



Publicado
Acute generalized exanthematous pustulosis related to phenytoin administration. Case report
Pustulosis exantemática aguda generalizada relacionada al uso de fenitoína
Palabras clave:
Drug eruptions, Acute Generalized Exanthematous Pustulosis, hydantoins (en)Drug eruptions, Acute Generalized Exanthematous Pustulosis, hydantoins (es)
La aparición de reacciones adversas a medicamentos del tipo pustulosis exantemática generalizada aguda es cada vez más frecuente. Se presenta el caso de una paciente de 78 años quien acude a consulta presentando unas pápulas y pústulas generalizadas en cuero cabelludo, tronco y extremidades, con estudio de histología compatible y a la que se le diagnostica pustulosis exantemática aguda generalizada (PEAG) asociada al uso de fenitoína, una medicación que puede provocar distintas reacciones cutáneas y que previamente se ha asociado a esta enfermedad. La paciente es tratada con esteroides sistémicos y la enfermedad llega a una resolución satisfactoria
Case report:
Acute generalized exanthematous pustulosis related to phenytoin administration
Palabras clave: Erupciones por medicamentos; Pustulosis exantematica aguda generalizada; hidantoínas.
Keywords: Drug eruptions, Acute Generalized Exanthematous Pustulosis, hydantoins.
Juan R Castro–Ayarza
Dermatologist
Specialist in university teaching
Faculty of Medicine
Universidad Nacional de Colombia
Bogotá, D.C. – Colombia
Eduardo Fierro
Dermatologist. Oncologist
Faculty of Medicine
Universidad Nacional de Colombia
Bogotá, D.C. – Colombia.
Corresponding author:
Juan Raul Castro Ayarza
Calle 91 #19c 62,
office 206
Phone number: 031 530 0048
Email: juanraulcastro@yahoo.com
SUMMARY
The occurrence of acute generalized exanthematous pustulosis adverse reactions to medication administration is becoming more frequent. This article reports the case of a 78-year-old woman who attended the clinic with generalized papules and pustules on the scalp, trunk and limbs, with a concordant histology study and who was diagnosed with acute generalized exanthematous pustulosis (AGEP) associated with the use of phenytoin, a medication that may cause different skin reactions and that has been previously related to this disease. The patient was treated with systemic steroids and the disease had a satisfactory outcome.
INTRODUCTIoN
Adverse drug reactions are common in in-patients and can happen in several ways, for example as the emergence of inflammatory lesions on the skin (1). Sometimes the cause of the disease can be determined from the morphology of primary lesions. Presence of pustules, in particular, may help to guide the diagnosis of some reactions to medications (1).
From the presence of pustules it is possible to make an acute generalized exanthematous pustulosis (AGEP) diagnosis, a condition related to the administration of some medications such as anticonvulsants, antimalarials and antibiotics (2). This paper presents a case of AGEP associated with the use of phenytoin.
Case Report
A 78-year-old woman from Bogotá, Colombia, with seven days of course of the disease and who had pruritic erythematous lesions in her trunk and scalp. She was experiencing fever from the fifth day, which is why she was hospitalized.
The patient had a history of a two-month-old stroke associated with a seizure she suffered two weeks prior to her hospital admission. Due to this seizure episode, the patient was administered oral phenytoin 200mg/day. She had been previously under pharmacological management for dyslipidemia and dyspepsia with acetylsalicylic acid 100mg/day, lovastatin 40mg/day and omeprazole 20mg/day.
Physical examination of the patient revealed erythematous plaques with fine scale, as well as superficial pustules on the scalp, chin, trunk, and thighs (see Figure 1). In addition, there were no signs of lymphadenopathy and lesions were easy to detach by using curettage. Likewise, a 38.1°C temperature was found in one of her records during hospitalization.


Fig 1. Dorsum. An erythematous base plaque and small pustules are observed when looking closer.
Source: Images obtained from the data collected in the study.
Blood tests showed a complete blood count with hemoglobin 9.7g/dl, hematocrit 30.0%, leukocytes 13950 mm3/dl, neutrophils 81%, lymphocytes 15%, eosinophils 1% and platelets 107000 mm3/dl, whereas transaminases and creatinine studies were normal. The haematoxylin and eosin histopathology report of a skin biopsy allowed identifying epidermis with basal layer vacuolation and subcorneal pustules, as well as dermal edema and dense superficial perivascular lymphocytic infiltrate with presence of eosinophils (see Figure 2). By relating findings made on the pustular skin to its presence in subcorneal histology with measured fever and leukocytosis an AGEP diagnosis was made, thus phenytoin administration was suspended, since it was considered as a possible cause of the reaction, instead a prednisolone dose of 0.5mg/kg administered orally during seven days was added to the patient’s treatment. Once phenytoin was suspended, pustules and fever disappeared at the second day, while the erythema lasted 10 days, then skin symptoms started to decrease until they disappeared after a month, as evidenced in the dermatology outpatient visit.

Fig 2. 10x magnified haematoxylin and eosin stain histopathology. Epidermis with presence of orthokeratosis and foci of spongiosis and superficial epidermal and superficial perivascular lymphoid infiltrate with eosinophils are observed.
Source: Image obtained from the data collected in the study.
Discussion
AGEP type adverse drug reaction was first described in 1968 when studying patients suffering psoriasis with a clinical suspicion of pustular disease. Its name was established from the French translation made in 1980, distinguishing it from acute generalized pustulosis, a postreptococcal infection (2-3).
Prevalence of AGEP by age or sex has not been determined and there are few reports describing it in children (3-5). Despite this, it is thought that it has a prevalence of 1 to 5 per million people annually, although it is likely this disease is underdiagnosed (2). In up to 90% of the cases of AGEP that have been reported the disease has been associated with a medication. In addition, there seems to be a predisposition to this condition in haplotypes like HLA-B51, HLA-DR11 and HLA-DQ3, although there is no a specificity according to the type of drug (5). On the other hand, the increase of the expression of Fas, p53 and bcl-2, which leads to keratinocyte apoptosis, could cause AGEP, although a delayed hypersensitivity reaction has also been involved (5).
Additionally, in the literature on this pathology there are studies describing some antibacterial agents, mainly macrolides and penicillins, as well as several antimycotics (6-9); likewise, a large variety of medications, including some antihypertensives (calcium antagonists, angiotensin-converting enzyme inhibitors), antiarrhythmics, anticonvulsants, antidepressants and anxiolytics, even acetaminophen, have been reported (6). The clinical profile of this disease occurs from one to three weeks after the medication has been administered, however in the case of antibiotics the occurrence average time is 2.5 days, while for other medications is 18 days (6). It is important to note that, although less frequently, AGEP has been related to viral and bacterial infections and ultraviolet light exposure (2,5,6).
Symptoms usually found in this clinical profile include fever, asthenia and adynamia. The main cutaneous manifestation of the disease is the presence of pustules, however AGEP clinical picture starts with edematous alike erythematous macules that extend mainly in intertriginous areas (2,6). Generally, pustules emerge in these areas, they do not have a follicular pattern and, sometimes, they can come together, which causes a false Nikolsky sign (2,9). Another characteristic of AGEP is the presence of lymphadenopathies (2).
Systemic involvement is reflected in the appearance of neutrophilic leukocytosis, although eosinophilia may occur in one third of cases. Aminotransferases elevation is mild, less than the double of the normal value, whereas in the creatinine clearance process a 30% reduction occurs (2,6).
However, analyzing AGEP through histopathology does not allow the medical doctor to make a diagnosis at the disease acute moment, which delays initial treatment; but histopathology findings such as the appearance of subcorneal and intraepidermal pustules with peripheral spongiosis may help in making the diagnosis. The dermis may also be affected by a superficial perivascular infiltrate containing lymphocytes, neutrophils and, to a lesser extent, eosinophils. Some mild vasculitis changes, as well as necrotic keratinocytes may also happen (2,6).
Sidoroff et al. (2) suggest five diagnostic criteria for this disease:
1.Multiple pustules, from tens to hundreds, on an erythematous base.
2.Compatible histopathological changes.
3.Fever higher than 38 °C.
4.Neutrophil count higher than 7000 mm3.
5.Spontaneous resolution in 15 days.
In their research, in order to determine the diagnosis, Sidoroff et al. (2) created a table that includes the following items: morphology (pustules, erythema, distribution and scaling); course of the disease (acute onset, fever, spontaneous resolution, mucosal involvement and neutrophil count increase higher than 7000 mm3), and histological findings (neutrophil exocytosis, papillary edema and spongious changes). Nevertheless these items are complemented by an unpractical score in terms of daily clinical practice (1,2).
Patch tests and lymphocyte transformation tests have proved useful to determine the agent involved in the disease, achieving a positivity rate of up to 80%; besides they make clear the process in the pathogenesis of T cells (3).
The course of the disease implies that its clinical scenario should disappear between 4 and 10 days, with fever and lymphadenopathy being the first symptoms to do so. On the other hand, pustules usually heal spontaneously at approximately nine days resulting in scaling after their resolution (2,6).
AGEP is a disease difficult to diagnose in its initial stage and can be confused with an infectious process. Similarly, its initial development may resemble that of a DRESS (drug rash with eosinophilia and systemic symptoms) hypersensitivity reaction to medications, where there is low or null presence of pustules. Furthermore, clinical presentation of pustular psoriasis is difficult to differentiate, but usually this is a long course disease that has frequent relapses, while subcorneal pustular dermatosis has a less acute development (1,6). Likewise, Reiter’s disease differs in joint involvement, which is not found in AGEP, and acneiform eruptions, which also have pustules, generally triggered by previous use of corticosteroids, which is a situation that constitutes the treatment of AGEP, rather than its cause (3).
Despite there are vasculitis features in AGEP, it should be histologically differentiated from vasculitis purpura. Really severe cases may look like toxic epidermal necrolysis when pustules coincide with skin scaling (1).
As it happened in the case reported here, the use of phenytoin has also been described in other AGEP cases where idiosyncratic adverse skin reactions to medications are reported, including DRESS-type hypersensitivity, maculopapular exanthema, Steven Jonhson syndrome and necrolysis toxic epidermal (10,11). In addition, there are cases reporting cross-reactivity between phenytoin and carbamazepine and between phenytoin and phenobarbital with skin manifestations (12). Nonetheless, there is only one case in the literature that reports the association of AGEP with this medication (13).
Conclusion
Quitting the use of the medication is fundamental in the treatment for AGEP. In addition, using systemic corticosteroids may be appropriate in cases with hepatic or systemic involvement. The administration of antipyretics is adequate based on the symptomatology of the patient (1).
AGEP is an adverse drugs reaction that usually finds its resolution after stopping the use of the medication causing it. There are different drugs related to its onset, including phenytoin, as seen in this case.
References
1.Mockenhaupt M. Severe drug-induced skin reactions: clinical pattern, diagnostics and therapy. J Dtsch Dermatol Ges. 2009;7(2):142-60. http://doi.org/bkps7n.
2.Sidoroff A, Halevy S, Bavinck JN, Vaillant L, Roujeau JC. Acute generalized exanthematous pustulosis (AGEP) - a clinical reaction pattern. J Cutan Pathol. 2001;28(3):113-119. http://doi.org/dbgwpb.
3.Auer-Grumbach P, Pfaffenthaler E, Soyer HP. Pustulosis acuta generalisata is a post-streptococcal disease and is distinct from acute generalized exanthematous pustulosis. Br J Dermatol. 1995;133(1):135-9. http://doi.org/bwrdpr.
4.Mengesha YM, Bennett ML. Pustular skin disorders: diagnosis and treatment. Am J Clin Dermatol. 2002;3(6):389-400. http://doi.org/dbszx9.
5.Meadows KP, Egan CA, Vanderhooft S. Acute generalizated exanthematous pustulosis (AGEP), an uncommon condition in children: case report and review of the literature. Pediatr Dermatol. 2000;17(5):399-402. http://doi.org/fkkrdk.
6.Beylot C, Doutre MS, Beylot-Barry M. Acute Generalized Exanthematous Pustulosis. Semin Cutan Med Surg. 1996;15(4):244-9.
7.Beltraminelli HS, Lerch M, Arnold A, Bircher AJ, Haeusermann P. Acute generalized exanthematous pustulosis induced by the antifungal terbinafine: case report and review of the literature. Br J Dermatol. 2005;152(4):780-3. http://doi.org/cgg5hd.
8.Heymann WR, Manders SM. Itraconazole-induced acute generalized exanthemic pustulosis. J Am Acad Dermatol. 1995;33(1):130-1. http://doi.org/c4m3dw.
9.Cuchía HJ, Arévalo NF, Castellanos HJ. Pustulosis aguda exantemática generalizada inducida por terbinafina: reporte de un caso. Rev Asoc Col Dermatol. 2008 [cited 2016 Sep 22];16(3):214-6. Available from: https://goo.gl/wGNpmf.
10.Sánchez X, Merlano C, Cruz CM. Síndrome de hipersensibilidad a medicamentos con eosinofilia y síntomas sistémicos (DRESS). Rev Asoc Col Dermatol. 2008 [cited 2016 Sep 22];16(3);208-10. Available from: https://goo.gl/ZI4DLq.
11.Maoz KB, Brenner S. Drug rash with eosinophilia and systemic symptoms syndrome: sex and the causative agent. Skinmed. 2007;6(6):271-3. http://doi.org/bw2kzk.
12.Mendiratta V, Bhushan P. Phenytoin-induced DRESS with cross-reactivity to carbamazepine in a 10-year-old Indian child. Clin Exp Dermatol. 2006;31(5):720-1. http://doi.org/dj5sxd.
13.Mallo S, Fernández E, Cardeñoso E, Ingelmo JM, Pascual AM. Pustulosis aguda exantemática generalizada: aportación de dos casos. Med Cutan Iber Lat Am. 2003 [cited 2016 Sep 22];31(4):246-51. Available from: https://goo.gl/kTkQah.
Reporte de caso:
Pustulosis exantemática aguda generalizada relacionada al uso de fenitoína
Palabras clave: Erupciones por medicamentos; Pustulosis exantematica aguda generalizada; hidantoínas.
Keywords: Drug eruptions, Acute Generalized Exanthematous Pustulosis, hydantoins.
Juan R Castro–Ayarza
Dermatólogo
Especialista en docencia universitaria
Facultad de Medicina
Universidad Nacional de Colombia
Bogotá, D.C. – Colombia
Eduardo Fierro
Dermatólogo oncólogo
Facultad de Medicina
Universidad Nacional de Colombia
Bogotá, D.C. – Colombia.
Correspondencia:
Juan Raul Castro Ayarza
Dirección postal: Calle 91 #19c 62,
cons 206
Tel: 530 0048
Correo electrónico:
juanraulcastro@yahoo.com
RESUMEN
La aparición de reacciones adversas a medicamentos del tipo pustulosis exantemática generalizada aguda es cada vez más frecuente. Se presenta el caso de una paciente de 78 años quien acude a consulta presentando unas pápulas y pústulas generalizadas en cuero cabelludo, tronco y extremidades, con estudio de histología compatible y a la que se le diagnostica pustulosis exantemática aguda generalizada (PEAG) asociada al uso de fenitoína, una medicación que puede provocar distintas reacciones cutáneas y que previamente se ha asociado a esta enfermedad. La paciente es tratada con esteroides sistémicos y la enfermedad llega a una resolución satisfactoria.
INTRODUCCIÓN
Las reacciones adversas a medicamentos son un evento frecuente en el paciente hospitalizado y pueden manifestarse en diferentes condiciones, por ejemplo la aparición de lesiones inflamatorias en la piel (1). Algunas veces el origen de la enfermedad puede determinarse a partir de la morfología de las lesiones primarias; la presencia de pústulas, en particular, puede ayudar a orientar el diagnóstico de algunas reacciones a medicamentos (1).
A partir de la aparición de las pústulas, se puede llegar al diagnóstico de pustulosis exantemática aguda generalizada (PEAG), la cual está relacionada con el uso de algunos medicamentos como anticonvulsivos, antimaláricos y antibióticos (2). En esta oportunidad, se presenta un caso de PEAG asociado al uso de fenitoína.
Reporte de caso
Mujer de 78 años proveniente de Bogotá, Colombia, que presenta siete días de evolución con lesiones eritematosas pruriginosas distribuidas en tronco, cuero cabelludo y con fiebre desde el quinto día, motivo por el cual es ingresada a hospitalización.
La paciente presenta antecedente de accidente cerebrovascular de dos meses de antigüedad asociado a un episodio convulsivo sufrido a dos semanas de la admisión y por el que recibió fenitoína oral 200mg/día. Previamente estuvo en manejo farmacológico por dislipidemia y enfermedad dispética con ácido acetilsalicílico 100mg/día, lovastatina 40mg día y omeprazol 20mg/día.
El examen físico revela unas placas eritematosas con descamación fina, junto con algunas pústulas superficiales en cuero cabelludo, mentón, tronco y muslos (ver Figura 1). No se palpan adenopatías. Las lesiones se desprenden con facilidad al raspado. Igualmente, se encuentra una temperatura de 38.1°C en uno de sus registros durante la hospitalización.
Los análisis sanguíneos muestran un hemograma con hemoglobina de 9.7g/dl, hematocrito 30.0%, leucocitos 13950 mm3/dl, neutrofilos 81%, linfocitos 15%, eosinófilos 1% y plaquetas 107000 mm3/dl, mientras que estudios de transaminasas y creatinina son normales. Se realiza biopsia de piel con reporte de histopatología en hematoxilina-eosina con epidermis con vacuolización de la capa basal y pústulas subcórneas, dermis con edema e infiltrado linfocitario perivascular superficial denso con eosinófilos (ver Figura 2). Al relacionar los hallazgos en piel con pústulas y su presencia en la histología de forma subcórnea con fiebre cuantificada y leucocitosis se realiza un diagnóstico de PEAG, por lo que el manejo con fenitoína se suspende, al considerarse como posible agente sospechoso y se adiciona prednisolona a 0.5mg/kg de peso vía oral por 7 días. La paciente presenta resolución de las pústulas y de la fiebre a los 2 días, persistencia del eritema por 10 días y luego el cuadro empieza a disminuir hasta la resolución total de los síntomas de la piel al cabo de un mes, tal como se evidencia en consulta por dermatología.


Fig 1. Lesiones dermatológicas primarias. Se observa una base con eritema y presencia de pequeñas pústulas en el acercamiento.
Fuente: Documento obtenido durante la realización del estudio
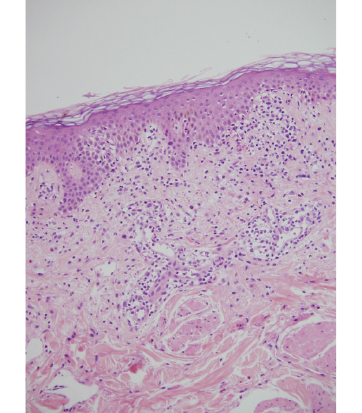
Fig 2. Histopatología con tinción de hematoxilina y eosina, aumento 10x. Epidermis con ortoqueratosis y focos de espongiosis e infiltrado linfoide epidérmico y perivascular superficial con eosinófilos.
Fuente: Documento obtenido durante la realización del estudio
Discusión
La reacción adversa a medicamentos tipo PEAG fue descrita por primera vez en 1968, cuando se investigaba sobre pacientes con psoriasis con sospecha de enfermedad pustular; su nombre fue establecido a partir de la traducción del francés en 1980, diferenciándose de la pustulosis aguda generalizada, que es una infección postreptocócica (2-3).
No se ha determinado una prevalencia de PEAG por edad o sexo y existen pocos reportes en niños (3-5). No obstante lo anterior, se cree que esta patología tiene una prevalencia de 1-5/millón al año, aunque es probable que la misma sea subdiagnosticada (2).
En los casos reportados, la PEAG se ha logrado relacionar hasta en un 90% con un medicamento; además parece haber una predisposición en haplotipos como HLA-B51, HLA-DR11, HLA-DQ3, sin que este tenga especificidad acorde al tipo de medicamento (5). Por otra parte, el aumento de la expresión de Fas, p53, y bcl-2, que conduce la apoptosis de los queratinocitos, podría causar la enfermedad, aunque una reacción de hipersensibilidad retardada también se ha visto implicada (5).
Asimismo, en la literatura sobre esta patología se han descrito algunos antibacterianos, principalmente macrólidos y penicilinas, así como varios antimicóticos (6-9). Por su parte, una gran variedad de medicamentos, algunos antihipertensivos (calcioantagonistas, inhibidores de la enzima convertidora de angiotensina), antiarrítmicos, anticonvulsivantes, antidepresivos y ansiolíticos, incluso el acetaminofén, ha sido reportada (6). La aparición del cuadro clínico se da de una a tres semanas después de administración el medicamento, sin embargo la media de los antibióticos es de 2.5 días, mientras que de otros medicamentos, 18 días (6). Es importante decir que la PEAG, en menor frecuencia, se relaciona con infecciones virales, bacterianas y los rayos ultravioleta (2,5,6).
Los síntomas con que suele acompañarse el cuadro son fiebre, astenia y adinamia. Por su parte, la aparición de pústulas es la principal manifestación cutánea de la enfermedad, sin embargo el cuadro clínico inicia sobre máculas eritematosas que se extienden principalmente en zonas intertriginosas, además de tener una apariencia edematosa (2,6). Por lo general, las pústulas usualmente emergen en estas zonas, no tienen un patrón folicular y, algunas veces, pueden confluir, lo que produce un falso signo de Nikolsky (2,9). Otra característica de la PEAG es la aparición de adenopatías (2).
El compromiso sistémico se refleja en aparición de leucocitosis con neutrofilia, aunque en un tercio de los casos podría presentarse eosinofilia. La elevación de las aminotransferasas es leve, no mayor al doble del valor normal, mientras que en la depuración de creatinina se produce una reducción del 30% (2,6).
Ahora bien, evaluar esta enfermedad por histopatología no permite diagnosticarla en el momento agudo, lo cual retrasa el tratamiento inicial. Sin embargo, hallazgos en la histopatología como la aparición de pústulas subcórneas e intraepidérmicas con espongiosis periférica, orientan el diagnóstico. La dermis también puede encontrarse comprometida con un infiltrado perivascular superficial que contiene linfocitos, neutrófilos y, en menor frecuencia, eosinofilos. También se pueden presentar algunos cambios de vasculitis leve, así como queratinocitos necróticos (2,6).
Existen 5 criterios diagnósticos para esta enfermedad, los cuales fueron sugeridos por Sidoroff et al. (2).
1.Múltiples pústulas, de decenas a cientos, sobre una base eritematosa.
2.Cambios histopatológicos compatibles.
3.Fiebre mayor a 38°C.
4.Recuento de neutrófilos mayor a 7000 mm3.
5.Resolución espontánea en 15 días.
En su investigación, Sidoroff et al. crean una tabla para definir el diagnóstico, en la que incluye los siguientes elementos: morfología (pústulas, eritema, distribución y descamación); evolución de la enfermedad (aparición aguda, fiebre, resolución espontánea, compromiso de mucosas y aumento de neutrófilos mayor a 7000), y hallazgos histológicos (exocitosis de neutrófilos, edema papilar y cambios espongióticos); sin embargo, estos elementos son complementados por un puntaje que es poco práctico para la aplicación clínica diaria (1,2).
El test de parche y el de transformación linfocítica han demostrado ser bastante útiles en lo que respecta a determinar el agente implicado, lográndose una positividad de hasta un 80%, además evidencian la importancia en la patogénesis de las células T (3).
El curso de la enfermedad implica que este cuadro debe desaparecer entre 4 y 10 días, siendo la fiebre y las adenopatías las primeras en hacerlo. Por su parte, las pústulas suelen resolverse espontáneamente aproximadamente a los nueve días, presentando una descamación posterior a su resolución (2,6).
La PEAG es una enfermedad de difícil diagnóstico en su etapa inicial y se le puede confundir con un proceso infeccioso; igualmente, su evolución inicial puede parecerse a una reacción por hipersensibilidad a medicamentos tipo DRESS (drug rash with eosinophilia and systemic symptons), en la que la presencia de pústulas es menor o inexistente. Por otra parte, la apariencia clínica de la psoriasis pustulosa es difícil de diferenciar, aunque esta suele ser de curso prolongado y recaídas frecuentes y la dermatosis pustular subcórnea tiene una evolución menos aguda (1,6). Asimismo, la enfermedad de Reiter se diferencia en el compromiso articular, el cual no se presenta en la PEAG, y en las erupciones acneiformes que también presentan pústulas, usualmente con el antecedente de uso previo de corticoides, situación que consiste en el tratamiento de la PEAG y no en su causa (3).
Aunque en la PEAG existen cambios de vasculitis, se debe diferenciar en términos de histología de la púrpura vasculítica. Los casos muy severos pueden parecer necrolisis epidérmica tóxica cuando confluyen las pústulas con desprendimiento cutáneo (1).
Tal como ocurrió en el caso de esta paciente, el uso de fenitoína también ha sido mencionado en otros casos con PEAG, reportando reacciones idiosincráticas cutáneas adversas a medicamentos, entre las que se incluyen hipersensibilidad tipo DRESS, exentema máculopapular, síndrome de Steven Jonhson y Necrolisis epidérmica tóxica (10,11). Además, hay casos de reacciones cruzadas de fenitoína con carbamazepina y fenobarbital con manifestaciones cutáneas (12). No obstante lo anterior, solo hay un caso en la literatura en el que se reporta la asociación de la PEAG con el uso de este mdicamento (13).
Conclusión
Descontinuar el medicamento es fundamental en el tratamiento; además, el uso de corticoides sistémicos puede ser indicado en los casos que presentan compromiso hepático o sistémico. La formulación de antipiréticos es adecuada según la sintomatología del paciente (1).
La PEAG es una reacción a medicamentos que suele resolverse luego de suspenderse el agente agresor. Existen diferentes fármacos relacionados con su aparición, por ejemplo la fenitoína, como se observa en este caso.
Referencias
1.Mockenhaupt M. Severe drug-induced skin reactions: clinical pattern, diagnostics and therapy. J Dtsch Dermatol Ges. 2009;7(2):142-60. http://doi.org/bkps7n.
2.Sidoroff A, Halevy S, Bavinck JN, Vaillant L, Roujeau JC. Acute generalized exanthematous pustulosis (AGEP) - a clinical reaction pattern. J Cutan Pathol. 2001;28(3):113-119. http://doi.org/dbgwpb.
3.Auer-Grumbach P, Pfaffenthaler E, Soyer HP. Pustulosis acuta generalisata is a post-streptococcal disease and is distinct from acute generalized exanthematous pustulosis. Br J Dermatol. 1995;133(1):135-9. http://doi.org/bwrdpr.
4.Mengesha YM, Bennett ML. Pustular skin disorders: diagnosis and treatment. Am J Clin Dermatol. 2002;3(6):389-400. http://doi.org/dbszx9.
5.Meadows KP, Egan CA, Vanderhooft S. Acute generalizated exanthematous pustulosis (AGEP), an uncommon condition in children: case report and review of the literature. Pediatr Dermatol. 2000;17(5):399-402. http://doi.org/fkkrdk.
6.Beylot C, Doutre MS, Beylot-Barry M. Acute Generalized Exanthematous Pustulosis. Semin Cutan Med Surg. 1996;15(4):244-9.
7.Beltraminelli HS, Lerch M, Arnold A, Bircher AJ, Haeusermann P. Acute generalized exanthematous pustulosis induced by the antifungal terbinafine: case report and review of the literature. Br J Dermatol. 2005;152(4):780-3. http://doi.org/cgg5hd.
8.Heymann WR, Manders SM. Itraconazole-induced acute generalized exanthemic pustulosis. J Am Acad Dermatol. 1995;33(1):130-1. http://doi.org/c4m3dw.
9.Cuchía HJ, Arévalo NF, Castellanos HJ. Pustulosis aguda exantemática generalizada inducida por terbinafina: reporte de un caso. Rev Asoc Col Dermatol. 2008 [cited 2016 Sep 22];16(3):214-6. Available from: https://goo.gl/wGNpmf.
10.Sánchez X, Merlano C, Cruz CM. Síndrome de hipersensibilidad a medicamentos con eosinofilia y síntomas sistémicos (DRESS). Rev Asoc Col Dermatol. 2008 [cited 2016 Sep 22];16(3);208-10. Available from: https://goo.gl/ZI4DLq.
11.Maoz KB, Brenner S. Drug rash with eosinophilia and systemic symptoms syndrome: sex and the causative agent. Skinmed. 2007;6(6):271-3. http://doi.org/bw2kzk.
12.Mendiratta V, Bhushan P. Phenytoin-induced DRESS with cross-reactivity to carbamazepine in a 10-year-old Indian child. Clin Exp Dermatol. 2006;31(5):720-1. http://doi.org/dj5sxd.
13.Mallo S, Fernández E, Cardeñoso E, Ingelmo JM, Pascual AM. Pustulosis aguda exantemática generalizada: aportación de dos casos. Med Cutan Iber Lat Am. 2003 [cited 2016 Sep 22];31(4):246-51. Available from: https://goo.gl/kTkQah.
Referencias
Mockenhaupt M. Severe drug-induced skin reactions: clinical pattern, diagnostics and therapy. J Dtsch Dermatol Ges. 2009;7(2):142-60. http://doi.org/bkps7n
Sidoroff A, Halevy S, Bavinck JN, Vaillant L, Roujeau JC. Acute generalized exanthematous pustulosis (AGEP) - a clinical reaction pattern. J Cutan Pathol. 2001;28(3):113-119. http://doi.org/dbgwpb
Auer-Grumbach P, Pfaffenthaler E, Soyer HP. Pustulosis acuta generalisata is a post-streptococcal disease and is distinct from acute generalized exanthematous pustulosis. Br J Dermatol. 1995;133(1):135-9. http://doi.org/bwrdpr
Mengesha YM, Bennett ML. Pustular skin disorders: diagnosis and treatment. Am J Clin Dermatol. 2002;3(6):389-400. http://doi.org/dbszx9
Meadows KP, Egan CA, Vanderhooft S. Acute generalizated exanthematous pustulosis (AGEP), an uncommon condition in children: case report and review of the literature. Pediatr Dermatol. 2000;17(5):399-402. http://doi.org/fkkrdk
Beylot C, Doutre MS, Beylot-Barry M. Acute Generalized Exanthematous Pustulosis. Semin Cutan Med Surg. 1996;15(4):244-9
Beltraminelli HS, Lerch M, Arnold A, Bircher AJ, Haeusermann P. Acute generalized exanthematous pustulosis induced by the antifungal terbinafine: case report and review of the literature. Br J Dermatol. 2005;152(4):780-3. http://doi.org/cgg5hd
Heymann WR, Manders SM. Itraconazole-induced acute generalized exanthemic pustulosis. J Am Acad Dermatol. 1995;33(1):130-1. http://doi.org/c4m3dw
Cuchía HJ, Arévalo NF, Castellanos HJ. Pustulosis aguda exantemática generalizada inducida por terbinafina: reporte de un caso. Rev Asoc Col Dermatol. 2008 [cited 2016 Sep 22];16(3):214-6. Available from: https://goo.gl/wGNpmf
Sánchez X, Merlano C, Cruz CM. Síndrome de hipersensibilidad a medicamentos con eosinofilia y síntomas sistémicos (DRESS). Rev Asoc Col Dermatol. 2008 [cited 2016 Sep 22];16(3);208-10. Available from: https://goo.gl/ZI4DLq
Maoz KB, Brenner S. Drug rash with eosinophilia and systemic symptoms syndrome: sex and the causative agent. Skinmed. 2007;6(6):271-3. http://doi.org/bw2kzk
Mendiratta V, Bhushan P. Phenytoin-induced DRESS with cross-reactivity to carbamazepine in a 10-year-old Indian child. Clin Exp Dermatol. 2006;31(5):720-1. http://doi.org/dj5sxd
Mallo S, Fernández E, Cardeñoso E, Ingelmo JM, Pascual AM. Pustulosis aguda exantemática generalizada: aportación de dos casos. Med Cutan Iber Lat Am. 2003 [cited 2016 Sep 22];31(4):246-51. Available from: https://goo.gl/kTkQah
Cómo citar
APA
ACM
ACS
ABNT
Chicago
Harvard
IEEE
MLA
Turabian
Vancouver
Descargar cita
Visitas a la página del resumen del artículo
Descargas
Licencia
Derechos de autor 2016 Case reports

Esta obra está bajo una licencia internacional Creative Commons Atribución-NoComercial-SinDerivadas 4.0.
Los autores al someter sus manuscritos conservarán sus derechos de autor. La revista tiene el derecho del uso, reproducción, transmisión, distribución y publicación en cualquier forma o medio.
El Formulario de Divulgación Uniforme para posibles Conflictos de Interés y los oficios de cesión de derechos y de responsabilidad deben ser entregados junto con el original.
Aquellos autores/as que tengan publicaciones con esta revista, aceptan los términos siguientes:
Los autores/as conservarán sus derechos de autor y garantizarán a la revista el derecho de primera publicación de su obra, el cual estará simultáneamente sujeto a la Licencia de reconocimiento de Creative Commons 4.0 que permite a terceros compartir la obra siempre que se indique su autor y su primera publicación en esta revista.
Los autores/as podrán adoptar otros acuerdos de licencia no exclusiva de distribución de la versión de la obra publicada (p. ej.: depositarla en un archivo telemático institucional o publicarla en un volumen monográfico) siempre que se indique la publicación inicial en esta revista.
Se permite y recomienda a los autores/as difundir su obra a través de Internet (p. ej.: en archivos telemáticos institucionales o en su página web) antes y durante el proceso de envío, lo cual puede producir intercambios interesantes y aumentar las citas de la obra publicada. (Véase El efecto del acceso abierto).























