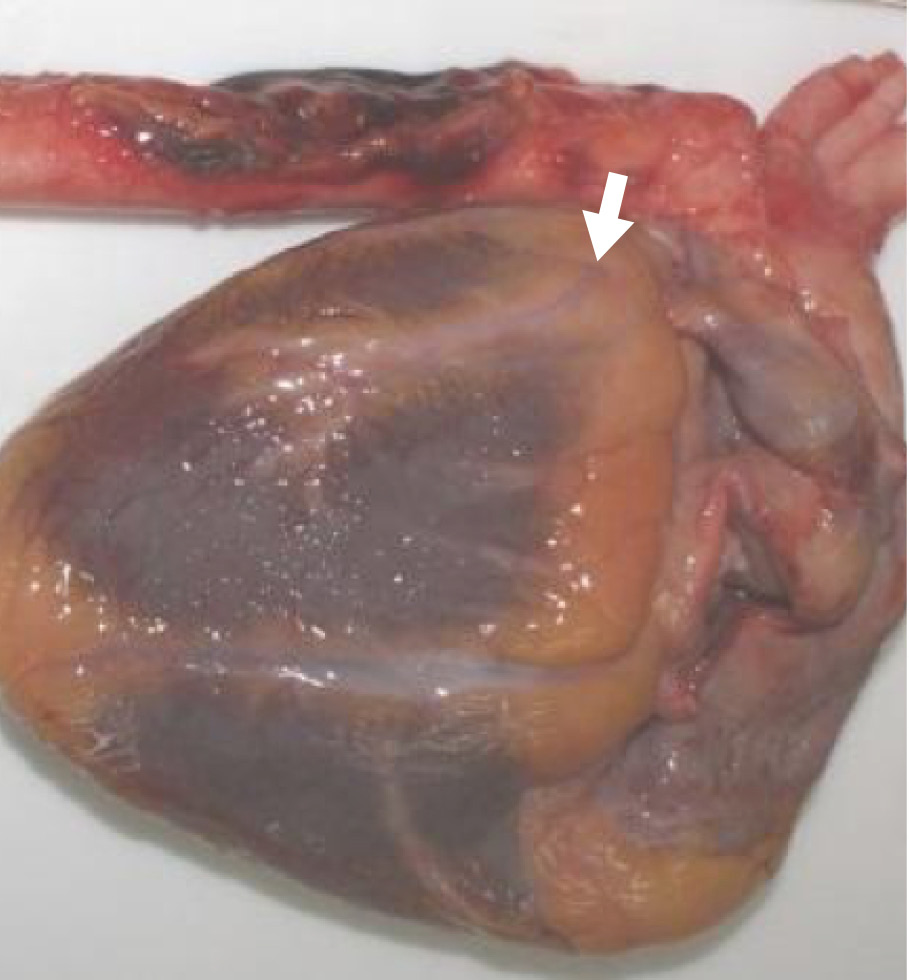
Fig 12. Posterior view of the heart with aortic arch and descending aorta, showing a hemorrhage in the location where the aorta attaches onto the spinal column, individual 2.
Source: INML/CF.

Fig 13. Thoracic cavity with lamellar subpleural hemorrhage in paravertebral areas, adjacent to the descending aorta, individual 2.
Source: INML/CF.

Fig 14. Lateral view of the upper third and face, showing uniform second-degree burns, mainly in areas that were not covered by clothing, individual 2.
Source: INML/CF.

Fig 15. Changes to the skin incurred by carbonization, hyperextension and disruption (see arrows), individual 1.
Source: INML/CF.
The hemorrhages of the lungs and colon indicate that the blast crossed through the bodies. In this case, the individuals were very near to the center of explosion and being in a confined space, received both the expansion blast and the reflected blast. Wolf explains that abdominal injuries are more common in explosions under water or in confined spaces.
Likewise, flash burns can be explained by the proximity to the center of the blast; Saukko mentions that this type of burn only affects people in proximity, unless the device is massive.
The avulsion of hand tissue indicates proximity to the explosive device.
CONCLUSION
The study of this case led to a literature review, searching for a classification system that would allow for the organization and approach of blast injury cases. It was found that the classifications in question either frame the study in clinical terms focusing on surviving patients or present injuries of both survivors and the deceased in a non-systematic way. This lack of homogeneity made it difficult to name the injuries found in the forensic case presented, which in turn led to the necessity of creating a new classification proposal to classify injuries of cadavers in an organized way.
|
INJURY |
Bogotá |
NC PIC |
De Palma |
Wolf |
Uribe |
Carnicero |
OIM |
Patiño |
Crane |
Saukko |
|
Subserosal hematomas of the colon |
1st |
1st |
1st |
1st |
1st |
1st |
1st |
1st |
Blast |
Blast |
|
Globe rupture |
1st |
1st |
1st |
1st |
|
1st |
|
|
- |
- |
|
Pulmonary hemorrhage |
1st |
1st |
1st |
1st |
1st |
1st |
1st |
1st |
Blast |
Blast |
|
Secondary projectile |
2nd |
2nd |
2nd |
2nd |
2nd |
2nd |
2nd |
2nd |
Other |
Other |
|
Hand avulsion |
1st |
3rd |
3rd |
1st |
3rd |
2nd |
1st |
1st |
- |
Blast |
|
Paranasal sinus fracture |
1st |
3rd |
3rd |
1st |
3rd |
2nd |
1st |
3rd |
- |
- |
|
Mandibular fracture |
3rd |
3rd |
3rd |
3rd |
3rd |
2nd |
3rd |
3rd |
Other |
Other |
|
Subarachnoid hemorrhage |
1st |
3rd/4th |
3rd |
3rd |
3rd |
2nd |
3rd |
1st |
- |
- |
|
Cerebral contusion |
3rd |
3rd/4th |
3rd |
3rd |
3rd |
2nd |
3rd |
1st |
Other |
Other |
|
Deceleration injury |
3rd |
3rd |
3rd |
3rd |
3rd |
2nd |
3rd |
3rd |
Other |
- |
|
Rupture of right atrium |
1st |
3rd |
3rd |
1st |
3rd |
2nd |
3rd |
3rd |
- |
- |
|
Flash burn |
1st |
4th |
4th |
1st |
4th |
2nd |
4th |
Other |
Other |
Blast |
|
Carbonization |
4th |
4th |
4th |
4th |
4th |
2nd |
4th |
- |
- |
Other |
Table 2. Injuries according to the classifications.
Source: Authors.
The severity of blast injuries varies in relation to the power and quantity of the explosive, open or confined space, and the proximity of the victim to the center of explosion. Given these characteristics, it is important to have a classification that highlights the groupings of all the documented injuries as primary to direct them towards a correlation with the scene and center of explosion
REFERENCES
1. 1. National Center for Injury Prevention and Control, Office of Noncommunicable Diseases, Injury and Environmental Health. Explosions and Blast injuries: A primer for Clinicians. Atlanta: Centers for Disease Control and Prevention; 2006 [cited 2014 Aug 1]. Available from: http:// goo.gl/AxSOxn.
2. 2. DePalma RG, Burris DG, Champion HR, Hodgson MJ. Blast injuries. N. Engl. J. Med. 2005;352(13):1335-42. http://doi.org/c6pfcr.
3. 3. Wolf SJ, Bebarta VS, Bonnett CJ, Pons PT, Cantrill SV. Blast injuries. Lancet. 2009;374(9687):405- 15. http://doi.org/fcfnw2.
4. 4. Carnicero-Giménez de Azcárate MA, Baigorri- Soler MC. Muerte por explosión: cuestiones y sistemática médico-forenses. Cuad. Med. Forense. 2002;27:39-52. http://doi.org/ct8g7t.
5. 5. Patiño JF. Trauma por explosiones y bombas. Bogotá, D.C.: Oficina de Recursos Educacionales-FEPAFEM; 2014 [updated 2014 Feb 28; cited 2015 Sep 17]. Available from: http://goo.gl/jLcFTH.
6. 6. Crane J. Violence associated with civil disturbance. In: Mason JK, Purdue BN, editors. The pathology of trauma. Londres: Arnold; 2000. p. 73-88.
7. 7. Saukko P, Knight B. Gumshot and explosion deaths. In: Knight’s Forensic Pathology. 3th ed. London: CRC Press; 2004 [cited 2015 Sep 17]. p. 245-280. Available from: http://goo.gl/O0da6Z.
8. 8. Gruss E. A correction for primary blast injury criteria. J. Trauma. 2006;60(6):1284-9. http:// doi.org/cbmhxn.
9. 9. Marín L. Lesiones por explosivos. Revista Médica de Risaralda. 2000 [cited 2015 Sep 17];6(1):18- 23. Available from: http://goo.gl/KFd4SQ.
10. 10. Bernal GE. Síndrome por explosión (Blast injury). Zaragoza: XVIII Jornadas Sanitarias Ayuntamiento de Zaragoza 2008; 2008.
11. 11. Schardin H. The physical principles of the effects of a detonation. In: Office of the Surgeon General. German aviation medicine, World War II. Washington, D.C.: Department of the US Air Force; 1950. p. 1207-1224.
12. 12. Benzinger, T. 1950. Physiological effects of blast in air and water. In: Office of the Surgeon General. German Aviation Medicine, World War II. Volume 2. Washington, D.C.: Department of the Air Force. p. 1225-1229.
13. 13. Uribe-Moreno R. Trauma por explosiones y bombas. In: Ministerio de Protección Social, Federación Panamericana de Asociaciones de Facultades (Escuelas) de Medicina FEDEPAM. Guía para manejo de urgencias. Tomo I. 3th ed. Bogotá, D.C.: Ministerio de la Protección Social; 2009. p. 265-270.
14. 14. Institute of Medicine of the Natinal Academes. Gulf War and health, volume 9: Long-term effects of blast exposures. Washington, D.C.: National Academies Press; 2014.
15. 15. Guermazi A, Daichi H, Smith SE, Palmer W, Katz JN. Imaging of Blast Injuries to the lower extremities sustained in the Boston marathon bombing. Arthritis Care Res. 2013;65(12):1893- 8. http://doi.org/7rg.
16. 16. Ritenour AE, Dorlac WC, Fang R, Woods T, Jenkins DH, Flaherty SF, et al. Complications after fasciotomy revision and delayed compartment relase in combat patients. J. Trauma. 2008;64(suppl 2):S153-61. http://doi.org/bvmk6v.
17. 17. Rosenfeld JV, McFarlane AC, Bragge P, Armonda RA, Grimes JB, Ling GS. Blast-related traumatic brain injury. Lancet Neurol. 2013;12(9):882-93. http://doi.org/f2nbg6.
18. 18. Crabtree J. Terrorist Homicide Bombing: A Primer for Preparation. J. Burn. Care Res. 2006;27(5):576- 88. http://doi.org/bwpbp3.
19. 19. Hull JB, Cooper GJ. Pattern and mechanism of traumatic amputation by explosive blast. J. Trauma. 1996;40(Suppl 3):S198-205. http://doi.org/c3vxgr.
20. 20. Cernak I, Savic J, Ignjatovic D, Jevtic M. Blast injury from explosive munitions. J. Trauma. 1999;47(1):96- 103. http://doi.org/bdj96x.
21. 21. Villalaín-Blanco JD. Lesiones por explosivos. In: Centro de Estudios Judiciales. Seminarios sobre delitos contra las personas. Madrid: Ministerio de Justicia, Centro de publicaciones; 1990. p. 113-138.
22. 22. Armstrong JH, Sullivent EE, Sasser SM. Blast Injuries From Bombings: What Craniofacial and Maxillofacial Surgeons Need to Know. J. Craniofac. Surg. 2010;21(4):954-9. http://doi.org/fpm8g9.
23. 23. Kluger Y, Peleg K, Daniel-Aharonson L, Mayo A; Israeli Trauma Group. The special injury pattern in terrorist bombings. J. Am. Coll. Surg. 2004;199(6):875-9. http://doi.org/c8k6tc.
24. 24. Born C, Briggs S, Ciraulo D, Frykberg E, Hammond J, Hirshberg A, et al. Catástrofes y víctimas en masa: II. Agentes explosivos, biológicos, químicos y nucleares. J. Am. Acad. Orthop. Surg. 2007;6:7.
25. 25. Cepeda S. El peligroso mundo de las ‘papas bomba’. DONJUAN. 2012 Apr 12. [cited 2014 Jul 20]. Available from: http://goo.gl/QLgVGg.
26. 26. Explosión en Suba se debió a fabricación de papas bomba. El Espectador. 2012 Mar 25 [cited 2014 Jul 20]. Available from. http://goo.gl/gTRGTL.
27. 27. En Medicina Legal permanecen los cuerpos de los universitarios muertos por explosión de ‘papas-bomba’. Caracol Radio. 2012 Mar 25 [cited 2015 Sep 17]. Available from: http://goo.gl/IcH03G.
28. 28. Tres estudiantes murieron por explosión en Suba mientras fabricaban papas bomba. La F.m. noticias. 2012 Mar 25 [cited 2015 Sep 17] Available from: http://goo.gl/sBj17W.
29. 29. Explosión en Suba se debió a fabricación de papas bomba. Correo confidencial. 2012 Mar 25 [cited 2015 Sep 17]. Available from: http://goo.gl/gJC00d.
30. 30. Mueren estudiantes cuando fabricaban papas bomba. Vanguardia. 2012 Mar 26 [cited 2015 Sep 17]. Available from: http://goo.gl/0f20v3