


Publicado
Evaluación de la prescripción profiláctica de omeprazol y ranitidina mediante la identificación de factores de riesgo de sangrado gastrointestinal
Evaluation of prophylactic prescription of omeprazole and ranitidine by identifying risk factors for gastrointestinal bleeding
DOI:
https://doi.org/10.15446/rcciquifa.v46n1.67289Palabras clave:
Sangrado gastrointestinal, riesgo, profilaxis, inhibidores de secreción ácida, antiulcerosos (es)Gastrointestinal bleeding, risk, prophylaxis, acid secretion inhibitors, acid suppression, antiulcer agents (en)
controversial. Con el fin de evaluar la pertinencia de este grupo de medicamentos en conformidad con el riesgo de sangrado gastrointestinal medido por la escala de Herzig et al. {Risk factors for nosocomial gastrointestinal bleeding and use of acid-suppressive
medication in non-critically ill patients, J. Gen. Intern. Med., 28(5), 683-690 (2013)}, se realizó un estudio observacional descriptivo longitudinal con recolección retrospectiva de la información, el cual incluyó todos los pacientes mayores de 18 años sin sangrado gastrointestinal y con más de tres días de hospitalización, en el servicio de medicina interna de un hospital de tercer nivel de Bogotá. Según esta escala, el 64% de los pacientes se clasificó en bajo riesgo, el 22,3% en medio-bajo, el 6,7% en medioalto,
y el 6,7% en alto. La prescripción profiláctica de inhibidores de la secreción ácida
se realizó en el 67% de los pacientes de bajo riesgo, en el 57% de los de medio-bajo y en el 100% de los pacientes de riesgo medio-alto y alto. Cerca de la mitad (55,35%) de los pacientes recibieron un antiulceroso sin requerirlo; por lo tanto, se recomienda
realizar actividades educativas dirigidas al personal prescriptor, con el fin de hacer un uso adecuado de este grupo de medicamentos.
Current information on the use of inhibitors of the production of hydrochloric acid (proton-pump inhibitor (PPI) ATC A02BC and histamine H2 receptor antagonists (Anti H2) ATC A02BC) in non-critical patients for the prophylaxis of stress ulcers is controversial. A descriptive longitudinal observational study with a retrospective collection of information, that included patients over 18 years with more than three days of hospitalization in internal medicine, without active gastrointestinal bleeding using the scale of Herzig et al. {Risk factors for nosocomial gastrointestinal bleeding and use of acid-suppressive medication in non-critically ill patients, J. Gen. Intern. Med., 28(5), 683-690 (2013)}, to assess the risk gastrointestinal bleeding was carried out. According to the risk score, patients were classified 64% as low risk, 22.3% medium-low risk, 6.7% medium-high risk and 6.7% high risk. Prophylactic prescription inhibiting acid secretion was performed in 67% of patients at low risk, 57% in medium-low risk and 100% for patients with medium-high and high risk. More than half (55.33%) of the patients received a PPI/anti H2 without requiring it. Educational activities are recommended to the prescribing staff in order to make proper use of this group of drugs.
Recibido: 8 de septiembre de 2016; Aceptado: 23 de abril de 2017
RESUMEN
La información actual sobre el uso de inhibidores de la producción de ácido clorhídrico (inhibidores de bomba de protones y antagonistas de los receptores de histamina H2), en pacientes no críticos hospitalizados para la profilaxis de úlceras por estrés es controversial. Con el fin de evaluar la pertinencia de este grupo de medicamentos en conformidad con el riesgo de sangrado gastrointestinal medido por la escala de Herzig et al. {Risk factors for nosocomial gastrointestinal bleeding and use of acid-suppres-sive medication in non-critically ill patients, J. Gen. Intern. Med, 28(5), 683-690 (2013)}, se realizó un estudio observacional descriptivo longitudinal con recolección retrospectiva de la información, el cual incluyó todos los pacientes mayores de 18 años sin sangrado gastrointestinal y con más de tres días de hospitalización, en el servicio de medicina interna de un hospital de tercer nivel de Bogotá. Según esta escala, el 64% de los pacientes se clasificó en bajo riesgo, el 22,3% en medio-bajo, el 6,7% en medio-alto, y el 6,7% en alto. La prescripción profiláctica de inhibidores de la secreción ácida se realizó en el 67% de los pacientes de bajo riesgo, en el 57% de los de medio-bajo y en el 100% de los pacientes de riesgo medio-alto y alto. Cerca de la mitad (55,35%) de los pacientes recibieron un antiulceroso sin requerirlo; por lo tanto, se recomienda realizar actividades educativas dirigidas al personal prescriptor, con el fin de hacer un uso adecuado de este grupo de medicamentos.
Palabras clave:
Sangrado gastrointestinal, riesgo, profilaxis, inhibidores de secreción ácida, antiulcerosos.SUMMARY
Current information on the use of inhibitors of the production of hydrochloric acid (proton-pump inhibitor (PPI) ATC A02BC and histamine H2 receptor antagonists (Anti H2) ATC A02BC) in non-critical patients for the prophylaxis of stress ulcers is controversial. A descriptive longitudinal observational study with a retrospective collection of information, that included patients over 18 years with more than three days of hospitalization in internal medicine, without active gastrointestinal bleeding using the scale of Herzig et al. {Risk factors for nosocomial gastrointestinal bleeding and use of acid-suppressive medication in non-critically ill patients, J. Gen. Intern. Med., 28(5), 683-690 (2013)}, to assess the risk gastrointestinal bleeding was carried out. According to the risk score, patients were classified 64% as low risk, 22.3% medium-low risk, 6.7% medium-high risk and 6.7% high risk. Prophylactic prescription inhibiting acid secretion was performed in 67% of patients at low risk, 57% in medium-low risk and 100% for patients with medium-high and high risk. More than half (55.33%) of the patients received a PPI/anti H2 without requiring it. Educational activities are recommended to the prescribing staff in order to make proper use of this group of drugs.
Keywords:
Gastrointestinal bleeding, risk, prophylaxis, acid secretion inhibitors, acid suppression, antiulcer agents.INTRODUCCIÓN
Actualmente, existe información controversial en relación con el uso de inhibidores de la producción de ácido clorhídrico, inhibidores de la bomba de protones (IBP) y antihistamínicos H2 (antiH2), en pacientes no críticos hospitalizados para la profilaxis de úlceras por estrés [1-3]. Esto en razón a que estas lesiones se producen en mayor proporción en pacientes hospitalizados en la Unidad de Cuidados Intensivos (UCI) [4], con un alto riesgo de presentar sangrado gastrointestinal (SGI). Eventualmente, lo anterior puede conllevar a inestabilidad hemodinámica manifestada como hipotensión, taquicardia, falla respiratoria o anemia, entre otras [5], por lo que el tratamiento profiláctico en este grupo de pacientes es de gran importancia. No obstante, en ocasiones esta práctica no tiene relación con la prevención de ulceras por estrés en pacientes no críticos hospitalizados [6]; más bien, se prescriben indiscriminadamente en un rango del 30% al 50% de los pacientes admitidos, a pesar de no tener evidencia de un beneficio en esta población en específico [7,8], por lo cual se ha llegado a concluir que hay una sobreutilización de los IBP y antiH2 [9]. Se ha identificado que la causa, la mayoría de las veces, es una evaluación inapropiada para la prescripción de estos medicamentos [10], y se ha sugerido como solución la realización de protocolos que influyan en la toma de decisiones en el momento de indicarlos para darles un mejor uso [11]. De esta discusión surgió la propuesta de Herzig et al., un sistema de puntuaciones que ayuda a determinar el riesgo clínico de SGI en los pacientes no críticos hospitalizados, con base en la identificación de los factores más relevantes [12]. Además, dicho sistema de puntuaciones se convierte en una herramienta que permite clasificar a los pacientes por grupos de riesgo, de modo que serían los pacientes de más alto riesgo los que se beneficiarán con el uso de omeprazol (A02BC01) o ranitidina (A02BA02) [13].
En el contexto colombiano, no son muchos los estudios que se han elaborado relacionados con el tema [14-16], por tal razón, el presente estudio descriptivo retrospectivo pretende ampliar un poco más la información existente, con el propósito de contribuir, en alguna medida, a generar mejores patrones de prescripción de la terapia profiláctica con los inhibidores de la secreción ácida, a partir de la identificación de los factores de riesgo de SGI en pacientes no críticos hospitalizados, descritos en el sistema de puntaciones elaborado y validado por Herzig et al. [ 12].
METODOLOGÍA
Se realizó un estudio observacional descriptivo de corte longitudinal con recolección retrospectiva de la información. Corresponde a un estudio de utilización de medicamentos sobre hábitos de prescripción. La información se obtuvo de las historias clínicas del servicio de medicina interna de un hospital de alta complejidad del departamento de Cundinamarca, con sede principal en Bogotá D.C., de enero del 2015 a junio del 2015. Las historias clínicas se revisaron por medio del software Dinámica Gerencial Hospitalaria® (SYAC S.A.).
En la investigación se incluyeron pacientes mayores de 18 años, ingresados al servicio de medicina interna y quienes permanecieron hospitalizados por más de tres días, con el fin de asegurar que su tratamiento provenía exclusivamente de la prescripción intra-hospitalaria. Se excluyeron pacientes con hemorragia gastrointestinal (ICD-9-CM), así como pacientes que presentaran sangrado gastrointestinal (definido como presencia de cualquiera de las siguientes: hematemesis, aspirado nasogástrico con material tipo "cunchos de café", melena o hematoquecia dentro de las 24 horas después de la admisión o durante la estancia en la UCI), y pacientes con cateterización cardíaca, por ser pacientes expuestos a altas dosis de antiagregantes plaquetarios y anticoagulantes.
Para el cálculo de la muestra se utilizó la siguiente fórmula [17]:

Dado que la prevalencia de prescripción de omeprazol y ranitidina es desconocida, se asume un valor de 0,5 (50%), el cual maximiza el tamaño muestral [17], y un error aleatorio del 10%. Se obtuvo un tamaño de muestra de 105 pacientes, los cuales se seleccionaron de manera aleatoria del listado del censo diario de pacientes.
Estratificación del riesgo
Con base en el estudio de Herzig et al. [ 12], se tomaron los criterios (véase la tabla 1) que conforman el sistema de puntuación para riesgo clínico de sangrado gastrointestinal en pacientes no críticos, hospitalizados fuera de la Unidad de Cuidados Intensivos (UCI), con el fin de identificarlos en la revisión de las historias clínicas de los pacientes seleccionados. La puntuación final corresponde a la sumatoria de los puntos que cada factor de riesgo representa, con lo cual, posteriormente, se clasificaron los pacientes por el tipo de riesgo de sangrado gastrointestinal de la siguiente manera: riesgo bajo (≤ 7 puntos), riesgo medio-bajo (8-9 puntos), riesgo medio-alto (10-11 puntos), y riesgo alto (≥ 12 puntos).
Tabla 1: Sistema de puntuación para riesgo clínico de sangrado gastrointestinal de Herzig et al.
[
12] en pacientes hospitalizados fuera de la Unidad de Cuidados Intensivos (UCI).

Además de emplear el sistema de puntuaciones para identificar los factores de riesgo de SGI y clasificar a los pacientes por el grupo de riesgo, se extrajo de las historias clínicas el momento en el que fueron prescritos algunos de los inhibidores de la secreción ácida, a fin de encontrar la relación entre el grupo de riesgo y la prescripción para cada uno de los grupos de riesgo antes descritos.
Este tipo de investigación explora por medio de la observación y la recogida de datos en las historias clínicas de los pacientes, por tanto, no implica ninguna intervención ni modificación intencionada de variables biológicas, fisiológicas, psicológicas o sociales en seres humanos. Según la Resolución 8430 de Octubre 4 de 1993 del Ministerio de Salud de Colombia, esta es una investigación sin riesgo. Se consideró la Ley 1581 de 2012 y su Decreto reglamentario 1377 de 2013, relacionados con protección de datos personales. El acceso a la información, a las historias clínicas y al protocolo, en su integridad fue puesto a consideración de los comités de investigaciones y de ética institucionales, los cuales aprobaron el protocolo. Este estudio sigue los lineamientos internacionales de investigación del código de Nuremberg, la declaración de Helsinki y el informe BELMONT.
RESULTADOS Y DISCUSIÓN
Se seleccionaron 141 historias clínicas que cumplían criterios de inclusión, de las cuales 38 se excluyeron por: diagnóstico de hemorragia gastrointestinal (HGI), cateterismo cardiaco, o sangrado gastrointestinal (SGI) en la Unidad de Cuidados Intensivos (UCI), estancia de hospitalización menor a tres días y por ser de consulta externa. La figura 1 muestra de manera detallada este resultado. Finalmente, 103 historias clínicas (61 hospitalizados en el servicio de medicina interna y 42 de interconsulta a medicina interna) quedaron disponibles para la realización del estudio.
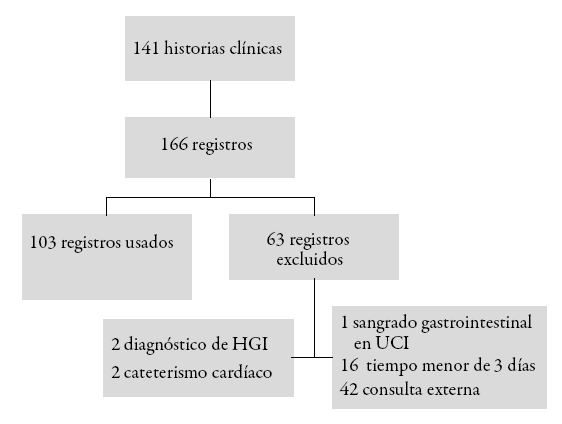
Figura 1: Algoritmo de inclusión-exclusión.
La edad promedio de los pacientes fue de 33 años (rango 18-88 años), y el 51% eran mujeres. El 69% (71/103) del total de los pacientes ingresados a medicina interna recibieron un inhibidor de la secreción ácida de manera profiláctica. De los pacientes hospitalizados en el servicio de medicina interna y los pacientes evaluados por interconsulta por este servicio, de acuerdo con el riesgo evaluado por la escala de Herzig et al. [ 12], el 64% (66/103) se clasificó como de riesgo bajo, mientras que el 22% (23/103) de riesgo bajo-medio (véase la figura 2).
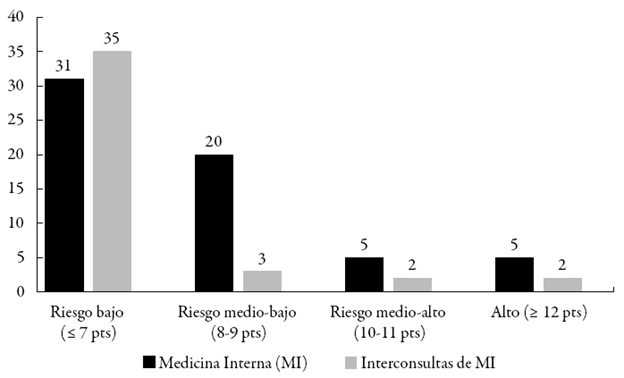
Figura 2: Clasificación de los pacientes según el riesgo de SGI.
Durante la hospitalización, el 39% (41/103) de los pacientes recibieron omeprazol, el 20% (21/103) recibieron ranitidina, y el 9% (9/103) recibieron ambos, ya fuera por reemplazo (7%), o bien por duplicidad de prescripción (2%). Al momento del alta, al 11% (11/103) de los pacientes se les prescribió omeprazol, y a un 1% (1/103) ranitidina; de estos 12, en un 75% no se evidenció en la historia clínica alguna de las indicaciones aprobadas para estos medicamentos.
Con relación a la prescripción de inhibidores de la secreción ácida según el grupo de riesgo, se encontró que al 67% (44/66) de los pacientes de riesgo bajo, y al 57% (13/23) de los de riesgo medio-bajo recibieron profilaxis. Para los grupos de alto riesgo, el 100% recibió profilaxis, tal como se observa en la figura 3.
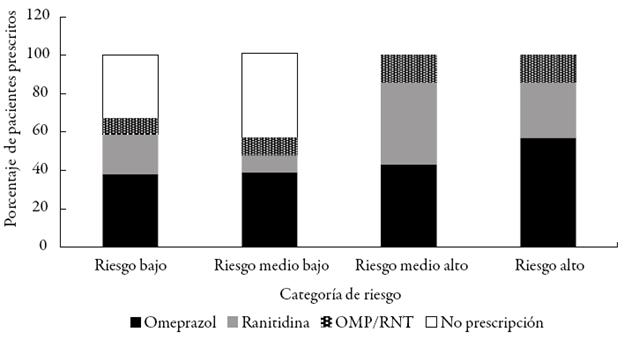
Figura 3: Prescripción de inhibidores de secreción ácida según grupo de riesgo.
El sangrado gastrointestinal intrahospitalario (SGIH) es una fuente importante de morbilidad y mortalidad evitable en este ámbito [12], la cual aumenta significativamente el tiempo de hospitalización [18]. Sin embargo, la profilaxis con inhibidores de la secreción ácida para esta condición se ha recomendado en guías de uso de estos medicamentos para pacientes hospitalizados en la UCI, debido a que existe evidencia en varios estudios que muestran cómo el uso profiláctico de omeprazol y ranitidina ha reducido relativamente el riesgo entre un 29% y un 61% en este grupo de pacientes [19,20], mientras que en pacientes hospitalizados fuera de la UCI se ha cuestionado el uso de estos medicamento, dado el bajo riesgo, en general, de estos pacientes de presentar SGIH [6,20-22]; así sucedió en este estudio, en el que se presentó en un 8% de los 103 pacientes incluidos en los registros analizados.
De este 8%, se observó que el 25% se clasificó como pacientes de alto riesgo, y el 75% como de los dos grupos de menor riesgo, lo que supone poco valor predictivo de la propuesta de Herzig et al. [ 12]. Esto pudo suceder por diferencias en las condiciones clínicas de los pacientes hospitalizados (estadio de la patología de base, estado nutricional previo, aspectos culturales) que modifican esa probabilidad, y no fueron contempladas en el estudio en mención. También se puede deber a un tamaño de muestra insuficiente que produce estos resultados solo por azar, y dada la naturaleza observacional de este estudio, no es posible determinar si el porcentaje de sangrado hubiese sido mayor en pacientes que recibieron alguno de los inhibidores de la secreción ácida durante la hospitalización. A pesar de lo anterior, esta investigación aporta al conocimiento en condiciones locales.
La idea de aplicar el sistema de puntuaciones es estar en capacidad de identificar en los pacientes los factores de riesgo que los predisponen a presentar SGI en el periodo de hospitalización, y con esto realizar una clasificación por tipo de riesgo a fin de justificar el uso profiláctico de inhibidores de la secreción ácida, lo cual permita disminuir tal riesgo en los pacientes del grupo con más alto puntaje y evite el uso indiscriminado de estos medicamentos en los pacientes del grupo de más bajo riesgo. Según el estudio de Herzig et al. [ 12], el número necesario a tratar (NNT) para riesgo bajo y medio bajo es superior a 500, con el fin de prevenir un episodio de sangrado gastrointestinal nosocomial, con lo cual se demuestra la poca utilidad de utilizar inhibidores de secreción ácida en pacientes hospitalizados con estas condiciones [12]. Sin embargo, y coincidiendo con los resultados de otros estudios [7,8,10], más del 50% de los pacientes analizados en esta investigación recibieron alguno de los inhibidores de secreción ácida en cada clasificación de riesgo (véase la figura 3), incluyendo el grupo de riesgo más bajo, de manera que, en promedio, fueron más prescritos los inhibidores de la bomba de protones (44%, en el que el 100% fue omeprazol) con respecto a los antagonistas de los receptores de histamina-2 (25% en el que el 100% fue ranitidina). Estos últimos resultados comparados con el estudio de Bernal y López difieren, puesto que el porcentaje de prescripción de Ranitidina (65,91%) es mayor que el de omeprazol (27,27%) [15]. Si bien el estudio fue aplicado en la misma institución, se puede concluir que el patrón de prescripción de estos medicamentos cambió, pues para la época la ranitidina estaba incluida en el plan de beneficios del sistema de salud, mientras que el omeprazol, recién ingresado al mercado, aún no contaba con financiación del Estado.
Por otra parte, es importante evaluar si el modelo de Herzig et al. [ 12] es aplicable al medio colombiano, dadas las diferencias en las condiciones y los factores determinantes en salud que existen en tal estudio con respecto a este. Por ejemplo, al realizar la comparación del estudio de Herzig et al. [ 12] frente a un estudio de características similares realizado en Colombia por Bernal y López [15], se encontraron diferencias en los factores de riesgo predisponentes para el sangrado gastrointestinal, en los que algunos de este último -comparado con el primero- que aparecen como factores predisponentes, no aparecen en el sistema de puntuación, y algunos que parecen prevenir el uso aparecen como factores de alto riesgo en el sistema de puntuación de Herzig et al. [ 12], tal como se puede apreciar en la tabla 2.
Tabla 2: Comparación de factores de riesgo para sangrado gastrointestinal de dos estudios.

Estos hallazgos se pueden explicar, principalmente, por las diferencias en la formación académica de los médicos, la disponibilidad de recursos terapéuticos de la época y la presión asistencial que obliga a tomar decisiones sin mucho tiempo de razonamiento clínico.
El uso indiscriminado de estos medicamentos, sin una guía de manejo, puede conllevar al empeoramiento de la salud de los pacientes, puesto que no se tiene en cuenta la relación entre el uso y el riesgo asociado que cualquier medicamento posee, incluyendo las potenciales interacciones o contraindicaciones, así como el costo que el uso inadecuado pueda conllevar, no solo por el precio del medicamento per se, sino por las posibles implicaciones en la salud del paciente que esto pueda generar.
En conclusión, al aplicar el sistema de clasificación de riesgo de sangrado gastrointestinal de Herzig et al. [ 12], se encontró que al menos la mitad de los pacientes hospitalizados recibieron omeprazol/ranitidina sin requerirlo, dado su bajo puntaje de riesgo de SGIH. Se requiere de emplear estrategias educativas dirigidas a los médicos prescriptores, con el fin de que se logre una unidad de criterio frente al uso profiláctico de estos medicamentos. Para estar en capacidad de proferir con certeza estas últimas afirmaciones y otras discutidas anteriormente, se considera importante la realización de otros estudios de mayor profundidad, y en diferentes instituciones de salud, los cuales proporcionen una clara definición de los factores de mayor riesgo clínico que predisponen a la aparición de sangrado gastrointestinal en pacientes hospitalizados fuera de la UCI. Asimismo, una posterior validación de un sistema de puntuación de riesgo para este fin en el contexto colombiano, de la que resulte una guía más objetiva para los clínicos y, así, se genere una prescripción más individualizada y racional de estos medicamentos.
AGRADECIMIENTOS
Los autores agradecen a las autoridades científicas y administrativas del Hospital Universitario de La Samaritana, a la Universidad Nacional de Colombia -en especial al Centro de Información de Medicamentos de la Universidad Nacional (CIMUN)-, por su apoyo en la resolución de consultas durante la realización del estudio.
REFERENCIAS
Referencias
(1) D.J. Cook, B.K. Reeve, G.H. Guyatt, D.K. Heyland, L.E. Griffith, L. Buckinghamy, et al., Stress ulcer prophylaxis in critically ill patients. Resolving discordant meta-analyses, JAMA, 275(4), 308-314 (1996).
(2) C. Durand, K.C. Willett, A.R. Desilets, Proton pump Inhibitor use in Hospitalized patients: Is Overutilization Becoming a problem? Clinical Medicine Insights, Gastroenterology, 51, 65-76 (2012).
(3) M. Sheikh-Taha, S. Alaeddine, J. Nassif, Use of acid suppressive therapy in hospitalized non-critically ill patients, World J. Gastrointest. Pharmacol. Ther., 3(6), 93-96 (2012).
(4) B. Anderberg, R. Sjodahl, Prophylaxis and management of stress ulcers, Scand. J. Gastroenterol. Suppl., 110, 101-104 (1985).
(5) M.B. Fennerty, Pathophysiology of the upper gastrointestinal tract in the critically ill patient: rationale for the therapeutic benefits of acid suppression, Crit. Care Med. 30, S351-S355 (2002).
(6) Therapeutic ASHP, Guidelines on Stress Ulcer Prophylaxis. ASHP Commission on Therapeutics and approved by the ASHP Board of Directors on November 14, 1998, Am. J. Health Syst. Pharm., 56(4), 347-379 (1996).
(7) F. Parente, C. Cucino, S. Gallus, S. Bargiggia, S. Greco, L. Pastore, et al., Hospital use of acidsuppressive medications and its fall-out on prescribing in general practice: a 1-month survey, Aliment. Pharmacol. Ther., 17, 1503-1506 (2003).
(8) R.J. Nardino, R.J. Vender, P.N. Herbert, Overuse of acid-suppressive therapy in hospitalized patients, Am. J. Gastroenterol., 95, 3118-3122 (2000).
(9) S.J. Herzig, B.P. Vaughn, M.D. Howell, L.H. Ngo, E.R. Marcantonio, Acid-suppressive medication use and the risk for nosocomial gastrointestinal bleeding, Arch. Intern. Med., 171(11), 991-997 (2011).
(10) J.J. Heidelbaugh, A.H. Kim, R. Chang, P.C. Walker, Overutilization of protonpump inhibitors: what the clinician needs to know, Ther. Adv. Gastroenterol., 5(4), 219-232 (2012).
(11) J.J. Lopez, C. Bustamante, Utilizacion profilactica de antiulcerosos en pacientes de tres hospitales de la ciudad de Bogota, Rev. Colomb. Cienc. Quím. Farm., 29, 32-39 (2000).
(12) S.J. Herzig, M.B. Rothberg, D.B. Feinbloom, M.D. Howell, K.K.L. Ho, L.H. Ngo, et al., Risk factors for nosocomial gastrointestinal bleeding and use of acidsuppressive medication in non-critically ill patients, J. Gen. Intern. Med., 28(5), 683-690 (2013).
(13) S. Nickoloff, Capsule commentary on Herzig et al. risk factors for nosocomial gastrointestinal bleeding and use of acid-suppressive medication in non-critically ill patients, J. Gen. Intern. Med., 28(5), 710 (2013).
(14) J.E. Machado-Alba, J.D. Castrillon-Spitia, M.J. Londono-Builes, A. Fernandez- Cardona, C.F. Campo-Betancourth, S.A. Ochoa-Orozco, et al., Analisis economico de la prescripcion inadecuada de antiulcerosos en pacientes hospitalizados en institucion de tercer nivel de Colombia, Rev. Esp. de Enf. Digest., 106(2), 77-85 (2014).
(15) L.J. Bernal-Garzon, J.J. Lopez-Gutierrez, Propuesta de una guia de practica clinica para la utilizacion profilactica de antiulcerosos en el servicio de medicina interna de un hospital de tercer nivel en Bogota, Rev. Colomb. Cienc. Quím. Farm., 34(1), 24-34 (2005).
(16) J. Machado-Alba, A. Fernández, J.D. Castrillon, C.F. Campo, L.F. Echeverri, A.
Gaviria, et al., Patrones de prescripción y costos económicos de inhibidores de
bomba de protones en Colombia, Colomb. Med., 44(1), 13-18 (2013).
(17) P. Fernandez, Determinacion del tamano muestral, Cad. Atenc. Primaria, 3, 138 (1996).
(18) M.A. Qadeer, J.E. Richter, D.J. Brotman, Hospital-acquired gastrointestinal bleeding outside the critical care unit risk factors, role of acid suppression, and endoscopy findings, J. Hosp. Med., 1(1), 13-20 (2006).
(19) C.M. Wilcox, J.G. Spenney, Stress ulcer prophylaxis in medical patients: who, what, and how much? A.m. J Gastroenterol., 83, 1199-1211 (1988).
(20) J.M. Grau, J. Casademont, J. Fernandez-Sola, F. Cardellach, A. Urbano-Marquez, Prophylaxis of gastrointestinal tract bleeding in patients admitted to a general hospital ward. Comparative study of sucralfate and cimetidine, Scand. J. Gastroenterol., 28, 244-248 (1993).
(21) D.J. Cook, Fuller HD, G.H. Guyatt, J.C. Marshall, D. Leasa, R. Hall, et al., Risk factors for gastrointestinal bleeding in critically ill patients. Canadian Critical Care Trials Group, N. Engl. J. Med., 330, 377-381 (1994).
(22) F. Navab, J. Steingrub, Stress ulcer: is routine prophylaxis necessary? Am. J. Gastroenterol.,90, 708-712 (1995).
Cómo citar
APA
ACM
ACS
ABNT
Chicago
Harvard
IEEE
MLA
Turabian
Vancouver
Descargar cita
Licencia
Derechos de autor 2017 Revista Colombiana de Ciencias Químico-Farmacéuticas

Esta obra está bajo una licencia internacional Creative Commons Atribución 4.0.
El Departamento de Farmacia de la Facultad de Ciencias de la Universidad Nacional de Colombia autoriza la fotocopia de artículos y textos para fines de uso académico o interno de las instituciones citando la fuente. Las ideas emitidas por los autores son responsabilidad expresa de estos y no de la revista.
Todo el contenido de esta revista, excepto dónde está identificado, está bajo una Licencia Creative Commons de Atribución 4.0 aprobada en Colombia. Consulte la normativa en: http://co.creativecommons.org/?page_id=13















