


Publicado
Adherence to antiretroviral treatment and associated factors in people living with HIV/AIDS in Quindío, Colombia
Adhesión al tratamiento antirretroviral y factores asociados en personas viviendo con VIH/sida en Quindío, Colombia
DOI:
https://doi.org/10.15446/revfacmed.v65n3.55535Palabras clave:
HIV, Antiretroviral Therapy Highly Active, Medication Adherence, Depression, Anxiety, Social Support (en)VIH, Terapia antirretroviral altamente activa, Adhesión al tratamiento, Depresión, Ansiedad, Apoyo social (es)
Descargas
Introduction: HIV/AIDS is a chronic disease; therefore, recognizing which factors favor adherence to antiretroviral treatment is necessary.
Objective: To determine the association between adherence to antiretroviral treatment and depression, anxiety, perception of social support and sociodemographic variables in people living with HIV/AIDS in Quindío, Colombia.
Materials and methods: An observational, cross-sectional study was performed in an intentional sample of 70 adults, who were applied the Morisky-Green questionnaire, the Beck Depression Inventory, the Beck Anxiety Inventory, the Medical Outcomes Study (MOS) Social Support Survey, and a sociodemographic survey. Univariate and bivariate analyzes were performed by calculating the odds ratio to determine association (p<0.05).
Results: 57.1% of the participants reported low adherence to treatment, 30% had moderate or severe depressive symptoms, 71.4% scored minimal or mild anxiety levels, and 77.1% had a low perception of social support. A statistical association between depression (high levels tripled the risk of non-adherence) and self-report on how treatment is followed (excellent or good self-report increased by five times the probability of adherence) was found.
Conclusion: Depression and self-report on compliance were associated with adherence to antiretroviral therapy. A comprehensive study on the perception of social support and cognitive variables, such as self-efficacy and risk perception, is highly recommended for people living with HIV/AIDS.
Introducción. El VIH/sida es una enfermedad crónica, por ello es necesario reconocer qué factores favorecen la adhesión al tratamiento antirretroviral.
Objetivo. Determinar la asociación entre adhesión al tratamiento antirretroviral y depresión, ansiedad, percepción de apoyo social y variables sociodemográficas en personas viviendo con VIH/sida en Quindío, Colombia.
Materiales y métodos. Se realizó un estudio observacional analítico de tipo transversal en una muestra intencional de 70 adultos, a quienes se les aplicó el cuestionario autorreferido de Morisky-Green, el Inventario de Depresión de Beck, el Inventario de Ansiedad de Beck, el cuestionario MOS (Medical Outcomes Study) de Apoyo Social y una encuesta sociodemográfica. Se realizaron análisis univariados y bivariados calculando Odds Ratio para determinar asociación (p<0.05).
Resultados. 57.1% de los participantes reportó poca adhesión al tratamiento, 30% presentó síntomas depresivos moderados o graves, 71.4% puntuó niveles mínimos o leves de ansiedad y 77.1% tuvo baja percepción de apoyo social. Se encontró asociación estadística entre depresión —niveles altos triplicaron el riesgo de no adhesión— y autoevaluación de la manera como se sigue el tratamiento —excelente o buena aumentó cinco veces la probabilidad de adhesión—.
Conclusión. La depresión y la autoevaluación del cumplimiento se asociaron con adhesión al tratamiento antirretroviral. Se sugiere profundizar el estudio de la percepción de apoyo social y variables cognitivas, como la autoeficacia y percepción de riesgo, en personas que viven con VIH/sida.
Original research
DOI: https://doi.org/10.15446/revfacmed.v65n3.55535
Adherence to antiretroviral treatment and associated factors
in people living with HIV/AIDS in Quindío, Colombia
Adhesión al tratamiento antirretroviral y factores asociados en personas
viviendo con VIH/sida en Quindío, Colombia
Received: 02/02/2016. Accepted: 16/06/2016.
Deisy Viviana Cardona-Duque1 • Óscar Adolfo Medina-Pérez2 • Sandra Milena Herrera-Castaño3 • Paula Andrea Orozco-Gómez3
1 Universidad de San Buenaventura Medellín - Armenia Campus - Faculty of Psychology - Behavioral and Organizational Health
Research Group - Armenia - Colombia.
2 Universidad Nacional Abierta y a Distancia - Medellín Campus - School of Social Sciences, Arts and Humanities - Subject, Mind and Community Research Group - Medellín - Colombia.
3 Hospital Departamental Universitario del Quindío San Juan de Dios - Department of Teaching and Research - Hospital Management Research Group - Armenia - Colombia.
Corresponding author: Deisy Viviana Cardona-Duque. Behavioral and Organizational Health Research Group, Faculty of Psicology,
Universidad de San Buenaventura Medellín. Carrera 13 No. 1A-50 norte. Phone number: +57 6 7313596. Armenia. Colombia.
Email: deisy.cardona@tau.usbmed.edu.co.
| Abstract |
Introduction: HIV/AIDS is a chronic disease; therefore, recognizing which factors favor adherence to antiretroviral treatment is necessary.
Objective: To determine the association between adherence to antiretroviral treatment and depression, anxiety, perception of social support and sociodemographic variables in people living with HIV/AIDS in Quindío, Colombia.
Materials and methods: An observational, cross-sectional study was performed in an intentional sample of 70 adults, who were applied the Morisky-Green questionnaire, the Beck Depression Inventory, the Beck Anxiety Inventory, the Medical Outcomes Study (MOS) Social Support Survey, and a sociodemographic survey. Univariate and bivariate analyzes were performed by calculating the odds ratio to determine association (p<0.05).
Results: 57.1% of the participants reported low adherence to treatment, 30% had moderate or severe depressive symptoms, 71.4% scored minimal or mild anxiety levels, and 77.1% had a low perception of social support. A statistical association between depression (high levels tripled the risk of non-adherence) and self-report on how treatment is followed (excellent or good self-report increased by five times the probability of adherence) was found.
Conclusion: Depression and self-report on compliance were associated with adherence to antiretroviral therapy. A comprehensive study on the perception of social support and cognitive variables, such as self-efficacy and risk perception, is highly recommended for people living with HIV/AIDS.
Keywords: HIV; Antiretroviral Therapy Highly Active; Medication Adherence; Depression; Anxiety; Social Support (MeSH).
Cardona-Duque DV, Medina-Pérez OA, Herrera-Castaño SM, Orozco-Gómez PA. Antiretroviral treatment adherence and associated factors in people living with HIV/aids in Quindío – Colombia. Rev. Fac. Med. 2017;65(3):403-10. English. doi: https://doi.org/10.15446/revfacmed.v65n3.55535.
| Resumen |
Introducción. El VIH/sida es una enfermedad crónica, por ello es necesario reconocer qué factores favorecen la adhesión al tratamiento antirretroviral.
Objetivo. Determinar la asociación entre adhesión al tratamiento antirretroviral y depresión, ansiedad, percepción de apoyo social y variables sociodemográficas en personas viviendo con VIH/sida en Quindío, Colombia.
Materiales y métodos. Se realizó un estudio observacional analítico de tipo transversal en una muestra intencional de 70 adultos, a quienes se les aplicó el cuestionario autorreferido de Morisky-Green, el Inventario de Depresión de Beck, el Inventario de Ansiedad de Beck, el cuestionario MOS (Medical Outcomes Study) de Apoyo Social y una encuesta sociodemográfica. Se realizaron análisis univariados y bivariados calculando Odds Ratio para determinar asociación (p<0.05).
Resultados. 57.1% de los participantes reportó poca adhesión al tratamiento, 30% presentó síntomas depresivos moderados o graves, 71.4% puntuó niveles mínimos o leves de ansiedad y 77.1% tuvo baja percepción de apoyo social. Se encontró asociación estadística entre depresión —niveles altos triplicaron el riesgo de no adhesión— y autoevaluación de la manera como se sigue el tratamiento —excelente o buena aumentó cinco veces la probabilidad de adhesión—.
Conclusión. La depresión y la autoevaluación del cumplimiento se asociaron con adhesión al tratamiento antirretroviral. Se sugiere profundizar el estudio de la percepción de apoyo social y variables cognitivas, como la autoeficacia y percepción de riesgo, en personas que viven con VIH/sida.
Palabras clave: VIH; Terapia antirretroviral altamente activa; Adhesión al tratamiento; Depresión; Ansiedad; Apoyo social (DeCS).
Cardona-Duque DV, Medina-Pérez OA, Herrera-Castaño SM, Orozco-Gómez PA. [Adhesión al tratamiento antirretroviral y factores asociados en personas viviendo con VIH/sida en Quindío, Colombia]. Rev. Fac. Med. 2017;65(3):403-10. English. doi: https://doi.org/10.15446/revfacmed.v65n3.55535.
Introduction
HIV is a public health concern worldwide. Since 2000, 38.1 million people have acquired the virus and 25.3 million have died from AIDS-related illnesses (1). In 2015, UNAIDS (2) reported an average of 34 to 39.8 million people living with HIV/AIDS (PLWHA) in the world; in Latin America, the figure ranges between 1.7 and 2.3 million. According to the same report, 17 million people had access to antiretroviral therapy (ART) in December 2015, while about 22 million people did not have access to treatment at all. About 28 million new cases could be avoided, if response to AIDS in low- and middle-income countries increases (3).
The Colombian Public Health Surveillance System reported 8 196 new PLWHA cases in 2012 (4), with the highest incidence in Barranquilla (50.6 cases per 100 000 inhabitants), Quindío (28.4 cases per 100 000 inhabitants), and Cartagena (37.6 cases per 100 000 inhabitants). In addition, 2 216 deaths associated with HIV/AIDS and a mortality rate of 4.76 per 100 000 inhabitants were reported. Quindío was one of the most affected departments by this epidemic (5).
HIV/AIDS is considered a chronic disease that involves multiple factors, since it has an impact on physical and mental functioning (6) and may affect self-concept and sense of life (7). This condition is a stressor that implicates psychological, physiological, social and economic aspects, therefore, it demands strategies that favor treatment and reduce threats to health. In this regard, the patient’s attitudes and coping techniques can influence the HIV infection process (8), which, in turn, demands changes in lifestyle to comply with therapeutic indications. This is known as adherence to treatment, and indicates the commitment and participation of the individual in self-care (9,10).
Although no consensus in the definition of treatment adherence has been achieved (also known as cooperation or therapeutic compliance), it is generally understood as a complex and multifactorial problem that transcends following closely medical instructions or prescriptions (9,11). As proposed by DiMatteo & DiNicola, and accepted by other researchers, adherence is an active process of voluntary collaboration established between the patient and the health personnel to carry out mutually agreed upon behaviors, in order to generate the desired therapeutic effect (10,12,13).
Piña-López & Sánchez-Sosa (14) suggest that adherence in PLWHA is determined by the frequency with which subjects develop behaviors to comply with the instructions provided by health personnel based on their own skills. Adherence behaviors are a consequence of the interaction between biological variables (HIV disease and other conditions) and psychological variables (interaction styles related to stress, abilities, motives and emotional states), which have effects on health, control and course of infection with HIV (11,14).
Different situations may affect adherence to treatment in chronic diseases, for example, the nature of the disease, the time of evolution, the expectation of treatment outcomes, the characteristics of the treatment, the habits and customs of the patient (15,16), the interaction with health professionals, the characteristics of the health institution (9), and psychological and social aspects such as coping strategies (6). Other important factors in HIV infection include its asymptomatic character in most cases, the amount of drugs supplied (antiretrovirals and those necessary for opportunistic diseases), social stigmatization, side effects of certain drugs, patient’s beliefs, affective states, perception of control over stressful life events, and the disease, among others (17,18).
Following the model of Sánchez-Sosa et al. (19), psychological variables such as depression, stress, anxiety, low motivation and lack of social support can contribute to the progression of the disease and reduce the quality of life of the affected patients.
Remor (20) reports low adherence in the presence of high levels of anxiety, stress, depression and poor social support. Piña-López et al. (21) and Piña-López et al. (22) report competencies, stress, motives, frustration, tolerance and ambiguity as predictors of adherence, which may vary according to the time of infection; also, Piña-López et al. (23) proposed that intermediate levels of stress and low levels of depression are favorable, and, finally, Piña-López et al. (24) add that associated psychological variables are affected by self-report on social competences.
Arrivillaga et al. have identified a correlation between anxiety and depression, as well as a perception of poor control over health and stressful life events in women living with HIV/AIDS, which affect their adherence and quality of life. Likewise, Arrivillaga et al. (26), Arrivillaga et al. (27) y Arrivillaga et al. (28) stress the role played by social and economic factors in the adherence to antiretroviral treatment (ART) by women. Social support is another key factor associated with better health results, adherence and quality of life in PLWHA (7,25,29-31).
In this regard, adherence to ART is a complex process, permeated by psychological and social factors of great relevance for the evolution, treatment and quality of life of PLWHA. These factors need to be further analyzed given the implications for public health that the lack of adherence to ART have, and to contribute to the enrichment of intervention programs. It is, therefore, pertinent to generate knowledge in this field, and specifically in one of the leading departments of morbidity and mortality caused by HIV/AIDS in Colombia. The aim of this study was to establish the association between adherence to antiretroviral therapy and depression, anxiety, perception of social support and sociodemographic variables in a group of PLWHA in Quindío, Colombia during 2015.
Methodology
This is an observational and analytical cross-sectional study, in which 70 PLWHA participated —men and women enrolled in an accompaniment program offered by a health institution in Quindío (Colombia). Some of them were hospitalized and others were attending medical and psychological follow-ups. Sampling was non-probabilistic, intentional, and selected taking into account as inclusion criteria HIV diagnosis, ART, being of legal age, no physical or mental conditions that would hinder understanding the instruments, will to participate in the study, and a signed informed consent.
A socio-demographic data survey was used for collecting information regarding age, sex, marital status, schooling, socioeconomic stratum and religion. In addition, variables related to the disease such as diagnosis time, perception of family support and understanding during the treatment, consumption of psychoactive substances (cigarettes, coca paste and/or marihuana), frequency of psychological therapy, and self-report on how treatment was followed were also investigated.
Adherence to ART was assessed using the Morisky-Green Scale (32), which reflects patient compliance with medication and has been used in different studies (33-36). This instrument consists of four questions with two response options (Yes/No); if the answer for any of these items is Yes, it means that the patient has failed and is reported as non-adherent.
To identify depressive symptoms and their severity, the Beck Depression Inventory (BDI) was applied; this is a 21-item scale that considers psychological-cognitive and somatic-vegetative aspects, which are evaluated based on affirmations selected by the individual. The scores range from 0 to 3, yielding a total number between 0 and 63. A score of 0 to 9 indicates absence of depression; 10 to 18, mild depression; 19 to 29, moderate depression, and from 30 onwards, severe depression (37,38).
On the other hand, the Beck Anxiety Inventory (BAI) was used to evaluate anxiety symptoms when investigating subjective, neurophysiological, autonomic and panic factors. This inventory is made up of 21 items, each with the following response options: 0-not at all; 1-slightly, it does not bother me much; 2-moderately, it was very unpleasant but I could bear it, and 3-severely, I could hardly bear it. In the Spanish version, the cut-off points are 0 to 7 for minimal anxiety, 8 to 15 for mild anxiety, 16 to 25 for moderate anxiety, and 26 to 63 for severe anxiety (39).
Perceived social support was assessed using the Medical Outcomes Study (MOS) questionnaire designed by Sherbourne and Stewart in 1991, and adapted to the Colombian population (40), which assesses structural support or size of the social network (item 1) and functional support (perception of support, items 2-19). Functional support is independent and multidimensional, and is composed of emotional/informative, tangible and affective social support and positive social interaction. The first question inquiries into the number of close friends and relatives. The remaining questions have answering options from 1 to 5 (never, rarely, sometimes, most of the time, always). The raw scores range from 19 to 95, and a higher score indicates greater perceived social support.
The study was supported by the Bioethics Committee of the Universidad de San Buenaventura Medellín. The instruments were codified and a route was established for channeling severe depression and anxiety cases or suicidal ideation in order to refer patients to specialists or appropriate care centers. Subsequently, the participants were contacted to be informed about the objectives and procedures of the study, and to request voluntary participation. An appointment was coordinated with those who accepted under certain conditions to ensure confidentiality.
The instruments were applied through an individual interview; prior informed consent was signed and participants were informed about the purpose of the study, voluntariness, confidentiality and non-remuneration, as well as about their right to abandon the study at any time. Individual results were returned to participants, and general results to the health institution. Lastly, the channeling route was activated in the necessary cases.
Data tabulation was performed in Microsoft Excel 2013, and the statistical analysis was made through SPSS version 21. Univariate and bivariate analyzes were performed. Central tendency, dispersion and position were evaluated as quantitative variables and, on the other hand, qualitative variables included absolute and relative frequencies. To determine the existence or non-existence of statistical association, the odds ratio (OR) was calculated and its confidence intervals and p values were deemed as significant when they were <0.05.
It should be noted that depression and anxiety variables were dichotomized for the analysis, and were reported as absent/mild depression, moderate/severe depression, and minimal/mild anxiety, moderate/severe anxiety. Regarding social support perception, the scores found in the first three quartiles were taken as low, and the ones in the last quartile were considered high. The socioeconomic stratum variable was analyzed based on the Colombian stratification, and was grouped into three categories: 0, 1 and 2, which included homeless population, low-low and low strata, and 3, 4 and 5 strata gathering middle-low, medium and medium-high strata.
Results
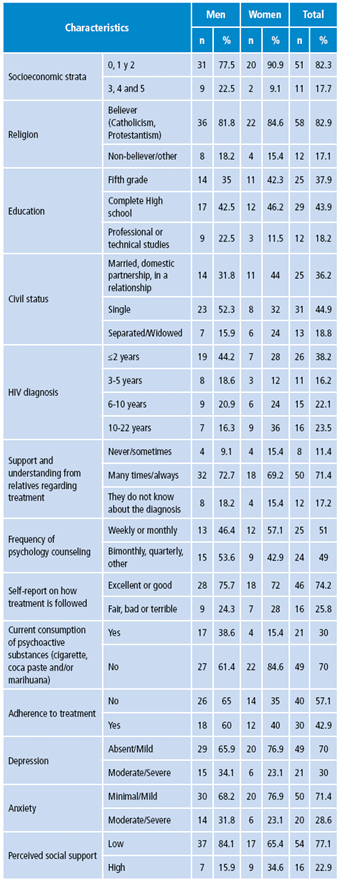
70 people, aged between 18 and 66 years, answered the survey; the average age was 38, with a standard deviation of 12 years. The highest age in 50% of the participants was 38, and the most frequent was 28. The highest proportions were found among men (64.5%), patients of socioeconomic strata 0, 1 and 2 (82.3%), catholics or protestants (82.9%), high school graduates (43.9%), and single (44.9%). 38.2% of the subjects were diagnosed two years or less before they participated in the study. Most of them (71.4%) reported feeling supported and understood by their relatives, and affirmed that they were receiving psychological therapy on a regular basis. 30% of the patients reported that they are currently using psychoactive substances.
57.1% of the patients did not show adherence to the pharmacological treatment, although most of them state that they are following it with excellent outcomes (74.2%). Regarding the psychological variables, absent or mild levels of depression were found in most participants; 30% scored moderate or severe depression. Moderate or severe levels of anxiety were observed in 28.6% of the cases, and the perception of little social support in 77.1% (Table 1).
Bivariate analysis
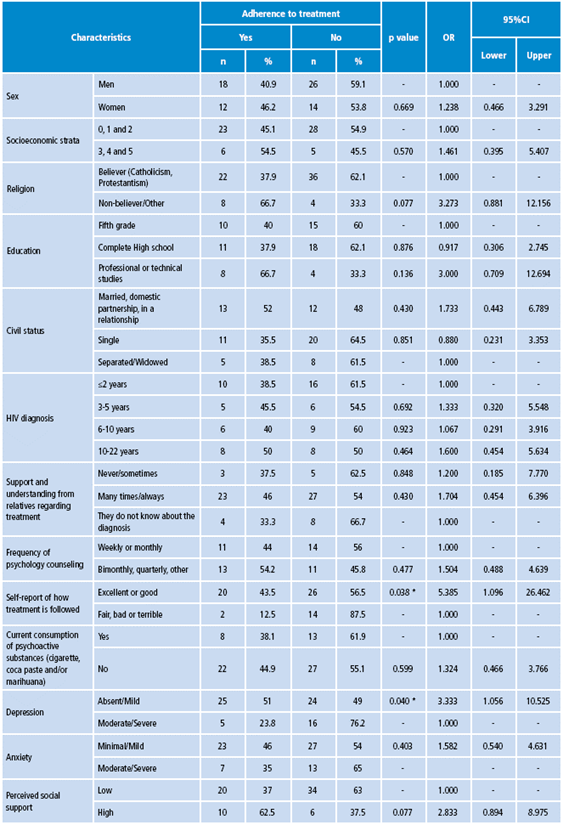
In order to determine some associations that would indicate possible factors related to ART adherence, a bivariate analysis was performed. Two of the evaluated variables had a statistically significant association with adherence: self-report on the way in which treatment was followed (p=0.038, OR=5.385, 95%CI: 1.096-26.46) and depression (p=0.040, OR=3.33; 95%CI: 1.056-10.52). The p-value found in the remaining variables was >0.05, although a higher proportion of adherence was observed in women, in people from socioeconomic strata 3 to 5, in those who have more than 10 years of diagnosis, in those who do not profess any religion, are married or in some kind of relationship, have technical or professional studies, who frequently or always feel support and understanding from their families, those who attend therapy periodically, who are not currently using any type of illegal substance, and those who have low levels of anxiety and perceive high levels of social support (Table 2).
Discussion
This study identified adherence to treatment in a group of PLWHA in Quindío and its association with psychological and social variables that may play a fundamental role in interventions with this population. An outstanding percentage of subjects showed poor adherence (57.1%), which is highly relevant since this situation may indicate how patients are coping with their condition and, at the same time, how their quality of life and their relatives or closed ones are being affected by it.
Lack of adherence to long-term treatment leads to personal, social, health and economic issues, as it generates a greater risk to health (relapses, onset or worsening of symptoms, evolution to late or severe phases of the disease, adverse effects, and resistance to medication), lower quality of life and well-being; higher rates of stress, interference with lifestyle or alterations in performance areas of patients and their relatives, and greater probability of increasing the demand for hospital and pharmaceutical resources (41).
Table 1. Percentage distribution of sociodemographic, family, health and psychological variables evaluated in people living with HIV/AIDS by sex. Quindío, Colombia. 2015.
|
Characteristics |
Men |
Women |
Total |
||||
|
n |
% |
n |
% |
n |
% |
||
|
Socioeconomic strata |
0, 1 y 2 |
31 |
77.5 |
20 |
90.9 |
51 |
82.3 |
|
3, 4 and 5 |
9 |
22.5 |
2 |
9.1 |
11 |
17.7 |
|
|
Religion |
Believer (Catholicism, Protestantism) |
36 |
81.8 |
22 |
84.6 |
58 |
82.9 |
|
Non-believer/other |
8 |
18.2 |
4 |
15.4 |
12 |
17.1 |
|
|
Education |
Fifth grade |
14 |
35 |
11 |
42.3 |
25 |
37.9 |
|
Complete High school |
17 |
42.5 |
12 |
46.2 |
29 |
43.9 |
|
|
Professional or technical studies |
9 |
22.5 |
3 |
11.5 |
12 |
18.2 |
|
|
Civil status |
Married, domestic partnership, in a relationship |
14 |
31.8 |
11 |
44 |
25 |
36.2 |
|
Single |
23 |
52.3 |
8 |
32 |
31 |
44.9 |
|
|
Separated/Widowed |
7 |
15.9 |
6 |
24 |
13 |
18.8 |
|
|
HIV diagnosis |
≤2 years |
19 |
44.2 |
7 |
28 |
26 |
38.2 |
|
3-5 years |
8 |
18.6 |
3 |
12 |
11 |
16.2 |
|
|
6-10 years |
9 |
20.9 |
6 |
24 |
15 |
22.1 |
|
|
10-22 years |
7 |
16.3 |
9 |
36 |
16 |
23.5 |
|
|
Support and understanding from relatives regarding treatment |
Never/sometimes |
4 |
9.1 |
4 |
15.4 |
8 |
11.4 |
|
Many times/always |
32 |
72.7 |
18 |
69.2 |
50 |
71.4 |
|
|
They do not know about the diagnosis |
8 |
18.2 |
4 |
15.4 |
12 |
17.2 |
|
|
Frequency of psychology counseling |
Weekly or monthly |
13 |
46.4 |
12 |
57.1 |
25 |
51 |
|
Bimonthly, quarterly, other |
15 |
53.6 |
9 |
42.9 |
24 |
49 |
|
|
Self-report on how treatment is followed |
Excellent or good |
28 |
75.7 |
18 |
72 |
46 |
74.2 |
|
Fair, bad or terrible |
9 |
24.3 |
7 |
28 |
16 |
25.8 |
|
|
Current consumption of psychoactive substances (cigarette, coca paste and/or marihuana) |
Yes |
17 |
38.6 |
4 |
15.4 |
21 |
30 |
|
No |
27 |
61.4 |
22 |
84.6 |
49 |
70 |
|
|
Adherence to treatment |
No |
26 |
65 |
14 |
35 |
40 |
57.1 |
|
Yes |
18 |
60 |
12 |
40 |
30 |
42.9 |
|
|
Depression |
Absent/Mild |
29 |
65.9 |
20 |
76.9 |
49 |
70 |
|
Moderate/Severe |
15 |
34.1 |
6 |
23.1 |
21 |
30 |
|
|
Anxiety |
Minimal/Mild |
30 |
68.2 |
20 |
76.9 |
50 |
71.4 |
|
Moderate/Severe |
14 |
31.8 |
6 |
23.1 |
20 |
28.6 |
|
|
Perceived social support |
Low |
37 |
84.1 |
17 |
65.4 |
54 |
77.1 |
|
High |
7 |
15.9 |
9 |
34.6 |
16 |
22.9 |
|
Source: Own elaboration based on the data obtained in the study.
With this in mind, a public health problem is surfacing and demanding more attention, especially when it comes to low adherence to ART due to an increased probability of risk behaviors and possible reinfection and resistance to treatment, both in patients who have already been treated as in those who are just initiating a therapeutic regimen but have contracted a resistant virus (17,20). In addition, it causes a decrease in lymphocyte count and an increase in viral load, which facilitates the appearance of opportunistic diseases (21).
The findings in PLWHA from Quindío are not far removed from research in the field of adherence to treatment in Colombia, where Arrivillaga et al. (26) have indicated approximate figures (43%). In other countries, around 50% of patients with chronic diseases adhere, although this number can be between 37% and 83% in patients with HIV depending on the type of medication and population (42). Some studies show that about 50% of PLWHA fail to comply with medication intake and schedules, while 14% continue to maintain the risky behaviors that led them to become infected (17,43,44). It should be noted that adherence decreases as the complexity of the treatment increases, and that ART demands high compliance from the individual (more than 90-95%) to avoid resistance (21,45).
42.9% of patients in this study report being adherent. When comparing these results with other works, approximate figures can be found: in Spain reported adherence is 55% (45), in Venezuela 63.2% (46), and in Mexico between 31.9% (31), 57% (22), 65.6% (23) and 85.3%. This last indicator was not common when compared to most findings reporting a figure of about 50%, which may be explained by factors such as motivation and stress (19), particularly in Los Angeles, where the value reaches 63% (47).
However, differences with other studies were found: a study carried out in Madrid did not achieve strict therapeutic compliance not even in the third of the patients evaluated (20). In contrast, a longitudinal study in Italy reported a total of 81.4% of adherent patients (48). Comparative studies could help to reveal the contextual factors related to these differences.
Moreover, this research shows statistically significant differences that indicate greater adherence in those whose self-report is excellent when asked about the way they are following their treatment. However, despite the fact that 74.2% of PLWHA say that they have a good or excellent compliance with the treatment, only 42.9% adhered adequately according to the measurement instrument. The relevance of this aspect lies in the role of cognitive variables such as self-efficacy, locus of control, health beliefs, perception of vulnerability and treatment effectiveness in adherence behaviors (9-11), which require further research.
Similarly, there is a significant association between treatment adherence and depression. When depressive symptoms are absent or mild, the proportion of adherent and non-adherent patients does not differ. However, when these symptoms are moderate or severe, there is a significant difference, which indicates a greater probability of adherence among those with lower symptomatology. These findings coincide with reports in other countries such as Spain (20), Mexico (23) and Chile (49).
This situation is likely to be caused by the fact that HIV diagnosis and treatment generate distress (50), emotional alterations related to mourning due to the loss of health, and the assumption of a new role as a PLWHA, which can be more evident than in other diseases (e.g. cancer) (51). Likewise, patients may face discrimination and affective or economic losses given the social stigma that comes along with the disease, which in turn could generate alterations in their mood (12); furthermore, depressive symptoms may be a side effect of some transcriptase inhibitors (52,53).
Table 2. Association between sociodemographic, family, health and psychological variables, and adherence to treatment in people living with HIV/AIDS. Quindío, Colombia. 2015.
|
Characteristics |
Adherence to treatment |
p value |
OR |
95%CI |
|||||
|
Yes |
No |
||||||||
|
Lower |
Upper |
||||||||
|
n |
% |
n |
% |
||||||
|
Sex |
Men |
18 |
40.9 |
26 |
59.1 |
- |
1.000 |
- |
- |
|
Women |
12 |
46.2 |
14 |
53.8 |
0.669 |
1.238 |
0.466 |
3.291 |
|
|
Socioeconomic strata |
0, 1 and 2 |
23 |
45.1 |
28 |
54.9 |
- |
1.000 |
- |
- |
|
3, 4 and 5 |
6 |
54.5 |
5 |
45.5 |
0.570 |
1.461 |
0.395 |
5.407 |
|
|
Religion |
Believer (Catholicism, Protestantism) |
22 |
37.9 |
36 |
62.1 |
- |
1.000 |
- |
- |
|
Non-believer/Other |
8 |
66.7 |
4 |
33.3 |
0.077 |
3.273 |
0.881 |
12.156 |
|
|
Education |
Fifth grade |
10 |
40 |
15 |
60 |
- |
1.000 |
- |
- |
|
Complete High school |
11 |
37.9 |
18 |
62.1 |
0.876 |
0.917 |
0.306 |
2.745 |
|
|
Professional or technical studies |
8 |
66.7 |
4 |
33.3 |
0.136 |
3.000 |
0.709 |
12.694 |
|
|
Civil status |
Married, domestic partnership, in a relationship |
13 |
52 |
12 |
48 |
0.430 |
1.733 |
0.443 |
6.789 |
|
Single |
11 |
35.5 |
20 |
64.5 |
0.851 |
0.880 |
0.231 |
3.353 |
|
|
Separated/Widowed |
5 |
38.5 |
8 |
61.5 |
- |
1.000 |
- |
- |
|
|
HIV diagnosis |
≤2 years |
10 |
38.5 |
16 |
61.5 |
- |
1.000 |
- |
- |
|
3-5 years |
5 |
45.5 |
6 |
54.5 |
0.692 |
1.333 |
0.320 |
5.548 |
|
|
6-10 years |
6 |
40 |
9 |
60 |
0.923 |
1.067 |
0.291 |
3.916 |
|
|
10-22 years |
8 |
50 |
8 |
50 |
0.464 |
1.600 |
0.454 |
5.634 |
|
|
Support and understanding from relatives regarding treatment |
Never/sometimes |
3 |
37.5 |
5 |
62.5 |
0.848 |
1.200 |
0.185 |
7.770 |
|
Many times/always |
23 |
46 |
27 |
54 |
0.430 |
1.704 |
0.454 |
6.396 |
|
|
They do not know about the diagnosis |
4 |
33.3 |
8 |
66.7 |
- |
1.000 |
- |
- |
|
|
Frequency of psychology counseling |
Weekly or monthly |
11 |
44 |
14 |
56 |
- |
1.000 |
- |
- |
|
Bimonthly, quarterly, other |
13 |
54.2 |
11 |
45.8 |
0.477 |
1.504 |
0.488 |
4.639 |
|
|
Self-report of how treatment is followed |
Excellent or good |
20 |
43.5 |
26 |
56.5 |
0.038 * |
5.385 |
1.096 |
26.462 |
|
Fair, bad or terrible |
2 |
12.5 |
14 |
87.5 |
- |
1.000 |
- |
- |
|
|
Current consumption of psychoactive substances (cigarette, coca paste and/or marihuana) |
Yes |
8 |
38.1 |
13 |
61.9 |
- |
1.000 |
- |
- |
|
No |
22 |
44.9 |
27 |
55.1 |
0.599 |
1.324 |
0.466 |
3.766 |
|
|
Depression |
Absent/Mild |
25 |
51 |
24 |
49 |
0.040 * |
3.333 |
1.056 |
10.525 |
|
Moderate/Severe |
5 |
23.8 |
16 |
76.2 |
- |
1.000 |
- |
- |
|
|
Anxiety |
Minimal/Mild |
23 |
46 |
27 |
54 |
0.403 |
1.582 |
0.540 |
4.631 |
|
Moderate/Severe |
7 |
35 |
13 |
65 |
- |
- |
- |
||
|
Perceived social support |
Low |
20 |
37 |
34 |
63 |
- |
1.000 |
- |
- |
|
High |
10 |
62.5 |
6 |
37.5 |
0.077 |
2.833 |
0.894 |
8.975 |
|
* Statistically significant differences (p<0.05).
Source: Own elaboration based on the data obtained in the study.
The role of depression is fundamental to treatment, since negative thinking compromises the behavioral activity of those who present it at moderate and severe levels. Also, evidence shows that emotional states influence the functioning of the immune system and the evolution of HIV infection, particularly distress, depression and anxiety (18,44,54-56). The latter is identified in a higher proportion among non-adherents at moderate or severe levels, although no statistically significant differences have been observed.
Additionally, a higher proportion of adherence was found among those who scored higher in social support, even though no statistically significant differences were observed. This aspect has been studied extensively and is considered a factor that favors ART due to its buffering effect against stressful situations and depressive symptoms and, in general, its contribution to the process of adaptation to the new lifestyle.
There are many studies around the world that show social support as a protective factor related to adherence, well-being, perceived health and quality of life of PLWHA (18,29,31,57-59). This positive effect has also been confirmed in Colombia (7), where the search for professional support (6) and participation in support groups are also included (27). Similarly, the relationship between poor adherence to treatment, higher rates of emotional disturbances (distress and depression) and poor social support are clear (8,20,21,44); in spite of this, the fact that it can also become a source of conflict and stress must not be ignored (18).
In this particular sample, it is striking that when applying the MOS inventory, most participants perceived they were not socially supported, which is important for intervention in this context; however, when asked if they feel supported and understood by their relatives in relation to the treatment, most reported feeling it many times or always. This difference might suggest that, at first sight, although patients refer feeling supported, the way they receive such support is not perceived from an instrumental, affective, emotional or informational perspective in their daily lives, as the test indicates.
Further studies are required on what it means to provide and receive support, and to take a closer look at the different subtypes and their relationship to adherence. Likewise, it is important to delve into the role of social stigmatization, which can act to the detriment of seeking support, communicating the diagnosis, and deploying skills to obtain emotional and material support available in the surrounding environment.
Other results of this study indicate greater proportions of adherence in women (although not statistically significant), which requires more comparative research, and also among those who have higher levels of schooling and socioeconomic stratum, which is similar to the findings in other studies (26,60). Moreover, high adherence was also found in those who have a longer time of diagnosis, which positively interacts with the psychological variables that affect adherence (22), although its effects are inconclusive. In this regard, Levine et al. (47) observed that adherence seems to decline over time and Remor (20) identified greater adherence in patients with shorter infection times, since an increase in the probability of poor adherence when treatments involve several drugs for an indefinite period of time was observed. Finally, adherence was better in those who did not consume psychoactive substances, which is consistent with the literature presenting consumption as a problem in PLWHA (44,47). As for religion, studies are needed to elucidate its role as a coping strategy.
However, psychological and personal factors are not the only aspects implicated in adherence, since their effect may be influenced or mediated by aspects concerning the disease (symptoms and characteristics), treatment (secondary symptoms, therapeutic efficacy, doses, schedules, method of administration), the health system (characteristics of the system, barriers to medical care and accessibility to social and pharmaceutical services), the interaction of the patient with the health care team (relationship, communication, satisfaction, active involvement of staff and confidentiality) or social circumstances (educational level, social position, geographical and economic conditions, stigma and discrimination) (9,13,15,60-62). These aspects exceeded the objectives of this study, but the need for more research in this respect is emphasized to strengthen explanatory models.
In this sense, it is worth noting that research and work on adherence from a biopsychosocial perspective that considers all kinds of barriers and facilitators have a key role, so that people can exercise their duties and rights in health and follow their treatments adequately, particularly in developing countries (63). In Colombia, Arrivillaga et al. (26), Arrivillaga et al. (27), Arrivillaga et al. (28), and Arrivillaga et al. (62) report that the role of the health system, the socioeconomic position, gender role and other social aspects are some of the main obstacles to adherence to ART.
Finally, it is necessary to be cautious when interpreting the findings of this study due to the type and size of the sample and to the absence of validation measures in the Colombian population.
Conclusions
A high percentage of PLWHA did not report adequate adherence to ART (57.1%). A statistically significant association was found between adherence and depressive symptoms and self-assessment on the way treatment was followed. Low anxiety and high perception of social support did not represent statistically significant differences, but indicated higher proportions between adherents. The findings are related to global trends and some Colombian studies. There are no conclusive results on the association between diagnostic time, sociodemographic variables and adherence
to treatment.
Research on this topic has not discriminated some physiological symptoms that are typical of the infection, and those provoked by mood disorders; in addition, knowing the mental health history of the patients influences manifestation and coping methods, and would require further research on mediating variables and moderators of the relationship between depression and adherence.
In conclusion, longitudinal and mixed studies are recommended, as well as model proposals that include the analysis of the role of social and health barriers in adherence. The validation of interdisciplinary intervention programs contextualized to each region is pertinent in order to give effective answers to this situation that compromises public health.
Conflict of interests
None stated by the authors.
Funding
This research was funded by Universidad de San Buenaventura in Medellín and Hospital Departamental Universitario del Quindío San Juan de Dios.
Acknowledgement
To the participants of the study for their willingness to share their life experiences and to Dannys Alberth Aguirre for his contributions from the Asociación Ágora Colombia.
References
1.Hoja informativa 2015. Estadísticas Globales. Ginebra: ONUSIDA; 2015. Available from: https://goo.gl/dx0OX0.http://www.unaids.org/sites/default/files/media_asset/20150901_FactSheet_2015_es.pdf
2.Hoja Informativa 2016. Estadísticas mundiales. Ginebra: ONUSIDA; 2016. Available from: https://goo.gl/GyJdtU.
3.El sida en cifras 2015. Ginebra: ONUSIDA; 2015. Available from: https://goo.gl/h41cne.
4.Ministerio de Salud y Protección Social. Boletín Epidemiológico, situación del VIH/Sida Colombia 2013. Bogotá D.C.: MinSalud; 2013. Available from: https://goo.gl/1LrCMy.
5.Ministerio de Salud y Protección Social. Seguimiento de la Declaración de compromiso sobre el VIH/sida: Informe Nacional República de Colombia. Bogotá D.C.: Informe GARPR 2014; 2014. Available from: https://goo.gl/U8hKgr.
6.Gaviria AM, Quiceno JM, Vinaccia S, Martínez LA, Otalvaro MC. Estrategias de Afrontamiento y Ansiedad-Depresión en Pacientes Diagnosticados con VIH/Sida. Ter Psicológica. 2009;27(1):5-13. http://doi.org/fbb6gs.
7.Vinaccia-Alpi S, Fernández H, Quiceno JM, López-Posada M, Otalvaro C. Calidad de vida relacionada con la salud y apoyo social funcional en pacientes diagnosticados con VIH/Sida. Ter psicológica. 2008;26(1):125-32. http://doi.org/b9jhg5.
8.Carrobles JA, Remor E, Rodríguez-Alzamora L. Afrontamiento, apoyo social percibido y distrés emocional en pacientes con infección por VIH. Psicothema. 2003 [cited 2017 Mar 28];15(3):420-6. Available from: https://goo.gl/12IbQw.
9.Ginarte-Arias Y. La adherencia terapéutica. Rev Cuba Med Gen Integr. 2001;17(5):502-5.
10.Ortiz M, Ortiz E. Psicología de la salud: Una clave para comprender el fenómeno de la adherencia terapéutica. Rev Med Chile. 2007;135:647-52. http://doi.org/bpntkm.
11.Piña-López JA. Adhesión al tratamiento en personas con VIH/sida: una propuesta integradora (Adhesión y VIH/sida). Conductual. 2013[cited 2017 Mar 28];1(3):47-62. Available from: https://goo.gl/Q8VCvJ.
12.Martín-Alfonso L, Grau-Abalo J. La investigación de la adherencia terapéutica como un problema de la psicología de la salud. Psicología y Salud. 2004;14(1):89-99.
13.Knobel H, Guelar A. Estrategias para optimizar la adherencia al tratamiento antirretroviral: Intervenciones en la pauta terapéutica. Enferm Infecc Microbiol Clin. 2004;22(2):106-12. Available from:
http://doi.org/f2kgm5.
14.Piña-López JA, Sánchez-Sosa JJ. Modelo psicológico para la investigación de los comportamientos de adhesion en personas con VIH. Univ Psychol. 2007;6(2):399-407.
15.Alonso MA, Álvarez J, Arroyo J, Ávila L, Aylón R, Gangoso A, et al. Adherencia terapéutica: Estrategias prácticas de mejora. SaludMadrid. 2006;13(8):31-8.
16.Bejarano-Roncancio JJ, Ramírez ME, Saurith-lópez V, Sussman-Peña OA. Conocimientos, actitudes y prácticas alimentarias en pacientes diagnosticados con VIH en tratamiento farmacológico. Rev. Fac. Med. 2011;59(Supl 1):S3-11.
17.Ballester R. Adhesión terapéutica: Revisión histórica y estado de la cuestión en la infección por VIH/SIDA. Revista de Psicopatología y Psicología Clínica. 2002;7(3):151-75.
18.Villa IC, Vinaccia S. Adhesión terapéutica y variables psicológicas asociadas en pacientes con diagnóstico de VIH-sida. Psicología y Salud. 2006;16(1):51-62.
19.Sánchez-Sosa JJ, Cázares-Robles Ó, Piña-López JA, Dávila-Tapia M. Un modelo psicológico en los comportamientos de adhesión terapéutica en personas con VIH. Salud Ment. 2009;32(5):389-97.
20.Remor E. Valoración de la adhesión al tratamiento antirretroviral en pacientes VIH+. Psicothema. 2002;14(2):262-7.
21.Piña-López JA, Rivera-Icedo BM, Corrales-Rascón AE, Mungaray-Padilla K, Valencia-Vidrio MA. ¿Influye el tiempo de infección en meses sobre los predictores psicológicos de comportamientos de adhesión en una muestra de pacientes VIH+? Ter Psicológica. 2006 [cited 2017 Mar 28];24(2):183-90. Available from: https://goo.gl/as99Rw.
22.Piña-López JA, Sánchez-Sosa JJ, Fierros LE, Ybarra JL, Cázares-Robles Ó. Variables psicológicas y adhesión en personas con VIH: Evaluación en función del tiempo de infección. Ter Psicológica. 2011;29(2):149-57. http://doi.org/fzcqmh.
23.Piña-López JA, Dávila-Tapia M, Sánchez-Sosa JJ, Togawa C, Cázares-Robles Ó. Asociación entre los niveles de estrés y depresión y la adhesión al tratamiento en personas seropositivas al VIH en Hermosillo, México. Rev Panam Salud Pública. 2008;23(6):377-83. http://doi.org/d4td84.
24.González-Ramírez MT, Ybarra-Sagarduy JL, Piña-López JA. Relaciones sociales, variables psicológicas y conductas de adherencia en adultos con VIH. Int J Psychol Psychol Ther. 2012;12(2):173-84.
25.Arrivillaga M, Correa D, Varela M, Holguín L, Tovar J. Variables psicológicas en mujeres diagnosticadas con VIH/SIDA: Un estudio correlacional. Univ ersitas Psychol. 2006 [cited 2017 Mar 28];5(3):659-67. Available from: https://goo.gl/I6dLPk.
26.Arrivillaga M, Ross M, Useche B, Alzate ML, Correa D. Social position, gender role, and treatment adherence among Colombian women living with HIV/AIDS: social determinants of health approach. Rev Panam Salud Pública. 2009;26(6):502-10. http://doi.org/fhfhfn.
27.Arrivillaga M, Ross M, Useche B, Springer A, Correa D. Applying an expanded social determinant approach to the concept of adherence to treatment: the case of Colombian women living with HIV/AIDS. Womens Health Isues. 2011;21(2):177-83. http://doi.org/c7cbhk.
28.Arrivillaga M, Springer AE, Lopera M, Correa D, Useche B, Ross MW. HIV/AIDS treatment adherence in economically better off women in Colombia. AIDS Care. 2012;24(7):929-35. http://doi.org/fxrpx9.
29.Remor E. Apoyo social y calidad de vida en la infección por el VIH. Atención Primaria. 2002;30(3):143-8. http://doi.org/f2km2t.
30.Estrada Aguilera A, Vera Pérez V. Influencia social y familiar en el comportamiento del paciente con VIH/SIDA ante su diagnóstico y manejo. Rev Hosp Jua Mex. 2004;71(1):29-35.
31.González-Ramírez MT, Piña-López JA. Motivos, apoyo social y comportamientos de adhesión en personas con VIH: modelamiento con ecuaciones estructurales. Univ Psychol. 2011;10(2):399-409.
32.Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67-74. http://doi.org/dvj9mc.
33.Nogués-Solán X, Sorli Redó ML, Villar García J. Instrumentos de medida de adherencia al tratamiento. An Med Interna. 2007;24(3):138-41. http://doi.org/dstvr2.
34.Rodríguez-Chamorro MÁ, García-Jiménez E, Amariles P, Rodríguez-Chamorro A, Faus MJ. Revisión de tests de medición del cumplimiento terapéutico utilizados en la práctica clínica. Atención Primaria. 2008;40(8):413-7. http://doi.org/fwhdcm.
35.Serrano-Castro PJ, Pozo-Muñoz C, Alonso-Morillejo E, Martos-Méndez MJ, Bretones-Nieto B. Factores vinculados a la adhesión al tratamiento en pacientes con epilepsia refractaria y no refractaria. Rev Neurol. 2011;53(12):721-8.
36.Castaño-Castrillón J, Echeverri-Rubio C, Giraldo-Cardona JF, Maldonado-Mora Á, Melo-Parra J, Meza-Orozco G, et al. Adherencia al tratamiento de pacientes hipertensos atendidos en Assbasalud ESE, Manizales (Colombia) 2011. Rev Fac Med. 2012;60(3):179-97.
37.Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4(6):561-71. http://doi.org/cgh25q.
38.Beck AT, Steer RA, Carbin MG. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clin Psychol Rev. 1988;8(1):77-100. http://doi.org/cw3bsj.
39.Sanz J. Recomendaciones para la utilización de la adaptación española del Inventario de Ansiedad de Beck (BAI) en la práctica clínica. Clínica y Salud. 2014;25(1):39-48. http://doi.org/b4z3.
40.Londoño-Arredondo NH, Rogers HL, Castilla-Tang JF, Posada-Gómez SL, Ochoa-Arizal NL, Jaramillo-Pérez M, et al. Validación en Colombia del cuestionario MOS de apoyo social. Int J Psychol Res. 2012 [cited 2017 Mar 29];5(1):142-50. Available from: https://goo.gl/GihHIO.
41.Martín-Alfonso L. Repercusiones para la salud pública de la adherencia terapéutica deficiente. Rev Cuba Salud Pública. 2006;32(3):1-9.
42.Organización Panamericana de la Salud. Adherencia a los tratamientos a largo plazo: pruebas para la acción. Washington D.C.: Organización Mundial de la Salud; 2004 [cited 2017 Mar 30]. Available from: https://goo.gl/XCi3Kb.
43.Nieuwkerk PT, Sprangers MA, Burger DM, Hoetelmans RM, Hugen PW, Danner SA, et al. Limited patient adherence to Highly Active Antiretroviral Therapy for HIV-1 infection in an observational cohort study. Arch Intern Med. 2001;161(16):1962-8. http://doi.org/cb8rb4.
44.Ballester-Arnal R. Aportaciones desde la psicología al tratamiento de las personas con infección por VIH/SIDA. Revista de Psicopatología y Psicología Clínica. 2005;10(1):53-69. http://doi.org/b42k.
45.Ortego C, Huedo-Medina TB, Vejo J, Llorca FJ. Adherence to highly active antiretroviral therapy in Spain. A meta-analysis. Gac Sanit. 2011;25(4):282-9. http://doi.org/ddmgrs.
46.Leone S, Márquez L. Relación estigma y calidad de vida en la adhesión al tratamiento de pacientes con VIH/SIDA. Eureψa. 2014;11(2):258-69.
47.Levine AJ, Hinkin CH, Castellon SA, Mason KI, Lam MN, Perkins A, et al. Variations in patterns of highly active antiretroviral therapy (HAART) adherence. AIDS Behav. 2005;9(3):355-62. http://doi.org/b9hfd5.
48.Aloisi MS, Arici C, Balzano R, Noto P, Piscopo R, Filice G, et al. Behavioral correlates of adherence to antirretroviral therapy. J Acquir Immune Defic Sydromes. 2002;31(Suppl 3):S145-8.
49.Varela M, Galdames S. Depresión y adhesión a terapia anti-retroviral en pacientes con infección por VIH atendidos en el Hospital San Pablo de Coquimbo, Chile. Rev Chilena Infectología. 2014;31(3):323-8. http://doi.org/b42n.
50.Remor E, Ulla S, Arranz P, Carrobles JA. ¿Es la percepción de control un factor protector contra el distrés emocional en personas VIH+? Psiquis. 2001;22(3):111-6.
51.Edo M, Ballester R. Estado emocional y conducta de enfermedad en pacientes con VIH/SIDA y enfermos oncológicos. Revista de Psicopatología y Psicología Clínica. 2006 [cited 2017 Mar 30];11(2):79-90. Available from: https://goo.gl/LnRpsk.
52.Soto-Ramírez LE, Herrera-Bastos E, Andrade-Vilanueva J, Calva-Mercado JJ, Gaytan-Martínez J, et al. Guía de manejo antirretroviral de las personas con VIH: Recomendaciones para el tratamiento antirretroviral en adultos. México D.F. Organización Mundial para la Salud; 2011 [cited 2017 Mar 30]. Available from: https://goo.gl/utGheC.
53.Consejo Nacional para la Prevención y Control del Sida. Guía de manejo antirretroviral de las personas con VIH. México D.F.: Conasida; 2014 [cited 2017 Mar 30]. Available from: https://goo.gl/Z5K7Ik.
54.Borrás F. SIDA: Aportaciones desde la psiconeuroinmunología. Rev de Psicol Gral y Aplic. 1994;47(2):225-9.
55.De Flores T. Impacto emocional y cambios inmunológicos en la notificación diagnóstica de seropositividad. Ann Psicol. 1994;10(2):135-43.
56.Klinger JC, Herrera JA, Díaz ML, Jhann AA, Ávila GI, Tobar CI. La psiconeuroinmunología en el proceso salud enfermedad. Colomb Med. 2005 [cited 2017 Mar 30];36(2):120-9. Available from: https://goo.gl/TMZvmJ.
57.Watt MH, Maman S, Earp JA, Eng E, Setel PW, Golin CE, et al. “It’s all the time in my mind”: Facilitators of adherence to antiretroviral therapy in a Tanzanian setting. Soc Sci Med; 2009;68(10):1793-800. http://doi.org/bmrm68.
58.Wu X, Chen J, Huang H, Liu Z, Li X, Wang H. Perceived stigma, medical social support and quality of life among people living with HIV/AIDS in Hunan, China. Appl Nurs Res. 2015;28(2):169-74. http://doi.org/f697t4.
59.Kelly JD, Hartman C, Graham J, Kallen MA, Giordano TP. Social support as a predictor of early diagnosis, linkage, retention, and adherence to HIV care: Results from the steps study. J Assoc Nurses AIDS Care. 2014;25(5):405-13. http://doi.org/f6pbxm.
60.Heath K, Singer J, O´Shaughnessy M, Montaner JS, Hogg RS. Intentional Nonadherence due to adverse symptoms associated with antiretroviral therapy. J Acquir Defic Syndr. 2002;31(2):211-7. http://doi.org/btw5dz.
61.Margulies S, Barber N, Recoder ML. VIH-SIDA y “Adherencia” al tratamiento: Enfoques y perspectivas. Antípoda. 2006;3:281-300.
62.Arrivillaga-Quintero M. Análisis de las barreras para la adherencia terapéutica en mujeres colombianas con VIH/sida: cuestión de derechos de salud. Salud Publica Mex. 2010;52(4):350-6. http://doi.org/dh6ck7.
63.Posse M, Meheus F, van Asten H, van der Ven A, Baltussen R. Barriers to access to antiretroviral treatment in developing countries: a review. Trop Med Int Heal. 2008;13(7):904-13. http://doi.org/bm652t.
Recibido: 2 de febrero de 2016; Aceptado: 16 de junio de 2016
Abstract
Introduction:
HIV/AIDS is a chronic disease; therefore, recognizing which factors favor adherence to antiretroviral treatment is necessary.
Objective:
To determine the association between adherence to antiretroviral treatment and depression, anxiety, perception of social support and sociodemographic variables in people living with HIV/ AIDS in Quindío, Colombia.
Materials and methods:
An observational, cross-sectional study was performed in an intentional sample of 70 adults, who were applied the Morisky-Green questionnaire, the Beck Depression Inventory, the Beck Anxiety Inventory, the Medical Outcomes Study (MOS) Social Support Survey, and a sociodemographic survey. Univariate and bivariate analyzes were performed by calculating the odds ratio to determine association (p<0.05).
Results:
57.1% ofthe participants reported low adherence to treatment, 30% had moderate or severe depressive symptoms, 71.4% scored minimal or mild anxiety levels, and 77.1% had a low perception of social support. A statistical association between depression (high levels tripled the risk of non-adherence) and self-report on how treatment is followed (excellent or good self-report increased by five times the probability of adherence) was found.
Conclusion:
Depression and self-report on compliance were associated with adherence to antiretroviral therapy. A comprehensive study on the perception of social support and cognitive variables, such as self-efficacy and risk perception, is highly recommended for people living with HIV/AIDS.
Keywords:
HIV, Antiretroviral Therapy Highly Active, Medication Adherence, Depression, Anxiety, Social Support (MeSH).Resumen
Introducción.
El VIH/sida es una enfermedad crónica, por ello es necesario reconocer qué factores favorecen la adhesión al tratamiento antirretroviral.
Objetivo.
Determinar la asociación entre adhesión al tratamiento antirretroviral y depresión, ansiedad, percepción de apoyo social y variables sociodemográficas en personas viviendo con VIH/sida en Quindío, Colombia.
Materiales y métodos.
Se realizó un estudio observacional analítico de tipo transversal en una muestra intencional de 70 adultos, a quienes se les aplicó el cuestionario autorreferido de Morisky-Green, el Inventario de Depresión de Beck, el Inventario de Ansiedad de Beck, el cuestionario MOS (Medical Outcomes Study) de Apoyo Social y una encuesta sociodemográfica. Se realizaron análisis univariados y bivariados calculando Odds Ratio para determinar asociación (p<0.05).
Resultados.
57.1% de los participantes reportó poca adhesión al tratamiento, 30% presentó síntomas depresivos moderados o graves, 71.4% puntuó niveles mínimos o leves de ansiedad y 77.1% tuvo baja percepción de apoyo social. Se encontró asociación estadística entre depresión -niveles altos triplicaron el riesgo de no adhesión- y autoevaluación de la manera como se sigue el tratamiento -excelente o buena aumentó cinco veces la probabilidad de adhesión-.
Conclusión.
La depresión y la autoevaluación del cumplimiento se asociaron con adhesión al tratamiento antirretroviral. Se sugiere profundizar el estudio de la percepción de apoyo social y variables cognitivas, como la autoeficacia y percepción de riesgo, en personas que viven con VIH/sida.
Palabras clave:
VIH, Terapia antirretroviral altamente activa, Adhesión al tratamiento, Depresión, Ansiedad, Apoyo social (DeCS).Introduction
HIV is a public health concern worldwide. Since 2000, 38.1 million people have acquired the virus and 25.3 million have died from AIDS-related illnesses 1. In 2015, UNAIDS 2 reported an average of 34 to 39.8 million people living with HIV/AIDS (PLWHA) in the world; in Latin America, the figure ranges between 1.7 and 2.3 million. According to the same report, 17 million people had access to antiretroviral therapy (ART) in December 2015, while about 22 million people did not have access to treatment at all. About 28 million new cases could be avoided, ifresponse to AIDS in low- and middle-income countries increases 3.
The Colombian Public Health Surveillance System reported 8 196 new PLWHA cases in 2012 4, with the highest incidence in Barranquilla (50.6 cases per 100 000 inhabitants), Quindío (28.4 cases per 100 000 inhabitants), and Cartagena (37.6 cases per 100 000 inhabitants). In addition, 2 216 deaths associated with HIV/AIDS and a mortality rate of 4.76 per 100 000 inhabitants were reported. Quindío was one of the most affected departments by this epidemic 5.
HIV/AIDS is considered a chronic disease that involves multiple factors, since it has an impact on physical and mental functioning 6 and may affect self-concept and sense of life 7. This condition is a stressor that implicates psychological, physiological, social and economic aspects, therefore, it demands strategies that favor treatment and reduce threats to health. In this regard, the patient's attitudes and coping techniques can influence the HIV infection process 8, which, in turn, demands changes in lifestyle to comply with therapeutic indications. This is known as adherence to treatment, and indicates the commitment and participation of the individual in self-care 9,10.
Although no consensus in the definition of treatment adherence has been achieved (also known as cooperation or therapeutic compliance), it is generally understood as a complex and multifactorial problem that transcends following closely medical instructions or prescriptions 9,11. As proposed by DiMatteo & DiNicola, and accepted by other researchers, adherence is an active process of voluntary collaboration established between the patient and the health personnel to carry out mutually agreed upon behaviors, in order to generate the desired therapeutic effect 10,12,13.
Piña-López & Sánchez-Sosa 14 suggest that adherence in PLWHA is determined by the frequency with which subjects develop behaviors to comply with the instructions provided by health personnel based on their own skills. Adherence behaviors are a consequence of the interaction between biological variables (HIV disease and other conditions) and psychological variables (interaction styles related to stress, abilities, motives and emotional states), which have effects on health, control and course of infection with HIV 11,14.
Different situations may affect adherence to treatment in chronic diseases, for example, the nature of the disease, the time of evolution, the expectation of treatment outcomes, the characteristics of the treatment, the habits and customs of the patient 15,16, the interaction with health professionals, the characteristics of the health institution 9, and psychological and social aspects such as coping strategies 6. Other important factors in HIV infection include its asymptomatic character in most cases, the amount of drugs supplied (antiretrovirals and those necessary for opportunistic diseases), social stigmatization, side effects of certain drugs, patient's beliefs, affective states, perception of control over stressful life events, and the disease, among others 17,18.
Following the model of Sánchez-Sosa et al. 19, psychological variables such as depression, stress, anxiety, low motivation and lack of social support can contribute to the progression of the disease and reduce the quality of life of the affected patients.
Remor 20 reports low adherence in the presence of high levels of anxiety, stress, depression and poor social support. Piña-López et al. 21 and Piña-López et al. 22 report competencies, stress, motives, frustration, tolerance and ambiguity as predictors of adherence, which may vary according to the time of infection; also, Piña-López et al. 23 proposed that intermediate levels of stress and low levels of depression are favorable, and, finally, Piña-López et al. 24 add that associated psychological variables are affected by self-report on social competences.
Arrivillaga et al. have identified a correlation between anxiety and depression, as well as a perception of poor control over health and stressful life events in women living with HIV/AIDS, which affect their adherence and quality of life. Likewise, Arrivillaga et al. 26, Arrivillaga et al. 27 y Arrivillaga et al. 28 stress the role played by social and economic factors in the adherence to antiretroviral treatment (ART) by women. Social support is another key factor associated with better health results, adherence and quality of life in PLWHA 7,25,29-31.
In this regard, adherence to ART is a complex process, permeated by psychological and social factors of great relevance for the evolution, treatment and quality of life of PLWHA. These factors need to be further analyzed given the implications for public health that the lack of adherence to ART have, and to contribute to the enrichment of intervention programs. It is, therefore, pertinent to generate knowledge in this field, and specifically in one of the leading departments of morbidity and mortality caused by HIV/AIDS in Colombia. The aim of this study was to establish the association between adherence to antiretroviral therapy and depression, anxiety, perception of social support and sociodemographic variables in a group of PLWHA in Quindío, Colombia during 2015.
Methodology
This is an observational and analytical cross-sectional study, in which 70 PLWHA participated -men and women enrolled in an accompaniment program offered by a health institution in Quindío (Colombia). Some of them were hospitalized and others were attending medical and psychological follow-ups. Sampling was non-probabilistic, intentional, and selected taking into account as inclusion criteria HIV diagnosis, ART, being of legal age, no physical or mental conditions that would hinder understanding the instruments, will to participate in the study, and a signed informed consent.
A socio-demographic data survey was used for collecting information regarding age, sex, marital status, schooling, socioeconomic stratum and religion. In addition, variables related to the disease such as diagnosis time, perception of family support and understanding during the treatment, consumption of psychoactive substances (cigarettes, coca paste and/or marihuana), frequency of psychological therapy, and self-report on how treatment was followed were also investigated.
Adherence to ART was assessed using the Morisky-Green Scale 32, which reflects patient compliance with medication and has been used in different studies 33-36. This instrument consists of four questions with two response options (Yes/No); if the answer for any of these items is Yes, it means that the patient has failed and is reported as non-adherent.
To identify depressive symptoms and their severity, the Beck Depression Inventory (BDI) was applied; this is a 21-item scale that considers psychological-cognitive and somatic-vegetative aspects, which are evaluated based on affirmations selected by the individual. The scores range from 0 to 3, yielding a total number between 0 and 63. A score of 0 to 9 indicates absence of depression; 10 to 18, mild depression; 19 to 29, moderate depression, and from 30 onwards, severe depression 37,38.
On the other hand, the Beck Anxiety Inventory (BAI) was used to evaluate anxiety symptoms when investigating subjective, neurophysiological, autonomic and panic factors. This inventory is made up of 21 items, each with the following response options: 0-not at all; 1-slightly, it does not bother me much; 2-moderately, it was very unpleasant but I could bear it, and 3-severely, I could hardly bear it. In the Spanish version, the cut-off points are 0 to 7 for minimal anxiety, 8 to 15 for mild anxiety, 16 to 25 for moderate anxiety, and 26 to 63 for severe anxiety 39.
Perceived social support was assessed using the Medical Outcomes Study (MOS) questionnaire designed by Sherbourne and Stewart in 1991, and adapted to the Colombian population 40, which assesses structural support or size of the social network (item 1) and functional support (perception of support, items 2-19). Functional support is independent and multidimensional, and is composed of emotional/informative, tangible and affective social support and positive social interaction. The first question inquiries into the number of close friends and relatives. The remaining questions have answering options from 1 to 5 (never, rarely, sometimes, most of the time, always). The raw scores range from 19 to 95, and a higher score indicates greater perceived social support.
The study was supported by the Bioethics Committee of the Universidad de San Buenaventura Medellín. The instruments were codified and a route was established for channeling severe depression and anxiety cases or suicidal ideation in order to refer patients to specialists or appropriate care centers. Subsequently, the participants were contacted to be informed about the objectives and procedures of the study, and to request voluntary participation. An appointment was coordinated with those who accepted under certain conditions to ensure confidentiality.
The instruments were applied through an individual interview; prior informed consent was signed and participants were informed about the purpose of the study, voluntariness, confidentiality and non-remuneration, as well as about their right to abandon the study at any time. Individual results were returned to participants, and general results to the health institution. Lastly, the channeling route was activated in the necessary cases.
Data tabulation was performed in Microsoft Excel 2013, and the statistical analysis was made through SPSS version 21. Univariate and bivariate analyzes were performed. Central tendency, dispersion and position were evaluated as quantitative variables and, on the other hand, qualitative variables included absolute and relative frequencies. To determine the existence or non-existence of statistical association, the odds ratio (OR) was calculated and its confidence intervals and p values were deemed as significant when they were <0.05.
It should be noted that depression and anxiety variables were dichotomized for the analysis, and were reported as absent/mild depression, moderate/severe depression, and minimal/mild anxiety, moderate/severe anxiety. Regarding social support perception, the scores found in the first three quartiles were taken as low, and the ones in the last quartile were considered high. The socioeconomic stratum variable was analyzed based on the Colombian stratification, and was grouped into three categories: 0, 1 and 2, which included homeless population, low-low and low strata, and 3, 4 and 5 strata gathering middle-low, medium and medium-high strata.
Results
70 people, aged between 18 and 66 years, answered the survey; the average age was 38, with a standard deviation of12 years. The highest age in 50% of the participants was 38, and the most frequent was 28. The highest proportions were found among men (64.5%), patients of socioeconomic strata 0, 1 and 2 (82.3%), catholics or protestants (82.9%), high school graduates (43.9%), and single (44.9%). 38.2% of the subjects were diagnosed two years or less before they participated in the study. Most of them (71.4%) reported feeling supported and understood by their relatives, and affirmed that they were receiving psychological therapy on a regular basis. 30% of the patients reported that they are currently using psychoactive substances.
57.1% ofthe patients did not show adherence to the pharmacological treatment, although most of them state that they are following it with excellent outcomes (74.2%). Regarding the psychological variables, absent or mild levels of depression were found in most participants; 30% scored moderate or severe depression. Moderate or severe levels of anxiety were observed in 28.6% of the cases, and the perception of little social support in 77.1% (Table 1).
Source: Own elaboration based on the data obtained in the study.Table 1: Percentage distribution of sociodemographic, family, health and psychological variables evaluated in people living with HIV/AIDS by sex. Quindío, Colombia. 2015.
Bivariate analysis
In order to determine some associations that would indicate possible factors related to ART adherence, a bivariate analysis was performed. Two of the evaluated variables had a statistically significant association with adherence: self-report on the way in which treatment was followed (p=0.038, OR=5.385, 95%CI: 1.096-26.46) and depression (p=0.040, OR=3.33; 95%CI: 1.056-10.52). The p-value found in the remaining variables was >0.05, although a higher proportion of adherence was observed in women, in people from socioeconomic strata 3 to 5, in those who have more than 10 years of diagnosis, in those who do not profess any religion, are married or in some kind of relationship, have technical or professional studies, who frequently or always feel support and understanding from their families, those who attend therapy periodically, who are not currently using any type of illegal substance, and those who have low levels of anxiety and perceive high levels of social support (Table 2).
* Statistically significant differences (p<0.05). Source: Own elaboration based on the data obtained in the study.Table 2: Association between sociodemographic, family, health and psychological variables, and adherence to treatment in people living with HIV/AIDS. Quindío, Colombia. 2015.
Discussion
This study identified adherence to treatment in a group of PLWHA in Quindío and its association with psychological and social variables that may play a fundamental role in interventions with this population. An outstanding percentage of subjects showed poor adherence (57.1%), which is highly relevant since this situation may indicate how patients are coping with their condition and, at the same time, how their quality of life and their relatives or closed ones are being affected by it.
Lack of adherence to long-term treatment leads to personal, social, health and economic issues, as it generates a greater risk to health (relapses, onset or worsening of symptoms, evolution to late or severe phases of the disease, adverse effects, and resistance to medication), lower quality of life and well-being; higher rates of stress, interference with lifestyle or alterations in performance areas of patients and their relatives, and greater probability of increasing the demand for hospital and pharmaceutical resources 41.
With this in mind, a public health problem is surfacing and demanding more attention, especially when it comes to low adherence to ART due to an increased probability of risk behaviors and possible reinfection and resistance to treatment, both in patients who have already been treated as in those who are just initiating a therapeutic regimen but have contracted a resistant virus 17,20. In addition, it causes a decrease in lymphocyte count and an increase in viral load, which facilitates the appearance of opportunistic diseases 21.
The findings in PLWHA from Quindío are not far removed from research in the field of adherence to treatment in Colombia, where Arrivillaga et al. 26 have indicated approximate figures (43%). In other countries, around 50% of patients with chronic diseases adhere, although this number can be between 37% and 83% in patients with HIV depending on the type of medication and population 42. Some studies show that about 50% of PLWHA fail to comply with medication intake and schedules, while 14% continue to maintain the risky behaviors that led them to become infected 17,43,44. It should be noted that adherence decreases as the complexity of the treatment increases, and that ART demands high compliance from the individual (more than 90-95%) to avoid resistance 21,45.
42.9% of patients in this study report being adherent. When comparing these results with other works, approximate figures can be found: in Spain reported adherence is 55% 45, in Venezuela 63.2% 46), and in Mexico between 31.9% 31, 57% 22, 65.6% 23 and 85.3%. This last indicator was not common when compared to most findings reporting a figure of about 50%, which may be explained by factors such as motivation and stress 19, particularly in Los Angeles, where the value reaches 63% 47.
However, differences with other studies were found: a study carried out in Madrid did not achieve strict therapeutic compliance not even in the third of the patients evaluated 20. In contrast, a longitudinal study in Italy reported a total of 81.4% of adherent patients 48. Comparative studies could help to reveal the contextual factors related to these differences.
Moreover, this research shows statistically significant differences that indicate greater adherence in those whose self-report is excellent when asked about the way they are following their treatment. However, despite the fact that 74.2% of PLWHA say that they have a good or excellent compliance with the treatment, only 42.9% adhered adequately according to the measurement instrument. The relevance of this aspect lies in the role of cognitive variables such as self-efficacy, locus of control, health beliefs, perception of vulnerability and treatment effectiveness in adherence behaviors 9-11, which require further research.
Similarly, there is a significant association between treatment adherence and depression. When depressive symptoms are absent or mild, the proportion of adherent and non-adherent patients does not differ. However, when these symptoms are moderate or severe, there is a significant difference, which indicates a greater probability of adherence among those with lower symptomatology. These findings coincide with reports in other countries such as Spain 20, Mexico 23 and Chile 49.
This situation is likely to be caused by the fact that HIV diagnosis and treatment generate distress 50, emotional alterations related to mourning due to the loss of health, and the assumption of a new role as a PLWHA, which can be more evident than in other diseases (e.g. cancer) 51. Likewise, patients may face discrimination and affective or economic losses given the social stigma that comes along with the disease, which in turn could generate alterations in their mood 12; furthermore, depressive symptoms may be a side effect of some transcriptase inhibitors 52,53.
The role of depression is fundamental to treatment, since negative thinking compromises the behavioral activity of those who present it at moderate and severe levels. Also, evidence shows that emotional states influence the functioning of the immune system and the evolution of HIV infection, particularly distress, depression and anxiety 18,44,54-56. The latter is identified in a higher proportion among non-adherents at moderate or severe levels, although no statistically significant differences have been observed.
Additionally, a higher proportion of adherence was found among those who scored higher in social support, even though no statistically significant differences were observed. This aspect has been studied extensively and is considered a factor that favors ART due to its buffering effect against stressful situations and depressive symptoms and, in general, its contribution to the process of adaptation to the new lifestyle.
There are many studies around the world that show social support as a protective factor related to adherence, well-being, perceived health and quality of life of PLWHA 18,29,31,57-59. This positive effect has also been confirmed in Colombia 7, where the search for professional support 6 and participation in support groups are also included 27. Similarly, the relationship between poor adherence to treatment, higher rates of emotional disturbances (distress and depression) and poor social support are clear 8,20,21,44; in spite of this, the fact that it can also become a source of conflict and stress must not be ignored 18.
In this particular sample, it is striking that when applying the MOS inventory, most participants perceived they were not socially supported, which is important for intervention in this context; however, when asked if they feel supported and understood by their relatives in relation to the treatment, most reported feeling it many times or always. This difference might suggest that, at first sight, although patients refer feeling supported, the way they receive such support is not perceived from an instrumental, affective, emotional or informational perspective in their daily lives, as the test indicates.
Further studies are required on what it means to provide and receive support, and to take a closer look at the different subtypes and their relationship to adherence. Likewise, it is important to delve into the role of social stigmatization, which can act to the detriment of seeking support, communicating the diagnosis, and deploying skills to obtain emotional and material support available in the surrounding environment.
Other results of this study indicate greater proportions of adherence in women (although not statistically significant), which requires more comparative research, and also among those who have higher levels of schooling and socioeconomic stratum, which is similar to the findings in other studies 26,60. Moreover, high adherence was also found in those who have a longer time of diagnosis, which positively interacts with the psychological variables that affect adherence 22, although its effects are inconclusive. In this regard, Levine et al. 47 observed that adherence seems to decline over time and Remor 20 identified greater adherence in patients with shorter infection times, since an increase in the probability of poor adherence when treatments involve several drugs for an indefinite period of time was observed. Finally, adherence was better in those who did not consume psychoactive substances, which is consistent with the literature presenting consumption as a problem in PLWHA 44,47. As for religion, studies are needed to elucidate its role as a coping strategy.
However, psychological and personal factors are not the only aspects implicated in adherence, since their effect may be influenced or mediated by aspects concerning the disease (symptoms and characteristics), treatment (secondary symptoms, therapeutic efficacy, doses, schedules, method of administration), the health system (characteristics of the system, barriers to medical care and accessibility to social and pharmaceutical services), the interaction of the patient with the health care team (relationship, communication, satisfaction, active involvement of staff and confidentiality) or social circumstances (educational level, social position, geographical and economic conditions, stigma and discrimination) 9,13,15,6062. These aspects exceeded the objectives of this study, but the need for more research in this respect is emphasized to strengthen explanatory models.
In this sense, it is worth noting that research and work on adherence from a biopsychosocial perspective that considers all kinds of barriers and facilitators have a key role, so that people can exercise their duties and rights in health and follow their treatments adequately, particularly in developing countries 63. In Colombia, Arrivillaga et al. 26, Arrivillaga et al. 27, Arrivillaga et al. 28, and Arrivillaga et al. 62 report that the role of the health system, the socioeconomic position, gender role and other social aspects are some of the main obstacles to adherence to ART.
Finally, it is necessary to be cautious when interpreting the findings of this study due to the type and size of the sample and to the absence of validation measures in the Colombian population.
Conclusions
A high percentage of PLWHA did not report adequate adherence to ART (57.1%). A statistically significant association was found between adherence and depressive symptoms and self-assessment on the way treatment was followed. Low anxiety and high perception of social support did not represent statistically significant differences, but indicated higher proportions between adherents. The findings are related to global trends and some Colombian studies. There are no conclusive results on the association between diagnostic time, sociodemographic variables and adherence to treatment.
Research on this topic has not discriminated some physiological symptoms that are typical of the infection, and those provoked by mood disorders; in addition, knowing the mental health history of the patients influences manifestation and coping methods, and would require further research on mediating variables and moderators of the relationship between depression and adherence.
In conclusion, longitudinal and mixed studies are recommended, as well as model proposals that include the analysis of the role of social and health barriers in adherence. The validation of interdisciplinary intervention programs contextualized to each region is pertinent in order to give effective answers to this situation that compromises public health.
Acknowledgement
To the participants of the study for their willingness to share their life experiences and to Dannys Alberth Aguirre for his contributions from the Asociación Ágora Colombia.
References
Referencias
Hoja informativa 2015. Estadísticas Globales. Ginebra: ONUSIDA; 2015. Available from: https://goo.gl/dx0OX0.http://www.unaids.org/sites/default/files/media_asset/20150901_FactSheet_2015_es.pdf
Hoja Informativa 2016. Estadísticas mundiales. Ginebra: ONUSIDA; 2016. Available from: https://goo.gl/GyJdtU.
El sida en cifras 2015. Ginebra: ONUSIDA; 2015. Available from: https://goo.gl/h41cne.
Ministerio de Salud y Protección Social. Boletín Epidemiológico, situación del VIH/Sida Colombia 2013. Bogotá D.C.: MinSalud; 2013. Available from: https://goo.gl/1LrCMy.
Ministerio de Salud y Protección Social. Seguimiento de la Declaración de compromiso sobre el VIH/sida: Informe Nacional República de Colombia. Bogotá D.C.: Informe GARPR 2014; 2014. Available from: https://goo.gl/U8hKgr.
Gaviria AM, Quiceno JM, Vinaccia S, Martínez LA, Otalvaro MC. Estrategias de Afrontamiento y Ansiedad-Depresión en Pacientes Diagnosticados con VIH/Sida. Ter Psicológica. 2009;27(1):5-13. http://doi.org/fbb6gs.
Vinaccia-Alpi S, Fernández H, Quiceno JM, López-Posada M, Otalvaro C. Calidad de vida relacionada con la salud y apoyo social funcional en pacientes diagnosticados con VIH/Sida. Ter psicológica. 2008;26(1):125-32. http://doi.org/b9jhg5.
Carrobles JA, Remor E, Rodríguez-Alzamora L. Afrontamiento, apoyo social percibido y distrés emocional en pacientes con infección por VIH. Psicothema. 2003 [cited 2017 Mar 28];15(3):420-6. Available from: https://goo.gl/12IbQw.
Ginarte-Arias Y. La adherencia terapéutica. Rev Cuba Med Gen Integr. 2001;17(5):502-5.
Ortiz M, Ortiz E. Psicología de la salud: Una clave para comprender el fenómeno de la adherencia terapéutica. Rev Med Chile. 2007;135:647-52. http://doi.org/bpntkm.
Piña-López JA. Adhesión al tratamiento en personas con VIH/sida: una propuesta integradora (Adhesión y VIH/sida). Conductual. 2013[cited 2017 Mar 28];1(3):47-62. Available from: https://goo.gl/Q8VCvJ.
Martín-Alfonso L, Grau-Abalo J. La investigación de la adherencia terapéutica como un problema de la psicología de la salud. Psicología y Salud. 2004;14(1):89-99.
Knobel H, Guelar A. Estrategias para optimizar la adherencia al tratamiento antirretroviral: Intervenciones en la pauta terapéutica. Enferm Infecc Microbiol Clin. 2004;22(2):106-12. Available from:
Piña-López JA, Sánchez-Sosa JJ. Modelo psicológico para la investigación de los comportamientos de adhesion en personas con VIH. Univ Psychol. 2007;6(2):399-407.
Alonso MA, Álvarez J, Arroyo J, Ávila L, Aylón R, Gangoso A, et al. Adherencia terapéutica: Estrategias prácticas de mejora. SaludMadrid. 2006;13(8):31-8.
Bejarano-Roncancio JJ, Ramírez ME, Saurith-lópez V, Sussman-Peña OA. Conocimientos, actitudes y prácticas alimentarias en pacientes diagnosticados con VIH en tratamiento farmacológico. Rev Fac Med. 2011;59(Supl 1):S3-11.
Ballester R. Adhesión terapéutica: Revisión histórica y estado de la cuestión en la infección por VIH/SIDA. Revista de Psicopatología y Psicología Clínica. 2002;7(3):151-75.
Villa IC, Vinaccia S. Adhesión terapéutica y variables psicológicas asociadas en pacientes con diagnóstico de VIH-sida. Psicología y Salud. 2006;16(1):51-62.
Sánchez-Sosa JJ, Cázares-Robles Ó, Piña-López JA, Dávila-Tapia M. Un modelo psicológico en los comportamientos de adhesión terapéutica en personas con VIH. Salud Ment. 2009;32(5):389-97.
Remor E. Valoración de la adhesión al tratamiento antirretroviral en pacientes VIH+. Psicothema. 2002;14(2):262-7.
Piña-López JA, Rivera-Icedo BM, Corrales-Rascón AE, Mungaray-Padilla K, Valencia-Vidrio MA. ¿Influye el tiempo de infección en meses sobre los predictores psicológicos de comportamientos de adhesión en una muestra de pacientes VIH+? Ter Psicológica. 2006 [cited 2017 Mar 28];24(2):183-90. Available from: https://goo.gl/as99Rw.
Piña-López JA, Sánchez-Sosa JJ, Fierros LE, Ybarra JL, Cázares-Robles Ó. Variables psicológicas y adhesión en personas con VIH: Evaluación en función del tiempo de infección. Ter Psicológica. 2011;29(2):149-57. http://doi.org/fzcqmh.
Piña-López JA, Dávila-Tapia M, Sánchez-Sosa JJ, Togawa C, Cázares-Robles Ó. Asociación entre los niveles de estrés y depresión y la adhesión al tratamiento en personas seropositivas al VIH en Hermosillo, México. Rev Panam Salud Pública. 2008;23(6):377-83. http://doi.org/d4td84.
González-Ramírez MT, Ybarra-Sagarduy JL, Piña-López JA. Relaciones sociales, variables psicológicas y conductas de adherencia en adultos con VIH. Int J Psychol Psychol Ther. 2012;12(2):173-84.
Arrivillaga M, Correa D, Varela M, Holguín L, Tovar J. Variables psicológicas en mujeres diagnosticadas con VIH/SIDA: Un estudio correlacional. Univ ersitas Psychol. 2006 [cited 2017 Mar 28];5(3):659-67. Available from: https://goo.gl/I6dLPk.
Arrivillaga M, Ross M, Useche B, Alzate ML, Correa D. Social position, gender role, and treatment adherence among Colombian women living with HIV/AIDS: social determinants of health approach. Rev Panam Salud Pública. 2009;26(6):502-10. http://doi.org/fhfhfn.
Arrivillaga M, Ross M, Useche B, Springer A, Correa D. Applying an expanded social determinant approach to the concept of adherence to treatment: the case of Colombian women living with HIV/AIDS. Womens Health Isues. 2011;21(2):177-83. http://doi.org/c7cbhk.
Arrivillaga M, Springer AE, Lopera M, Correa D, Useche B, Ross MW. HIV/AIDS treatment adherence in economically better off women in Colombia. AIDS Care. 2012;24(7):929-35. http://doi.org/fxrpx9.
Remor E. Apoyo social y calidad de vida en la infección por el VIH. Atención Primaria. 2002;30(3):143-8. http://doi.org/f2km2t.
Estrada Aguilera A, Vera Pérez V. Influencia social y familiar en el comportamiento del paciente con VIH/SIDA ante su diagnóstico y manejo. Rev Hosp Jua Mex. 2004;71(1):29-35.
González-Ramírez MT, Piña-López JA. Motivos, apoyo social y comportamientos de adhesión en personas con VIH: modelamiento con ecuaciones estructurales. Univ Psychol. 2011;10(2):399-409.
Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67-74. http://doi.org/dvj9mc.
Nogués-Solán X, Sorli Redó ML, Villar García J. Instrumentos de medida de adherencia al tratamiento. An Med Interna. 2007;24(3):138-41. http://doi.org/dstvr2.
Rodríguez-Chamorro MÁ, García-Jiménez E, Amariles P, Rodríguez-Chamorro A, Faus MJ. Revisión de tests de medición del cumplimiento terapéutico utilizados en la práctica clínica. Atención Primaria. 2008;40(8):413-7. http://doi.org/fwhdcm.
Serrano-Castro PJ, Pozo-Muñoz C, Alonso-Morillejo E, Martos-Méndez MJ, Bretones-Nieto B. Factores vinculados a la adhesión al tratamiento en pacientes con epilepsia refractaria y no refractaria. Rev Neurol. 2011;53(12):721-8.
Castaño-Castrillón J, Echeverri-Rubio C, Giraldo-Cardona JF, Maldonado-Mora Á, Melo-Parra J, Meza-Orozco G, et al. Adherencia al tratamiento de pacientes hipertensos atendidos en Assbasalud ESE, Manizales (Colombia) 2011. Rev Fac Med. 2012;60(3):179-97.
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4(6):561-71. http://doi.org/cgh25q.
Beck AT, Steer RA, Carbin MG. Psychometric properties of the Beck Depression Inventory: Twenty-five years of evaluation. Clin Psychol Rev. 1988;8(1):77-100. http://doi.org/cw3bsj.
Sanz J. Recomendaciones para la utilización de la adaptación española del Inventario de Ansiedad de Beck (BAI) en la práctica clínica. Clínica y Salud. 2014;25(1):39-48. http://doi.org/b4z3.
Londoño-Arredondo NH, Rogers HL, Castilla-Tang JF, Posada-Gómez SL, Ochoa-Arizal NL, Jaramillo-Pérez M, et al. Validación en Colombia del cuestionario MOS de apoyo social. Int J Psychol Res. 2012 [cited 2017 Mar 29];5(1):142-50. Available from: https://goo.gl/GihHIO.
Martín-Alfonso L. Repercusiones para la salud pública de la adherencia terapéutica deficiente. Rev Cuba Salud Pública. 2006;32(3):1-9.
Organización Panamericana de la Salud. Adherencia a los tratamientos a largo plazo: pruebas para la acción. Washington D.C.: Organización Mundial de la Salud; 2004 [cited 2017 Mar 30]. Available from: https://goo.gl/XCi3Kb.
Nieuwkerk PT, Sprangers MA, Burger DM, Hoetelmans RM, Hugen PW, Danner SA, et al. Limited patient adherence to Highly Active Antiretroviral Therapy for HIV-1 infection in an observational cohort study. Arch Intern Med. 2001;161(16):1962-8. http://doi.org/cb8rb4.
Ballester-Arnal R. Aportaciones desde la psicología al tratamiento de las personas con infección por VIH/SIDA. Revista de Psicopatología y Psicología Clínica. 2005;10(1):53-69. http://doi.org/b42k.
Ortego C, Huedo-Medina TB, Vejo J, Llorca FJ. Adherence to highly active antiretroviral therapy in Spain. A meta-analysis. Gac Sanit. 2011;25(4):282-9. http://doi.org/ddmgrs.
Leone S, Márquez L. Relación estigma y calidad de vida en la adhesión al tratamiento de pacientes con VIH/SIDA. Eureψa. 2014;11(2):258-69.
Levine AJ, Hinkin CH, Castellon SA, Mason KI, Lam MN, Perkins A, et al. Variations in patterns of highly active antiretroviral therapy (HAART) adherence. AIDS Behav. 2005;9(3):355-62. http://doi.org/b9hfd5.
Aloisi MS, Arici C, Balzano R, Noto P, Piscopo R, Filice G, et al. Behavioral correlates of adherence to antirretroviral therapy. J Acquir Immune Defic Sydromes. 2002;31(Suppl 3):S145-8.
Varela M, Galdames S. Depresión y adhesión a terapia anti-retroviral en pacientes con infección por VIH atendidos en el Hospital San Pablo de Coquimbo, Chile. Rev Chilena Infectología. 2014;31(3):323-8. http://doi.org/b42n.
Remor E, Ulla S, Arranz P, Carrobles JA. ¿Es la percepción de control un factor protector contra el distrés emocional en personas VIH+? Psiquis. 2001;22(3):111-6.
Edo M, Ballester R. Estado emocional y conducta de enfermedad en pacientes con VIH/SIDA y enfermos oncológicos. Revista de Psicopatología y Psicología Clínica. 2006 [cited 2017 Mar 30];11(2):79-90. Available from: https://goo.gl/LnRpsk.
Soto-Ramírez LE, Herrera-Bastos E, Andrade-Vilanueva J, Calva-Mercado JJ, Gaytan-Martínez J, et al. Guía de manejo antirretroviral de las personas con VIH: Recomendaciones para el tratamiento antirretroviral en adultos. México D.F. Organización Mundial para la Salud; 2011 [cited 2017 Mar 30]. Available from: https://goo.gl/utGheC.
Consejo Nacional para la Prevención y Control del Sida. Guía de manejo antirretroviral de las personas con VIH. México D.F.: Conasida; 2014 [cited 2017 Mar 30]. Available from: https://goo.gl/Z5K7Ik.
Borrás F. SIDA: Aportaciones desde la psiconeuroinmunología. Rev de Psicol Gral y Aplic. 1994;47(2):225-9.
De Flores T. Impacto emocional y cambios inmunológicos en la notificación diagnóstica de seropositividad. Ann Psicol. 1994;10(2):135-43.
Klinger JC, Herrera JA, Díaz ML, Jhann AA, Ávila GI, Tobar CI. La psiconeuroinmunología en el proceso salud enfermedad. Colomb Med. 2005 [cited 2017 Mar 30];36(2):120-9. Available from: https://goo.gl/TMZvmJ.
Watt MH, Maman S, Earp JA, Eng E, Setel PW, Golin CE, et al. “It’s all the time in my mind”: Facilitators of adherence to antiretroviral therapy in a Tanzanian setting. Soc Sci Med; 2009;68(10):1793-800. http://doi.org/bmrm68.
Wu X, Chen J, Huang H, Liu Z, Li X, Wang H. Perceived stigma, medical social support and quality of life among people living with HIV/AIDS in Hunan, China. Appl Nurs Res. 2015;28(2):169-74. http://doi.org/f697t4.
Kelly JD, Hartman C, Graham J, Kallen MA, Giordano TP. Social support as a predictor of early diagnosis, linkage, retention, and adherence to HIV care: Results from the steps study. J Assoc Nurses AIDS Care. 2014;25(5):405-13. http://doi.org/f6pbxm.
Heath K, Singer J, O´Shaughnessy M, Montaner JS, Hogg RS. Intentional Nonadherence due to adverse symptoms associated with antiretroviral therapy. J Acquir Defic Syndr. 2002;31(2):211-7. http://doi.org/btw5dz.
Margulies S, Barber N, Recoder ML. VIH-SIDA y “Adherencia” al tratamiento: Enfoques y perspectivas. Antípoda. 2006;3:281-300.
Arrivillaga-Quintero M. Análisis de las barreras para la adherencia terapéutica en mujeres colombianas con VIH/sida: cuestión de derechos de salud. Salud Publica Mex. 2010;52(4):350-6. http://doi.org/dh6ck7.
Posse M, Meheus F, van Asten H, van der Ven A, Baltussen R. Barriers to access to antiretroviral treatment in developing countries: a review. Trop Med Int Heal. 2008;13(7):904-13. http://doi.org/bm652t.
Cómo citar
APA
ACM
ACS
ABNT
Chicago
Harvard
IEEE
MLA
Turabian
Vancouver
Descargar cita
CrossRef Cited-by
1. Mónica Narváez, Liliane Lins-Kusterer, Juliet Valdelamar-Jiménez, Carlos Brites. (2022). Quality of Life and Antiretroviral Therapy Adherence: A Cross-Sectional Study in Colombia. AIDS Research and Human Retroviruses, 38(8), p.660. https://doi.org/10.1089/aid.2021.0233.
2. Carlos Jesús Canova Barrios. (2021). Calidad de vida relacionada con la salud en sujetos con VIH. Investigación en Enfermería: Imagen y Desarrollo, 23 https://doi.org/10.11144/Javeriana.ie23.cvrs.
3. Tadele Amare Zeleke, Tadesse Awoke Ayele, Zewditu Abdissa Denu, Lillian Mwanri, Telake Azale. (2025). The effect of depression on antiretroviral drug non-adherence among women living with HIV in Gondar health facilities, northwest Ethiopia: a prospective cohort study. Frontiers in Psychiatry, 16 https://doi.org/10.3389/fpsyt.2025.1488183.
4. Firhan Nurfalah, Sri Yona, Agung Waluyo. (2019). The relationship between HIV stigma and adherence to antiretroviral (ARV) drug therapy among women with HIV in Lampung, Indonesia. Enfermería Clínica, 29, p.234. https://doi.org/10.1016/j.enfcli.2019.04.138.
Dimensions
PlumX
Visitas a la página del resumen del artículo
Descargas
Licencia
Derechos de autor 2017 Revista de la Facultad de Medicina

Esta obra está bajo una licencia Creative Commons Reconocimiento 3.0 Unported.
-


















