



Publicado
Idiopathic meconium peritonitis as a surgical emergency: A case report in a newborn
Peritonitis meconial idiopática como urgencia quirúrgica. Reporte de caso en una recién nacida
Palabras clave:
Meconium, Peritonitis, Cyst, Obstruction, Postoperative, Ileus, Digestive System Abnormalities, Prenatal Diagnosis (en)Peritonitis, Meconio, Quistes, Obstrucción intestinal, Ileus, Complicaciones postoperatorias, Anomalías del sistema digestivo, Diagnóstico prenatal. (es)
La peritonitis meconial es una entidad poco descrita, propia de la edad fetal y perinatal, que se presenta de diversas formas y requiere un diagnóstico temprano. En el presente caso se realiza sospecha clínica desde el periodo antenatal, por medio de una ecografía obstétrica que muestra una masa abdominal ocupando el cuadrante derecho inferior y superior. La paciente inicia con síntomas agudos de obstrucción intestinal que mejoran luego de un abordaje quirúrgico oportuno. De acuerdo a lo anterior, se concluye que un desenlace favorable en esta patología depende de un diagnóstico temprano, pues a través del mismo se disminuyen las probabilidades de morbilidad y mortalidad
Case report:
Idiopathic meconium peritonitis as a surgical emergency: A case report in a newborn
Palabras clave: Meconium; Peritonitis; Cyst; Obstruction; Postoperative; Ileus; Digestive System Abnormalities; Prenatal Diagnosis.
Keywords: Peritonitis; Meconio; Quistes; Obstrucción intestinal; Ileus; Complicaciones postoperatorias; Anomalías del sistema digestivo; Diagnóstico prenatal.
Ana Jiménez–Uribe
Medical Intern,
Faculty of Medicine
Universidad de los Andes
Bogotá D.C. – Colombia
Armando Rojas
Chief, Pediatric Surgery Unit
Fundación Santa Fe de Bogotá
Universidad de los Andes
Bogotá D.C. – Colombia
Fernando Fierro
Pediatric Surgeon – Fundación Santa Fe de Bogotá
Universidad de los Andes
Chief, Department of Surgery – Hospital de la Misericordia
Universidad Nacional de Colombia
Bogotá D.C. – Colombia
Corresponding author:
Ana María Jiménez Uribe.
Carrera 68C #22b – 71
Edificio Alameira. Torre 2. Apto. 702
Email: am.jimenez1564@uniandes.edu.co
SUMMARY
Meconium peritonitis is a rarely described condition that is typically found in fetal and perinatal patients. It manifests in different ways and requires an early diagnosis. In this case report, a clinical suspicion of the disease was made at the antenatal period through an obstetric ultrasound scan showing an abdominal mass in both the bottom and top right quadrants. The patient initial symptoms were those of acute intestinal obstruction. Nevertheless, these symptoms improved after surgical approach was timely performed. Based on this outcome, it can be concluded that a favorable outcome to this pathology depends on its early diagnosis, since an early diagnosis decreases morbidity and mortality chances.
Introduction
Meconium peritonitis is a non-infectious chemical inflammatory response secondary to intestinal perforation in the fetal period (1). It manifests in several ways, including cyst or meconium pseudocyst (2), where the most common complication is intestinal obstruction, a surgical emergency that rapidly alters the patient’s general condition, since its symptoms include emesis, oral feed intolerance and severe dehydration, therefore it requires a rapid and specialized approach, particularly in this age group (3).
In this case, multiples studies and an early diagnosis allowing the anticipation of possible complications were required. Likewise, an analysis of the patient’s clinical condition was necessary to decide aspects such as when to perform the surgery, pre-surgical studies, surgical approach and postoperative actions that prevented the development of pathologies such paralytic ileus.
Clinical case
A 19-day-old female patient from Manizales, Colombia, who was referred by her pediatrician due to a prenatal diagnosis consisting of an ultrasound showing abdominal mass with a fixed bowel loop compatible with possible meconium peritonitis. The patient had a left femur fracture secondary to perinatal trauma caused by fetal extraction through caesarean section. There were not complications during the term of pregnancy and, apart from folic acid during the first trimester, the mother did not consume any medication. The patient was asymptomatic in the outpatient evaluation, thus her case was referred to the surgical board of the Fundación Santa Fe de Bogotá, who decided to schedule a mass resection surgery.
When the girl was 24 days old, her mother took her to the emergency department due to abdominal distention and several emetic episodes. After performing the patient’s physical assessment it was determined that she was active, her general condition was regular and that she had a left femur immobilization harness (fracture caused by labor dystocia). She had a distended abdomen, painful on palpation, with a mass located in her upper abdomen. The mass size was 5cm x 5cm approximately and it was delimited, solid and fixed. Later, this finding was confirmed through an abdominal ultrasound. In addition, it was observed that the size of the mass did not increase: it remained at 42 mm x 41 mm. Finally, an abdominal x-ray showed a calcified mass with signs of possible partial intestinal obstruction (see Figure 1).
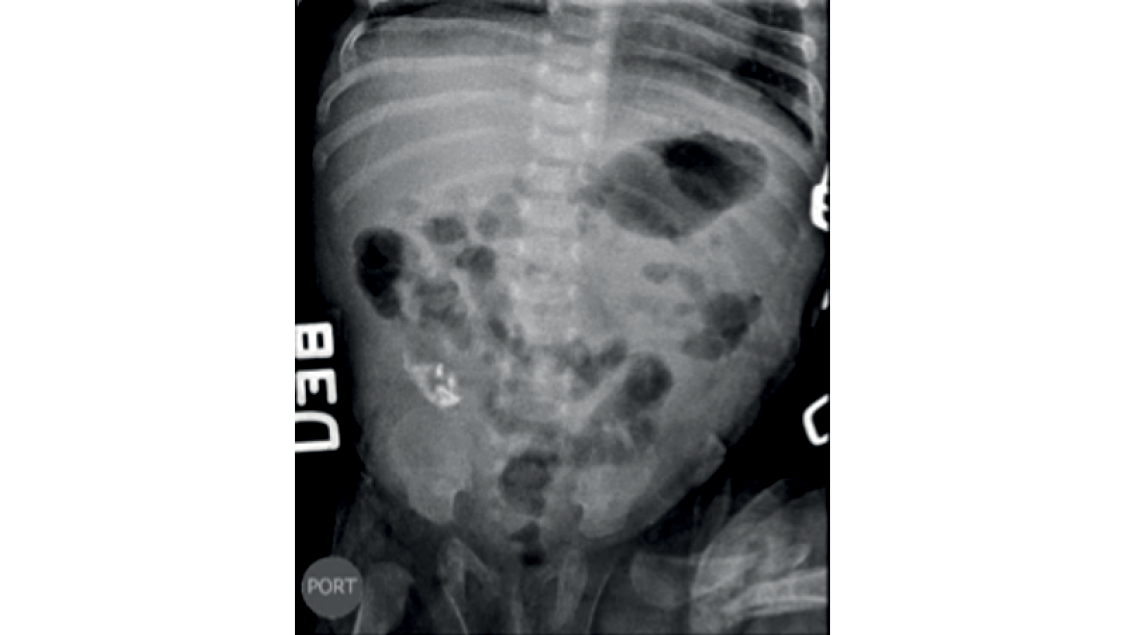
Fig 1. Abdominal x-ray. 42 mm x 41 mm calcified mass with signs of possible partial intestinal obstruction.
Source: Images obtained from the data collected in the study.
Due to the peritonitis acute clinical manifestation, the patient was sent to the operating room where the surgeons found an abdominal mass of approximately 7 x 7 cm with two cavities in the right hemiabdomen that adhered to the parietal peritoneum. The largest portion consisted of a solid mass of apparently meconium content, whereas the small portion was cystic, with non-fetid fibrinous membranes (see Figures 2a, 2b and 2c). Additionally, several adhesions in jejunoileal loops of bowel (see Figure 2d) and a 0.3 cm diameter antimesenteric intestinal perforation located at 10 cm from the ileocecal valve were observed. Finally, a 0.5 cm high broad-based Meckel’s diverticulum located at 20 cm from the ileocecal valve was also found (see Figure 2e).
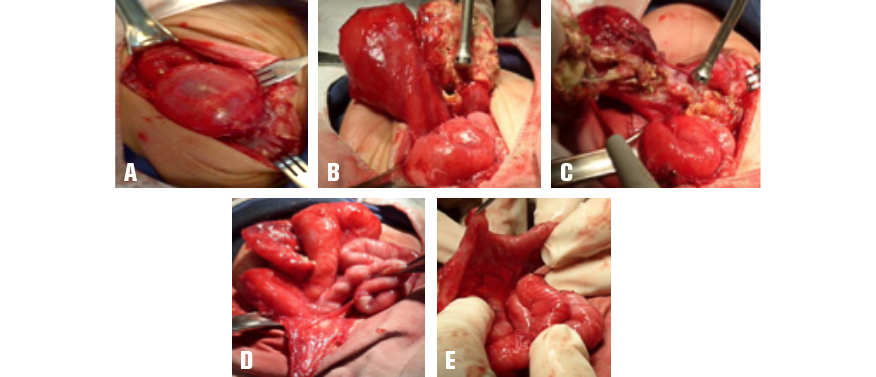
Fig 2A, 2B and 2C. 7 x 7 cm mass with two cavities: the first cavity is large and solid and has meconium content, while the second is cystic and has non-fetid fibrinous membranes. Fig 2D. Jejunoileal adhesions. Fig 2E. Antimesenteric intestinal perforation found 10 cm away from the ileocecal valve.
Source: Images obtained from the data collected in the study.
Taking these findings into account, a complete resection of the mass, a release of intestinal adhesions and a suture of the intestinal perforation, in a transverse direction, were made. Because of the size of the Meckel’s diverticulum its resection was not deemed suitable. Subsequently, pathology samples were taken and the patient was transferred to the pediatric intensive care unit, where she started receiving parenteral nutrition.
The follow-up abdominal x-ray showed a smaller amount of gas in the gastric chamber, as well as residual heterogeneous calcifications in the right hemiabdomen (see Figure 3). Pathology results allow identifying “an ileal perforation with dystrophic calcification, adhesions of richly vascularized fibrous tissue that was chronically inflamed, a peritoneal cyst associated with mixed inflammation and fibrosis, and meconium peritonitis”, which led to dismiss an intestinal duplication diagnosis.

Fig 3. Postoperative abdominal x-ray taken 24 hours after the surgery was performed.
Source: Images obtained from the data collected in the study.
In the postoperative period, the patient had a four days development ileus, which is an expected outcome from the surgical intervention and the pathology she underwent. In the fifth postoperative day she successfully tolerated oral feeding and in the sixth postoperative day she had her first liquid bowel movement, so it was decided to quit parenteral nutrition and keep feeding her orally. Since there were no complications during her recovery, the patient was discharged in the seventh postoperative day.
DiscussioN
Fortunately, the case reported here had an early diagnosis that was made in utero at week 24 of gestation from the identification of a calcified mass, which is a pathognomonic sign of meconium peritonitis (3). This allowed the pediatric surgery unit to have a prior knowledge of the case, which in turn made possible choosing an appropriate treatment plan. Furthermore, since prenatal and postnatal images of the patient were available it was possible to define the surgical approach to be performed, as well as the location and size of the mass.
The positive aspect of the physical examination was the presence of a palpable abdominal mass, which is something unusual and is commonly associated with symptoms such as abdominal distension, ascites, and intra-abdominal calcifications, among others (4). On the other hand, despite scheduling a mass resection surgery because of the asymptomatic condition of the patient, the procedure was performed as a surgical emergency due to the manifestation of acute obstructive symptoms that developed in a short time. However, the identification of the obstructive condition and its prompt medical-surgical management allowed an adequate progress and favorable development of both the surgical intervention and the postoperative recovery.
As for surgical management, a pseudocyst mass compatible with a meconium cyst was found. The mass was associated with a 0.3 cm diameter ileal perforation with necrosis in its borders and did not have underlying vascular involvement, thus resecting a part of the ileum was not necessary, a typical complication in this pathology (5,6), obtaining a better prognosis. It is important to emphasize that during the course of the disease, an added left femur fracture was always considered. Fortunately, such fracture did not cause any complications. Findings made during the surgical procedure suggested a possible intestinal duplication, since the walls of the mass resembled those of the intestine, but this option was later discarded by the pathology report.
Meconium peritonitis may be secondary to several etiologies, including intestinal atresia, volvulus, congenital flange, and meconium plug syndrome (2,7), the latter being the most common cause. A low percentage of these patients show a clinical picture of idiopathic origin, also known as simple meconium peritonitis (5), which, after discarding intestinal duplication, is the most probable diagnostic suspicion for the case reported here. This condition has been associated with transient vascular insufficiency or hypoxia of the fetal bowel, as well as with certain fetal intestinal infections, however such associations have not been yet fully established (6,5).
Regarding medical-surgical management in this case, surgical intervention instructions should be emphasized, including intestinal obstruction or persistent drainage of meconium to the abdominal cavity, which can lead to progressive abdominal distention, respiratory distress, or sepsis (7). Therefore, the surgical emergency instruction reported here was appropriate. At the beginning of the clinical picture, resecting the mass, due to its size rather than to gastrointestinal symptoms, was considered as an appropriate option in the context of an asymptomatic patient, given the risk of complications.
In conclusion, meconium peritonitis is a condition poorly described in the literature. In addition, it has a broad spectrum of both etiologies and probable short-term complications (1). Its clear method of diagnosis allows the medical staff to provide a rapid and adequate management (3). This case report shows how meconium peritonitis complications can develop acutely and unexpectedly. Fortunately, complications experienced by the patient had a favorable outcome since they were treated in a timely manner, which substantially decreased the probability of morbidity and mortality.
Conflicts of interest
The authors of this study state there were not conflicts of interests in writing this case report up (fees, personal benefits) or personal conflicts (directed towards a service or research unit) between authors and medicine manufacturers or surgical material suppliers.
Funding
None stated by the authors.
References
1.Lee YC, Chen CJ. Meconium pseudocyst: a classical and successfully treated case. J Formos Med Assoc. 2009;108(3):247-252. http://doi.org/bw85s2.
2.Tsai MH, Chu SM, Lien R, Huan HR, Luo CC. Clinical manifestations in infants with symptomatic meconium peritonitis. Pediatr Neonatol. 2009;50(2):59-64. http://doi.org/cvjpv2.
3.del Ciampo IR, Oliveira TQ, del Ciampo LA, Sawamura R, Torres LA, Augustin AE, et al. Early manifestations of cystic fibrosis in a premature patient with complex meconium ileus at birth. Rev Paul Pediatr. 2015;33(2):241-5. http://doi.org/f27fps.
4.Dirkes K, Crombleholme TM, Craigo SD, Latchaw LA, Jacir NN, Harris BH, et al. The natural history of meconium peritonitis diagnosed in utero. J Pediatr Surg. 1995;30(7):979-982. http://doi.org/dg28xd.
5.Uchida K, Koike Y, Matsushita K, Nagano Y, Hashimoto K, Otake K, et al. Meconium peritonitis: Prenatal diagnosis of a rare entity and postnatal management. Intractable Rare Dis Res. 2015;4(2):93-7. http://doi.org/bqm2.
6.Barthel ER, Speer AL, Levin DE, Naik-Mathuria BJ, Grikscheit TC. Giant cystic meconium peritonitis presenting in a neonate with classic radiographic eggshell calcifications and treated with an elective surgical approach: a case report. J Med Case Rep. 2012;6:229. http://doi.org/fzcxfb.
7.Lee G, Chandran S, Rajadurai VS. Calcified meconium pseudocyst: X-ray diagnosis of meconium peritonitis at birth. BMJ Case Rep. 2015;2015:bcr2015211052. http://doi.org/bqm3.
8.Ionescu S, Andrei B, Oancea M, Licsandru E, Ivanov M, Marcu V, et al. Postnatal Treatment in Antenatally Diagnosed Meconium Peritonitis. Chirurgia (Bucur). 2015;110(6):538-44.
Reporte de caso:
PERITONITIS MECONIAL IDIOPÁTICA COMO URGENCIA QUIRÚRGICA. REPORTE DE CASO EN UNA RECIÉN NACIDA
Palabras clave: Peritonitis; Meconio; Quistes; Obstrucción intestinal; Ileus; Complicaciones postoperatorias; Anomalías del sistema digestivo; Diagnóstico prenatal.
Keywords: Peritonitis; Meconium; Cysts; Obstruction; Ileus; Postoperative; Digestive System Abnormalities; Prenatal Diagnosis.
Ana Jiménez–Uribe
Interna de medicina
Facultad de Medicina Universidad de los Andes
Bogotá, D.C. – Colombia
Armando Rojas
Jefe de Unidad Cirugía Pediátrica Fundación Sante Fe de Bogotá Universidad de los Andes Bogotá, D.C. – Colombia.
Fernando Fierro
Cirujano Pediatra Fundación Santa Fe de Bogotá Universidad de los Andes 2Jefe Departamento Quirúrgico Hospital de la Misericordia Universidad Nacional de Colombia Bogotá, D.C. – Colombia.
Correspondencia:
Ana María Jiménez Uribe Dirección postal: Carrera 68c #22b – 71, Edi cio Alameira. Torre 2. Apto. 702 Correo electrónico: am.jimenez1564@uniandes.edu.co
RESUMEN
La peritonitis meconial es una entidad poco descrita, propia de la edad fetal y perinatal, que se presenta de diversas formas y requiere un diagnóstico temprano. En el presente caso se realiza sospecha clínica desde el periodo an- tenatal, por medio de una ecografía obstétrica que muestra una masa abdominal ocupando el cuadrante derecho inferior y superior. La pa- ciente inicia con síntomas agudos de obstruc- ción intestinal que mejoran luego de un aborda- je quirúrgico oportuno. De acuerdo a lo anterior, se concluye que un desenlace favorable en esta patología depende de un diagnóstico tem- prano, pues a través del mismo se disminuyen las probabilidades de morbilidad y mortalidad.
SUMMARY
Meconium peritonitis is an entity that has been rarely described and which is typically found in fetal and perinatal patients. It manifests in different ways and requires an early diagno- sis. In this case, a clinical suspicion of this dis- ease is made at the antenatal period through an obstetric ultrasound scan showing an ab- dominal mass in both the bottom and top right quadrants. The patient initial symptoms are those of acute intestinal obstruction, never- theless these symptoms improve after surgical approach is timely performed. Based on this outcome, it is concluded that a favorable out- come to this pathology depends on its early diagnosis, since an early diagnosis decreas- es morbidity and mortality chances.
INTRODUCCIÓN
La peritonitis meconial es una reacción infla- matoria química no infecciosa, secundaria a perforación intestinal en el periodo fetal (1), que se presenta de varias formas, entre ellas el quiste o psedoquiste meconial (2), cuya complicación más común es la obstrucción in- testinal, una urgencia quirúrgica conocida por desestabilizar rápidamente al paciente, ya que presenta síntomas como emesis, intolerancia a la vía oral y deshidratación grave, por lo que requiere de un abordaje rápido y especializa- do, en especial en este grupo etario (3).
En este caso se necesitaron múltiples estu- dios, y un diagnóstico temprano, el cual permitió prever las posibles complicaciones, además de un análisis del estado clínico de la pacien- te para elegir cuándo operarla, sus estudios pre-quirúrgicos, su abordaje quirúrgico y las conductas postoperatorias que evitaron la apa- rición de patologías como el íleo paralítico.
CASO CLÍNICO
Paciente femenina de 19 días de vida proce- dente y natural de Manizales, Colombia, que llegó remitida por su pediatra, con diagnósti- co prenatal por ecografía de masa abdominal con asa intestinal fija compatible con probable peritonitis meconial. Dentro de los antece- dentes de importancia la paciente presentaba una fractura del fémur izquierdo, secundaria a trauma perinatal de extracción podálica por cesárea; el embarazo no tuvo ninguna com- plicación y en el mismo no hubo consumo de medicamentos a excepción de ácido fólico durante el primer trimestre. En la valoración por consulta externa la niña se encontraba asintomática, razón por la cual su caso fue llevado a junta quirúrgica de la Fundación Santa Fe de Bogotá, donde se decidió programarla para cirugía de resección de la masa.
A los 24 días de edad, la madre la llevó al servicio de urgencias, ya que tuvo varios episodios eméticos y distensión abdominal. Al examen físico se encontró en regular estado general, activa, con arnés de inmovilización de fémur izquierdo (fractura por parto distósico). La paciente presentó abdomen distendido, doloroso a la palpación, con masa en hemiab- domen superior de 5 x 5 cm aproximadamen- te, delimitada, firme, no móvil; se solicitó una nueva ultrasonografía abdominal en la que se confirmó el hallazgo, además se evidenció que no hubo aumento en el tamaño de la masa, siendo aún de 42 mm x 41 mm. Por último, una radiografía de abdomen mostró masa cal-
cificada con signos de posible obstrucción in- testinal parcial (ver Figura 1).
Por su presentación clínica aguda, se de- cidió llevar a cirugía encontrando masa ab- dominal que ocupaba hemiabdomen derecho adherida a peritoneo parietal de aproximada- mente 7 x 7 cm, tabicada con dos cavidades; la porción más grande consistía en una masa sólida de contenido aparentemente meconial, mientras que la pequeña era quística, con membranas fibrinosas no fétidas (ver Figura 2a, 2b y 2c); asimismo, se observaron varias adherencias en asas intestinales yeyunoilea- les (ver Figura 2d) y una perforación intestinal anti-mesentérica, a 10 cm de la válvula ileoce- cal, de 0.3 cm de diámetro aproximadamente, así como un divertículo de Meckel de base amplia, de 0.5 cm de altura, a 20 cm de la válvula ileocecal (ver Figura 2e).

Fig 1. Radiografía de abdomen simple. Masa calci cada con signos de posible obstrucción intestinal parcial de 42 mm x 41 mm de diámetro.
Fuente: Documento obtenido durante la realización del estudio.
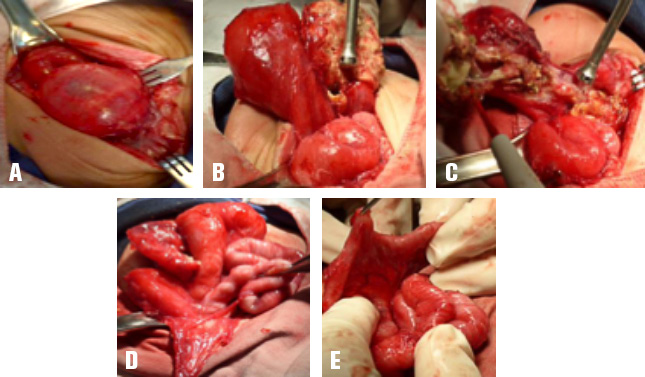
Fig 2A 2B 2C. Masa de 7 x 7 cm tabicada con dos cavidades: la primera grande y sólida con contenido meconial; la segunda, quística, con membranas brinosas no fétidas.
Fig 2D. Adherencias Yeyunoileales
Fig 2E. Perforación intestinal anti-mesentérica a 10 cm de la válvula ileocecal.
Con estos hallazgos se realizó resección completa de la masa, liberación de las adhe- rencias intestinales y rafia de la perforación intestinal en sentido transverso en un plano; por el tamaño del divertículo de Meckel se prefirió no resecarlo. Posteriormente, se to- maron muestras para patología y se trasladó la paciente a la unidad de cuidados intensi- vos pediátricos, en donde inició nutrición pa- renteral.
En la radiografía abdominal de control se encontró disminución en la cantidad de gas en la cámara gástrica, así como calcificacio- nes heterogéneas residuales en hemiabdo- men derecho (ver Figura 3). En los resultados de patología se identificaron una “perforación ileal con calcificación distrófica, unas adheren-
cias de tejido fibroso ricamente vascularizado que se encontraba crónicamente inflamado, un quiste peritoneal asociado a inflamación mixta y fibrosis, y peritonitis meconial organi- zada”, descartando de esta forma la presencia de una duplicación intestinal
En el postoperatorio la paciente presentó un ileo de cuatro días de evolución, algo de esperarse por la intervención quirúrgica y la patología adyacente. En el quinto día toleró con éxito la vía oral y para el sexto, realizó su primera deposición de consistencia líqui- da, por lo cual se decidió retirarle la nutrición parenteral y seguir con vía oral. Ya que no se presentaron complicaciones en la recu- peración, fue dada de alta al séptimo día post- operatorio.
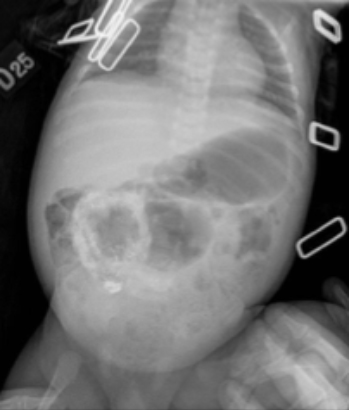
Fig 3. Radiografía de abdomen simple, 24 horas postoperatorio
Fuente: Documento obtenido durante la realización del estudio.
DISCUSIÓN
Este caso contó con la ventaja de un diag- nóstico temprano, el cual fue realizado in ute- ro a la semana 24 de gestación, a partir de la presencia de una masa calcificada, signo pa- tognomónico de peritonitis meconial (3). Lo anterior permitió un conocimiento previo del caso por parte del servicio de cirugía pediá- trica, por lo que fue posible elegir un plan de manejo adecuado; igualmente, se tuvo acce- so a imágenes tanto prenatales, como post- natales, con lo que pudo definirse el abordaje quirúrgico a emplear, así como la localización y el tamaño de la masa.
El aspecto positivo al examen físico fue la presencia de masa abdominal palpable, la cual es poco usual y se asocia más a sín- tomas como distensión abdominal, ascitis, calcificaciones intraabdominales, entre otros (4). Por otra parte, a pesar de haber programado la cirugía de resección de la masa por el hecho de que la paciente estuviera asinto- mática, la misma fue tratada como urgencia quirúrgica debido a la presentación de sínto- mas obstructivos agudos que evolucionaron en un corto tiempo. Sin embargo, la identifica- ción del cuadro obstructivo y su rápido ma- nejo médico-quirúrgico permitieron una ade- cuada evolución y un desarrollo favorable tanto de la intervención quirúrgica, como de su re- cuperación posoperatoria.
En cuanto el manejo quirúrgico, se encon- tró una masa pseudo quística compatible con quiste meconial, asociada a una perforación ileal de 0.3 cm de diámetro con bordes ne- cróticos, sin compromiso vascular subyacen- te, por lo que no fue necesario resecar parte del íleon, una complicación típica de esta pa- tología (5,6), lográndose un mejor pronóstico para la paciente. Es importante resaltar que en el transcurso de la enfermedad se debió te- ner en cuenta una fractura de fémur izquierdo agregada, la cual afortunadamente no generó ninguna complicación. Los hallazgos durante la cirugía sugerían una posible duplicación in- testinal, dado que las paredes de la masa se semejaban a las del intestino, pero esta opción fue descartada posteriormente por patología.
La peritonitis meconial puede ser secunda- ria a diversas etiologías, entre las que se inclu- yen, atresia intestinal, volvulus, brida congénita y síndrome del tapón de meconio (2,7), presen- tándose la última en la mayoría de los pacientes. Un porcentaje bajo de estos pacientes cursan con un cuadro de origen idiopático, también lla- mado peritonitis meconial simple (5), que, des- pués de descartar una duplicación intestinal, es la sospecha diagnóstica más posible para el caso aquí presentado. Esta entidad se ha vis- to asociada a la insuficiencia o hipoxia vascular transitoria del intestino fetal, así como a ciertas infecciones intestinales fetales, pero su rela- ción aún no está plenamente establecida (6,5).
Respecto al manejo médico-quirúrgico lle- vado a cabo en este caso, cabe resaltar las in- dicaciones de intervención quirúrgica, entre las que se encuentra la obstrucción intestinal o drenaje persistente de meconio a la cavidad abdominal, lo que puede producir distensión abdominal progresiva, dificultad respiratoria o sepsis (7). Por lo tanto, la indicación como urgencia quirúrgica en este caso fue ade- cuada; al inicio del cuadro clínico se tuvo en cuenta resecar la masa, no por presentar sín- tomas gastrointestinales, sino por el tamaño de la misma, considerándose indicado en el contexto de paciente asintomático, dado el riesgo de complicaciones.
En conclusión, la peritonitis meconial es una entidad poco descrita en la literatura que cuenta con un amplio espectro, no solo de etio-
logías, sino también de posibles complicacio- nes a corto plazo (1). Una de sus ventajas es su claro método de diagnóstico, el cual permite un rápido y adecuado manejo por parte del per- sonal médico (3). En este reporte se evidencia cómo las complicaciones pueden desarrollarse de forma aguda e imprevista; ahora bien, en el caso de esta paciente, dichas complicaciones tuvieron un desenlace favorable gracias a su ma- nejo oportuno, lo cual disminuyó de forma nota- ble la probabilidad de morbi-mortalidad.
CONFLICTOS DE INTERÉS
Los autores de este estudio declaran que en la redacción del mismo no hay conflicto de intereses personales (honorarios, beneficios personales), ni personales (dirigido hacia una unidad de servicio y/o investigación) en- tre los proveedores de medicamentos y ma- terial quirúrgico y el grupo de autores.
FINANCIACIÓN
Ninguna declarada por los autores.
Referencias
1.Lee YC, Chen CJ. Meconium pseudocyst: a classical and successfully treated case. J Formos Med Assoc. 2009;108(3):247-252. http://doi. org/bw85s2.
2.Tsai MH, Chu SM, Lien R, Huan HR, Luo CC. Clinical manifestations in infants with symp- tomatic meconium peritonitis. Pediatr Neonatol. 2009;50(2):59-64. http://doi.org/cvjpv2.
3.del Ciampo IR, Oliveira TQ, del Ciampo LA, Sawamura R, Torres LA, Augustin AE, et al. Early manifestations of cystic fibrosis in a premature patient with complex meconium ileus at birth. Rev Paul Pediatr. 2015;33(2):241-5. http://doi.org/f27fps.
4.Dirkes K, Crombleholme TM, Craigo SD, Latchaw LA, Jacir NN, Harris BH, et al. The natural history of meconium peritonitis diagnosed in utero. J Pediatr Surg. 1995;30(7):979-982. http://doi.org/dg28xd.
5.Uchida K, Koike Y, Matsushita K, Nagano Y, Hashimoto K, Otake K, et al. Meconium peritonitis: Prenatal diagnosis of a rare entity and postnatal management. Intractable Rare Dis Res. 2015;4(2):93-7. http://doi.org/bqm2.
6.Barthel ER, Speer AL, Levin DE, Naik-Mathu- ria BJ, Grikscheit TC. Giant cystic meconium peritonitis presenting in a neonate with classic ra- diographic eggshell calcifications and treated with an elective surgical approach: a case report. J Med Case Rep. 2012;6:229. http://doi.org/fzcxfb.
7.Lee G, Chandran S, Rajadurai VS. Calci- fied meconium pseudocyst: X-ray diagnosis of meconium peritonitis at birth. BMJ Case Rep. 2015;2015:bcr2015211052. http://doi.org/bqm3.
8.Ionescu S, Andrei B, Oancea M, Licsandru E, Ivanov M, Marcu V, et al. Postnatal Treat- ment in Antenatally Diagnosed Meconium Peri- tonitis. Chirurgia (Bucur). 2015;110(6):538-44.
Referencias
Lee YC, Chen CJ. Meconium pseudocyst: a classical and successfully treated case. J Formos Med Assoc. 2009;108(3):247-252. http://doi.org/bw85s2
Tsai MH, Chu SM, Lien R, Huan HR, Luo CC. Clinical manifestations in infants with symptomatic meconium peritonitis. Pediatr Neonatol. 2009;50(2):59-64. http://doi.org/cvjpv2
del Ciampo IR, Oliveira TQ, del Ciampo LA, Sawamura R, Torres LA, Augustin AE, et al. Early manifestations of cystic fibrosis in a premature patient with complex meconium ileus at birth. Rev Paul Pediatr. 2015;33(2):241-5. http://doi.org/f27fps
Dirkes K, Crombleholme TM, Craigo SD, Latchaw LA, Jacir NN, Harris BH, et al. The natural history of meconium peritonitis diagnosed in utero. J Pediatr Surg. 1995;30(7):979-982. http://doi.org/dg28xd
Uchida K, Koike Y, Matsushita K, Nagano Y, Hashimoto K, Otake K, et al. Meconium peritonitis: Prenatal diagnosis of a rare entity and postnatal management. Intractable Rare Dis Res. 2015;4(2):93-7. http://doi.org/bqm2
Barthel ER, Speer AL, Levin DE, Naik-Mathuria BJ, Grikscheit TC. Giant cystic meconium peritonitis presenting in a neonate with classic radiographic eggshell calcifications and treated with an elective surgical approach: a case report. J Med Case Rep. 2012;6:229. http://doi.org/fzcxfb
Lee G, Chandran S, Rajadurai VS. Calcified meconium pseudocyst: X-ray diagnosis of meconium peritonitis at birth. BMJ Case Rep. 2015;2015:bcr2015211052. http://doi.org/bqm3
Ionescu S, Andrei B, Oancea M, Licsandru E, Ivanov M, Marcu V, et al. Postnatal Treatment in Antenatally Diagnosed Meconium Peritonitis. Chirurgia (Bucur). 2015;110(6):538-44.
Cómo citar
APA
ACM
ACS
ABNT
Chicago
Harvard
IEEE
MLA
Turabian
Vancouver
Descargar cita
Visitas a la página del resumen del artículo
Descargas
Licencia
Derechos de autor 2016 Case reports

Esta obra está bajo una licencia internacional Creative Commons Atribución-NoComercial-SinDerivadas 4.0.
Los autores al someter sus manuscritos conservarán sus derechos de autor. La revista tiene el derecho del uso, reproducción, transmisión, distribución y publicación en cualquier forma o medio.
El Formulario de Divulgación Uniforme para posibles Conflictos de Interés y los oficios de cesión de derechos y de responsabilidad deben ser entregados junto con el original.
Aquellos autores/as que tengan publicaciones con esta revista, aceptan los términos siguientes:
Los autores/as conservarán sus derechos de autor y garantizarán a la revista el derecho de primera publicación de su obra, el cual estará simultáneamente sujeto a la Licencia de reconocimiento de Creative Commons 4.0 que permite a terceros compartir la obra siempre que se indique su autor y su primera publicación en esta revista.
Los autores/as podrán adoptar otros acuerdos de licencia no exclusiva de distribución de la versión de la obra publicada (p. ej.: depositarla en un archivo telemático institucional o publicarla en un volumen monográfico) siempre que se indique la publicación inicial en esta revista.
Se permite y recomienda a los autores/as difundir su obra a través de Internet (p. ej.: en archivos telemáticos institucionales o en su página web) antes y durante el proceso de envío, lo cual puede producir intercambios interesantes y aumentar las citas de la obra publicada. (Véase El efecto del acceso abierto).























