



Published
Diseño y validación del material educativo incluido en una estrategia de educación en salud dirigida a personas con enfermedades cardiovasculares e impartida vía WhatsApp
Design and validation of educational material included in a health education strategy aimed at individuals with cardiovascular diseases implemented via WhatsApp
DOI:
https://doi.org/10.15446/revfacmed.v72n3.111417Keywords:
Educación en salud, Rehabilitación cardiaca, Redes sociales, Fisioterapia (es)Health Education, Cardiac Rehabilitation, Social Networking, Therapeutics (en)
Introducción. Las enfermedades cardiovasculares (ECV) son la principal causa de muerte en el mundo. Se ha comprobado que la rehabilitación cardiaca ofrece beneficios a los pacientes con ECV; sin embargo, pocos perduran en el tiempo debido a la pobre adherencia, lo cual podría estar influenciado por la falta de programas de educación estructurados.
Objetivos. Diseñar y validar el material educativo incluido en una estrategia de educación en salud impartida vía WhatsApp dirigida a personas con ECV usuarios de un programa de rehabilitación cardiaca (PRC).
Materiales y métodos. Estudio de métodos mixtos basado en el proceso de investigación-creación y desarrollado en dos etapas: etapa de diseño y elaboración de la estrategia educativa y etapa de validación del material educativo, la cual incluyó una validación técnica (participación de 8 profesionales de la salud) y una validación por público objetivo (participación de 6 pacientes con ECV usuarios de un PCR-fase 2). Se siguieron los lineamientos de la Organización Panamericana de la Salud para la elaboración y validación de material educativo en salud.
Resultados. La versión 1 de la estrategia tenía 26 piezas educativas (17 imágenes, 5 audios y 4 videos), de las cuales 96.3% se calificaron en “dejar como está”. Teniendo en cuenta las sugerencias en contenido y forma hechas por los expertos, en la versión 2 se incluyeron 31 piezas educativas (22 imágenes, 5 audios y 4 videos). Posterior a la validación de público objetivo, la versión final del material consistió de 30 ítems (21 imágenes, 4 audios y 5 videos).
Conclusión. En el presente estudio fue posible diseñar y validar material educativo dirigido a usuarios de un PRC que, al estar centrado en el paciente y ser de fácil difusión vía una red social ampliamente utilizada, se convierte en una herramienta que puede ayudar a mejorar la adherencia a estos programas.
Este ensayo clínico fue registrado en el Australian New Zealand Clinical Trials Registry bajo el código ACTRN12622001446752.
Introduction: Cardiovascular disease (CVD) is the leading cause of death worldwide. Cardiac rehabilitation programs (CRP) have demonstrated advantages for patients with CVD; however, few maintain their participation over time due to poor adherence, which could be impacted by the lack of structured education programs.
Objectives: To design and validate educational material included in a health education strategy implemented via WhatsApp aimed at individuals with CVD who participate in a CRP.
Materials and methods: Mixed methods study based on the research-creation process and developed in two stages: design and elaboration stage of the educational strategy and validation stage of the educational material, which included a technical validation (participation of 8 health professionals) and a target audience validation (participation of 6 patients with CVD users of a phase 2-CRP). This study followed the guidelines of the Pan American Health Organization for the elaboration and validation of educational material in health care.
Results: The first version of the strategy included 26 educational pieces (17 images, 5 audios, and 4 videos), and 96.3% of them were rated as “use as is”. Considering the content and form suggestions made by the experts, the second version included 31 educational pieces (22 images, 5 audios, and 4 videos). Following the validation of the target audience, the final version of the material consisted of 30 pieces (21 images, 4 audios, and 5 videos).
Conclusion: The present study allowed us to design and validate educational material targeted at CRP users which, through its patient-centered nature and easy dissemination via a widely used social network, becomes a tool that can help to improve adherence to these programs.
This clinical trial was registered in the Australian New Zealand Clinical Trials Registry under code ACTRN12622001446752.
Original research
Design and validation of educational material included in a health education strategy aimed at individuals with cardiovascular diseases implemented via WhatsApp
Diseño y validación del material educativo incluido en una estrategia de educación en salud dirigida a personas con enfermedades cardiovasculares e impartida vía WhatsApp
Adriana Jacome-Hortua1![]() Adriana Pinto-Prada1
Adriana Pinto-Prada1![]() Natalia Quintero-Tibaduiza1
Natalia Quintero-Tibaduiza1![]() Paula Alejandra Luna1
Paula Alejandra Luna1![]() Tania Lucia Olaya-Grass1
Tania Lucia Olaya-Grass1![]() Liz Patricia Daza-Acosta1
Liz Patricia Daza-Acosta1![]() Katherine Anaya-Ocampo1
Katherine Anaya-Ocampo1![]() Zully Rocío Rincón-Rueda1
Zully Rocío Rincón-Rueda1![]()
1 Universidad de Santander - Faculty of Medical and Health Sciences - Bucaramanga - Colombia.Open access
Received: 04/10/2023
Accepted: 17/07/2024
Corresponding author: Adriana Jacome-Hortua. Facultad de Ciencias Médicas y de la Salud, Universidad de Santander. Bucaramanga. Colombia. E-mail: ad.jacome@mail.udes.edu.co.
Keywords: Health Education; Cardiac Rehabilitation: Social Networking; Therapeutics (MeSH).
Palabras clave: Educación en salud; Rehabilitación cardiaca; Redes sociales; Fisioterapia (DeCS).
How to cite: Jacome-Hortua A, Pinto-Prada A, Quintero-Tibaduiza N, Luna PA, Olaya-Grass TN, Daza-Acosta LP, et al. Design and validation of educational material included in a health education strategy aimed at individuals with cardiovascular diseases implemented via WhatsApp. Rev. Fac. Med. 2024;72(3):e111417. English. doi: https://doi.org/10.15446/revfacmed.v72n3.111417.
Cómo citar: Jacome-Hortua A, Pinto-Prada A, Quintero-Tibaduiza N, Luna PA, Olaya-Grass TN, Daza-Acosta LP, et al. [Diseño y validación del material educativo incluido en una estrategia de educación en salud dirigida a personas con enfermedades cardiovasculares e impartida vía WhatsApp]. Rev. Fac. Med. 2024;72(3):e111417. English. doi: https://doi.org/10.15446/revfacmed.v72n3.111417.
Copyright: Copyright: ©2024 Universidad Nacional de Colombia. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, as long as the original author and source are credited.
Abstract
Introduction: Cardiovascular disease (CVD) is the leading cause of death worldwide. Cardiac rehabilitation programs (CRP) have demonstrated advantages for patients with CVD; however, few maintain their participation over time due to poor adherence, which could be impacted by the lack of structured education programs.
Objectives: To design and validate educational material included in a health education strategy implemented via WhatsApp aimed at individuals with CVD who participate in a CRP.
Materials and methods: Mixed methods study based on the research-creation process and developed in two stages: design and elaboration stage of the educational strategy and validation stage of the educational material, which included a technical validation (participation of 8 health professionals) and a target audience validation (participation of 6 patients with CVD users of a phase 2-CRP). This study followed the guidelines of the Pan American Health Organization for the elaboration and validation of educational material in health care.
Results: The first version of the strategy included 26 educational pieces (17 images, 5 audios, and 4 videos), and 96.3% of them were rated as “use as is”. Considering the content and form suggestions made by the experts, the second version included 31 educational pieces (22 images, 5 audios, and 4 videos). Following the validation of the target audience, the final version of the material consisted of 30 pieces (21 images, 4 audios, and 5 videos).
Conclusion: The present study allowed us to design and validate educational material targeted at CRP users which, through its patient-centered nature and easy dissemination via a widely used social network, becomes a tool that can help to improve adherence to these programs.
This clinical trial was registered in the Australian New Zealand Clinical Trials Registry under code ACTRN12622001446752.
Resumen
Introducción. Las enfermedades cardiovasculares (ECV) son la principal causa de muerte en el mundo. Se ha comprobado que la rehabilitación cardiaca ofrece beneficios a los pacientes con ECV; sin embargo, pocos perduran en el tiempo debido a la pobre adherencia, lo cual podría estar influenciado por la falta de programas de educación estructurados.
Objetivos. Diseñar y validar el material educativo incluido en una estrategia de educación en salud impartida vía WhatsApp dirigida a personas con ECV usuarios de un programa de rehabilitación cardiaca (PRC).
Materiales y métodos. Estudio de métodos mixtos basado en el proceso de investigación-creación y desarrollado en dos etapas: etapa de diseño y elaboración de la estrategia educativa y etapa de validación del material educativo, la cual incluyó una validación técnica (participación de 8 profesionales de la salud) y una validación por público objetivo (participación de 6 pacientes con ECV usuarios de un PCR-fase 2). Se siguieron los lineamientos de la Organización Panamericana de la Salud para la elaboración y validación de material educativo en salud.
Resultados. La versión 1 de la estrategia tenía 26 piezas educativas (17 imágenes, 5 audios y 4 videos), de las cuales 96.3% se calificaron en “dejar como está”. Teniendo en cuenta las sugerencias en contenido y forma hechas por los expertos, en la versión 2 se incluyeron 31 piezas educativas (22 imágenes, 5 audios y 4 videos). Posterior a la validación de público objetivo, la versión final del material consistió de 30 ítems (21 imágenes, 4 audios y 5 videos).
Conclusión. En el presente estudio fue posible diseñar y validar material educativo dirigido a usuarios de un PRC que, al estar centrado en el paciente y ser de fácil difusión vía una red social ampliamente utilizada, se convierte en una herramienta que puede ayudar a mejorar la adherencia a estos programas.
Este ensayo clínico fue registrado en el Australian New Zealand Clinical Trials Registry bajo el código ACTRN12622001446752.
Introduction
Cardiovascular disease (CVD) is the leading cause of mortality and morbidity worldwide.1 It has been reported that modifiable CVD risk factors, such as hypertension (HT), dyslipidemia, diabetes mellitus (DM), smoking, psychological stress, sedentary lifestyle, alcohol consumption, high waist/hip ratio and unhealthy diet, increase the risk of developing heart disease, the main outcome being acute myocardial infarction.2
One of the support strategies for the treatment of individuals with CVD is cardiac rehabilitation programs (CRP), which involve activities that allow these individuals to improve their physical3,4 and mental status,5 as well as to promote their social independence.6 This is achieved by having personalized physical activity and health education as pillars, resulting in a positive impact on their quality of life,7-9 their reintegration into the workplace,10,11 and their functional capacity.12,13 However, studies have reported that these benefits are not sustained in the long term by many patients who participate in CRPs,14-16 possibly due to poor adherence to these programs, lack of follow-up, the presence of comorbidities, and the existence of structured health education processes.17,18
Recent scientific literature does not clearly describe the health education processes or interventions that should be used in this population, so each CRP must establish a route to follow for its proper implementation.19-21 Moreover, some authors, such as Molina et al.,22 point out that the importance of health education in the prevention of cardiovascular events is still not recognized, suggesting that the development and implementation of health education actions could increase the effectiveness of treatments, thus reducing the risk of comorbidities and complications. It has also been described that the use of health education programs or interventions improves health-related quality of life in patients with CVD and may even lead to a reduction in the scores obtained in scales predicting cardiovascular events due to their effect on risk factors.19,21
It has been reported that the use of information and communication technologies for the development and implementation of health education interventions is effective, particularly in secondary prevention activities, since, besides facilitating clear and timely access to health information by patients, these technologies make it possible to guide and supervise users at any time and from any place.23-25
A variety of social networks are available, but WhatsApp26 is popular and convenient for medical education as it allows smartphone users to send text messages, share audiovisual content, create groups, and have multiple users participate and monitor the conversation. It is also easily accessible (even for people with relatively low levels of literacy), can be used at any time, and does not involve additional data plan costs.23,25,27
In view of the above, the objectives of the present study were to design and validate the educational material included in a health education strategy implemented via WhatsApp aimed at individuals with CVD and users of a CRP.
Materials and methods
Study type
Mixed-methods sequential explanatory design study28,29 based on the research-creation process.30,31
Procedure
This study was carried out in 2 stages: design and elaboration stage of the educational strategy to be implemented via WhatsApp, which was developed from February to December 2020 in 5 phases (Figure 1), and validation stage carried out from July to November 2021. The health education material was developed and validated taking into account the guidelines of the Pan American Health Organization (PAHO).32
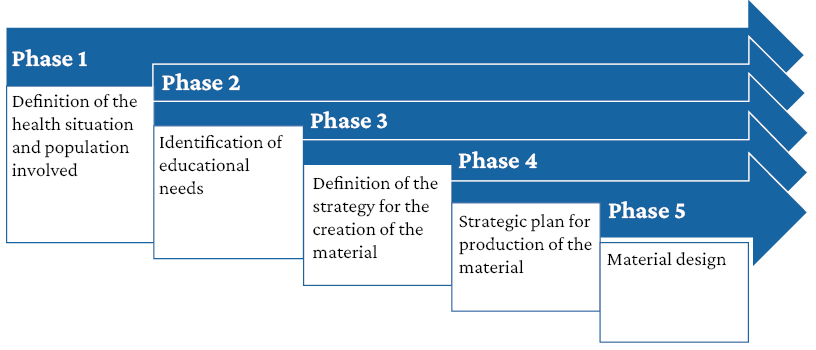
Figure 1. Phases of the design and validation process.
Source: Elaboration based on Hernández-Sánchez.33
Stage 1. Design and development of the educational strategy
The phases of this stage are described below:
Phase 1. Delimitation of the problem: To define and identify the population involved in this study, the scientific literature and health indicators were reviewed, a questionnaire was designed for the researchers, and a problem tree was created.
Phase 2. Identification of educational needs: International guidelines on cardiac rehabilitation education were reviewed to select the topics to be addressed, and the pedagogical competence of the educational strategy was formulated.
Phase 3. Definition of the educational strategy content and the pieces that would make up the strategy: The duration and frequency of delivery of the educational strategy was established.
Phase 4. Search for applications to create educational pieces: The general characteristics of the educational material were decided upon.
Phase 5: Production of the educational material: The first version of the educational material was produced.
Stage 2. Validation of the educational material
This stage was divided into two phases that were developed using a mixed approach:34
Phase 1. Technical validation: It was carried out by 8 health professional experts with more than 2 years of experience in health education processes and CRP, who quantitatively and qualitatively evaluated the first version of the pieces (images, audios, and videos) included in the educational material of the health education strategy developed in stage 1.
A form prepared in accordance with the model proposed by PAHO was filled out for quantitative evaluation.32 The form and the contents of each image, audio, and video piece included in the educational strategy were evaluated on a 1-5 Likert scale, with 1 being the lowest and 5 the highest score. In addition, several cut-off points were set based on the type of resource to define the behavior to be followed with each resource (Table 1). According to the type of resource and the number of criteria established, the highest score that each piece could obtain depending on its typology was: audio: 45 points, image: 40 points, and video: 55 points.
The qualitative evaluation was carried out through a focus group with experts (video call) and face-to-face semi-structured interviews with users, during which they were asked about their perception of the material. From these results, the adjustments to be made to the pieces were determined in order to produce the second version of the educational material.
Table 1. Criteria for quantitative evaluation of educational material and established cut-off points.
|
|
Video |
Audio |
Image |
|
Criteria |
- Image and sound are synchronized - There are elements that make it appealing - There are elements that summarize the content or message - A specific topic is presented in a comprehensive manner - The messages are easily understood - Images are clearly visible - Sound elements are heard properly - Messages are presented objectively - There are elements that encourage participation - There is no information overload - Duration is not too long |
- Sound level is appropriate - Language is clear - Messages are mutually strengthened - There are elements that make it appealing, e.g., music and a pleasant pitch - A single topic is addressed - Secondary aspects (music, sound effects, etc.) do not divert attention from the main message - Messages are presented objectively - There are elements that encourage audience participation - Community members can access it easily |
- A specific topic is presented - The topic is easily understood - Colors and images contribute to emphasizing the topic - The message is objective - The message does not allow for ambiguous interpretations - The material does not contain unnecessary elements - The size of the elements favors good visualization - The image encourages discussion of the topic it addresses - It can be easily transported |
|
Cut-off points |
Use as is (48-55 points) Improvements required (28-47 points) Rejected (less than 28 points). |
Use as is (40-45 points) Improvements required (21-39 points) Rejected (less than 21 points) |
Use as is (35-40 points) Improvements required (16-34 points) Rejected (less than 16 points) |
Phase 2. Target audience validation: It was carried out with the participation of 6 patients with CVD, users of a phase 2 CRP of a health care institution in Bucaramanga, who were selected by convenience sampling taking into account the following inclusion criteria: having a smartphone and knowing how to use WhatsApp, Google Forms, and Zoom. The selection process was initiated by the CRP administrative assistant, who explained to the patients the objective of the study and the specific stage in which they were going to participate. Once they agreed to participate, she shared their contact information (cell phone and WhatsApp number) with the researchers to validate the inclusion criteria by means of test messages.
The patients evaluated the second version of the educational material as follows: during the quantitative phase, they filled out the same form used for the technical validation; during the qualitative phase, each person answered the following question during a semi-structured interview: “Do you see any areas in the resource that should be improved?” The results of this phase made it possible to create the final version of the educational material.
Data analysis
Data regarding the quantitative evaluations of both versions of the educational material were described using means.35,36 As for the qualitative evaluations, the focus group audios and semi-structured interviews were transcribed and coded for descriptive analysis, grouping the suggestions made for each image, audio, and video piece evaluated, thus defining the improvements to be made to each one of them, independently of whether the result of the quantitative evaluation was “use as is”.
Ethical considerations
The study followed the ethical principles for biomedical research involving human subjects established in the Declaration of Helsinki37 and the scientific, technical, and administrative standards for health research of Resolution 8430 of 1993 issued by the Colombian Ministry of Health.38 It was also approved by the ethics committee of the Universidad de Santander as per minutes No. FI74-21 of June 8, 2021, and all participants signed an informed consent. Data were protected in accordance with Law 1581 of 2012.39
Results
Design and development of the educational strategy
In order to design the educational strategy, and based on the established problem, the competence to be developed was defined as “strengthening knowledge of cardiovascular risk factors, pharmacological treatment, nutritional recommendations, and physical activity among individuals attending a phase 2 CRP, to promote the adoption of healthy lifestyles and improve adherence to rehabilitation”.
To plan the structure of the educational strategy, the 4 main CVD risk factors (HT, DM, smoking, and dyslipidemia) were selected,12,40 addressing one per week, for a total of 4 weeks. The strategy was designed so that each working day of the week would address a different aspect of the risk factor under discussion: day 1: pathophysiology of the disease or condition (for smokers, composition and harmful effects were also addressed); day 2: pharmacological treatment (for smokers, psychotherapy, and other interventions for smoking cessation were mentioned); day 3: nutritional recommendations; day 4: physical activity recommendations; day 5: motivational element aimed at making the patient end the week with a message that inspires, encourages, and motivates them to modify their lifestyles (Table 2).
Table 2. Validation process by experts and target audience of the strategy and educational material.
|
Week |
Day |
1st version |
Score |
Recommendation |
Comments from experts |
2nd version |
Score |
Recommendation |
Comments from target audience |
Final version |
|---|---|---|---|---|---|---|---|---|---|---|
|
Week 1: Arterial Hypertension |
Monday Pathophysiology |
Img01 |
38 |
Use as is |
Explain that hypertension is a chronic disease that can be controlled, but not cured. Include normal blood pressure figures and warning values. |
Img01 |
37 |
Use as is |
Prevention should be adapted to all age groups. The language should also be more inclusive and differentiate the range of normal blood pressure based on age, gender, or race. |
Img01 |
|
Tuesday Pharmacology |
Img02 |
38 |
Use as is |
Change side effects to unwanted effects. |
Img02 |
35 |
Use as is |
Change the title of “undesirable aspects” to “side effects that may occur when taking HT medication,” and add: if the symptoms are severe, consult your physician. |
Img02 |
|
|
Wednesday Nutritional recommendations |
Img03 |
37 |
Use as is |
Emphasize the importance of consuming sodium. It is suggested to divide the image in two. |
Img03 |
40 |
Use as is |
Use a symbol that shows positive and negative aspects and adjust the food images accordingly. |
Img03 |
|
|
Img04 |
40 |
Use as is |
No modifications |
Img04 |
||||||
|
Aud01 |
44 |
Use as is |
Emphasize the importance of consuming sodium. |
Aud01 |
45 |
Use as is |
No modifications |
Aud01 |
||
|
Thursday Physical activity recommendations |
Vid01 |
53 |
Use as is |
Replace terms with images, e.g., free weight. |
Vid01 |
53 |
Use as is |
No modifications |
Vid01 |
|
|
Friday Motivational |
Img04 |
39 |
Use as is |
Specify the place where the patient can go to when they are experiencing grief, so that they know there is an expert who can provide them with more personalized care. |
Img05 |
38 |
Use as is |
Adjust the color scale. |
Img05 |
|
|
Challenge #1 was created at the suggestion of experts. |
Img06 |
35 |
Use as is |
No modifications |
Img06 |
|||||
|
Week 2: Diabetes mellitus |
Monday Pathophysiology |
Img05 |
39 |
Use as is |
The definition of type II diabetes should include “is caused by insulin resistance and inadequate insulin production” as a key part of the definition. |
Img07 |
38 |
Use as is |
Add the name of the pancreas over the image to better understand it. |
Img07 |
|
Tuesday Pharmacology |
Img06 |
37 |
Use as is |
Another image should be included with the treatment goals indicating the values to be achieved. |
Img08 |
38 |
Use as is |
Modify the glycosylated hemoglobin value from 6-7%. Add fasting glycemia values. List medications in a single line. |
Img08 |
|
|
Wednesday Nutritional recommendations |
Img07 |
38 |
Use as is |
State “all types of sugar, including honey or sugarcane, should be eliminated or reduced”. |
Img09 |
40 |
Use as is |
No modifications |
Img09 |
|
|
Aud02 |
43 |
Use as is |
The audio should clearly stress the importance of not self-medicating, given that even some herbal infusions can cause serious side effects on your health. |
Aud02 |
43 |
Use as is |
No modifications |
Aud02 |
||
|
Thursday Physical activity recommendations |
Vid02 |
53 |
Use as is |
Show images of strength training. |
Vid02 |
53 |
Use as is |
No modifications |
Vid02 |
|
|
Friday Motivational |
Img08 |
40 |
Use as is |
Include information on support networks. |
Img10 |
40 |
Use as is |
No modifications |
Img10 |
|
|
|
Challenge #2 was created at the suggestion of experts. |
Img11 |
35 |
Use as is |
No modifications |
Img11 |
||||
|
Week 3: Smoking |
Monday Pathophysiology |
Img9 |
38 |
Use as is |
Fix the size and font to improve its appearance. Not only include information on the harm caused by the common cigarette, but also on the harm caused by electric cigarettes and other similar devices. |
Img12 |
40 |
Use as is |
No modifications since explaining what an electronic cigarette is is not the purpose of the resource. |
Img12 |
|
Tuesday Pharmacology |
Img10 |
38 |
Use as is |
It is important to mention the psychotherapeutic dimension, which is a fundamental basis for smoking cessation. |
Img13 |
38 |
Use as is |
Change title to unwanted effects. |
Img13 |
|
|
Wednesday Nutritional recommendations |
Img11:Plato saludable |
39 |
Use as is |
Compare grams with centimeters or teaspoons to make it easier to understand. |
Img14 |
40 |
Use as is |
No modifications |
Img14 |
|
|
Aud03 |
44 |
Use as is |
Improve voice pitch. |
Aud03 |
45 |
Use as is |
No modifications |
Aud03 |
||
|
Img12: Leer etiquetas |
37 |
Use as is |
Include the nutritional table |
Img15 |
40 |
Use as is |
Make a video explaining the image. |
Vid03 |
||
|
Aud04 |
44 |
Use as is |
Name other foods that have the same effects and are cheaper. |
Aud04 |
45 |
Use as is |
Make a video explaining the image. |
|
||
|
Thursday Physical activity recommendations |
Vid03 |
54 |
Use as is |
Appropriate |
Vid03 |
55 |
Use as is |
No modifications |
Vid04 |
|
|
Friday Motivational |
Img13 |
38 |
Use as is |
Appropriate |
Img16 |
35 |
Use as is |
No modifications |
Img15 |
|
|
|
Challenge #3 was created at the suggestion of experts. |
Img17 |
35 |
Use as is |
No modifications |
Img16 |
||||
|
Week 4: Dyslipidemia |
Monday Pathophysiology |
Img14 |
39 |
Use as is |
|
Img18 |
38 |
Use as is |
No modifications |
Img17 |
|
Tuesday Pharmacology |
Img15 |
34 |
Improvements needed |
The image has too much content. |
Img19 |
38 |
Use as is |
Modify the size, type and font color of the undesired effect for each group of drugs. |
Img18 |
|
|
Wednesday Nutritional recommendations |
Img16 |
36 |
Use as is |
Summarize the text and change the font color. |
Img20 |
40 |
Use as is |
Redesign the resource, listing the four groups in a table, reducing the font, and putting the most relevant information in bullets. |
Img19 |
|
|
Aud05 |
44 |
Use as is |
No modifications |
Aud05 |
45 |
Use as is |
No modifications |
Aud04 |
||
|
Thursday Physical activity recommendations |
Vid04 |
52 |
Use as is |
No modifications |
Vid04 |
55 |
Use as is |
No modifications |
Vid05 |
|
|
Friday Motivational |
Img17 |
38 |
Use as is |
No modifications |
Img21 |
36 |
Use as is |
No modifications |
Img20 |
|
|
|
Challenge #4 was created at the suggestion of experts. |
Img22 |
35 |
Use as is |
No modifications |
Img21 |
||||
|
Total resources |
1st version: 26 pieces: 17 images, 5 audios, and 4 videos 2nd version: 31 pieces: 22 images, 5 audios, and 4 videos Final version: 30 pieces: 21 images, 4 audios, and 5 videos |
|||||||||
Img: image; HT: hypertension; Aud: audio; Vid: video.
The design and elaboration of the educational material was carried out using free versions of graphic design and audiovisual material creation applications such as Canva and Powtoon. The first version of the educational material comprised 26 educational pieces: 17 images, 5 audios, and 4 videos.
Validation of educational material
Technical validation
The group of experts that validated the first version of the strategy included 3 physical therapists, 1 family physician, 1 nutritionist, 1 psychologist, 1 nurse, and 1 public health professional. Among these professionals, 7 had a master’s degree, 5 were involved in teaching, 4 conducted research, 3 worked in health care, and 3 had more than 5 years of experience in CRP.
Table 2 presents the results of the quantitative evaluation of the technical validation. According to the established cut-off points and the average score obtained for each educational resource, it was determined that the behavior to be followed was “use as is” for all resources except for image 16, which addressed information on the pharmacological treatment of dyslipidemia and was considered to “need improvements”.
The resources were modified considering the suggestions made by the experts of the focus group, all of which were related to improving the clarity of the texts (elimination of ambiguities) to promote the discussion of the topics addressed. Therefore, the design and font were modified and information was added to improve the quality of the resources. In addition, a weekly challenge to be sent on Fridays was included, thus obtaining the second version of the educational strategy, which consisted of 31 educational pieces: 22 images, 5 audios, and 4 videos (Table 2).
Target audience validation
The mean age of the 6 patients with CVD who participated in this phase was 57±7.8 years and coronary artery disease was the most common CVD (n=3). The other diagnoses were atrial fibrillation, cardiogenic syncope, and valvular heart disease. Regarding risk factors, the most prevalent was HT (n=5), followed by dyslipidemia (n=3), and DM (n=2). Based on the mean score obtained in the quantitative assessment, the recommendation for all the resources was “use as is”. Furthermore, based on the suggestions made by these patients in the semi-structured interviews, each resource was modified to improve its quality (Table 3) and facilitate its understanding by potential patients, thus obtaining the final version of the strategy, which is made up of 30 educational pieces (21 images, 4 audios and 5 videos) and can be accessed at https://repositorio.udes.edu.co/handle/001/9929.
Table 3. Codes emerging from the qualitative analysis.
|
Category |
Emerging codes |
|
|
Experts |
Target audience |
|
|
Positive aspects of the material |
E7-L86: the topic is very well documented on promotion and prevention. |
P4-L205-207: the motivational resources are clear and appealing. I think the sentences are good. |
|
E8-L88: well-structured material in both form and content. |
P4-L212: resources on smoking are clear and user-friendly. |
|
|
E1-L89: material that is easy on the eye. |
P5-L242: training videos are clear and interesting. |
|
|
E3-L90: relevant strategy that is relevant, appropriate, and pertinent to the population. |
P6-L289,290: resources are good and useful for raising awareness of disease prevention, even at an early age. |
|
|
Aspects to be improved |
E4-L16: summarize stages of grief. E4-L85: summarize text. |
P2-L62: explain the medical terms, e.g. hypotension |
|
E2-L52: adjust the font size and style to improve its appearance. |
P3-L127,128: reduce the amount of nutritional resource information and improve image agreement. |
|
|
E4-L46: matching audio and video. Screen images on strength training. |
P1-L16-18: use more eye-catching colors in motivational resources. |
|
|
E4-L48: the motivational component must be more dynamic. |
P1-L11,12: replace some image resources on nutrition with explanatory videos. |
|
|
E2-L81: condense the text and change the font color. |
||
|
Suggestions |
E1-L65: it should be made clear in the audio that these are general recommendations, but please contact the nutritionist for personalized treatment. |
E3-L143: include normal blood pressure and glycemia figures. |
|
E2-L75: clearly identify the professional to whom the patient can turn to in each strategy. |
||
E: expert; P: patient; L: line.
Discussion
This research aimed to create and validate educational material included in a health education strategy directed at CVD patients participating in a phase 2 CRP and designed to be implemented via WhatsApp.
Studies have reported that developing and validating the educational material used in health education interventions aimed at patients could have a positive impact on their level of knowledge of both the disease and its treatment.19,41-44 For example, Arantes et al.,19 in a study conducted in 56 patients from Ribeirão Preto (Sao Paulo, Brazil) with coronary artery disease undergoing percutaneous coronary intervention, compared the results of the implementation of an educational program vs. usual care in terms of health-related quality of life (assessed with the SF-36 questionnaire), finding that patients who participated in the educational program showed a statistically significant improvement in the emotional role domain after one year of follow-up (p=0.05).
It is noteworthy that our research proposed the design of an educational strategy with a multidisciplinary approach. This is similar to the educational booklet for patients with head and neck cancer undergoing radiotherapy proposed by da Cruz et al.,41 who validated the design of the booklet by working with various professionals. For example, they resorted to experts in the field and professionals in literature and advertising, who evaluated the objectives, structure, presentation and relevance, resulting in a comprehensive and multidisciplinary document.
Likewise, Moura et al.44 created a booklet for the prevention of metabolic syndrome in adolescents with the participation of 6 health professionals and 7 professionals with experience in design. Their objective was to have specialized knowledge of the topics addressed in the educational material, factors that supported the inclusion in our study of a multiprofessional team for the elaboration and validation of the educational strategy.
Regarding the relevance of validating educational material, Brütting et al.45 evaluated the quality, readability, and comprehensibility of educational brochures for melanoma patients, demonstrating that there is an important need to create visual educational materials that emphasize self-care and that are easy to understand for the target population, in addition to being of good quality. In turn, Lipari et al.46 evaluated the comprehensibility, feasibility, and readability of online DM educational materials and concluded that they are not user-friendly and require improvement, suggesting that educational materials should be designed with the aim of increasing comprehensibility and feasibility.
Our visual educational material satisfactorily met these criteria because most of the pieces in the validation results were categorized as “use as is” and the adjustments made were derived from suggestions made by the experts and the target audience to complement the information. Some examples are “controllable but not curable chronic disease” or “the material is easy to understand”, “the message was clear and specific”, “it presents important elements to adopt new healthy lifestyle habits”, as emphasized by the target audience.
In line with the above, Arismendi-Bustamante et al.,47 who conducted a study to validate a game designed to promote healthy lifestyle habits and fruit and vegetable consumption in children between 7 and 12 years of age, concluded that the importance of educational material lies in the fact that it should generate a change in the behavior of the target audience. For this reason, in our study, validation by target audience was considered a fundamental step for the strategy to be of mass use and easy to implement. Furthermore, such validation allows adjusting the material following the suggestions of the end users, which could contribute to achieving favorable changes in these patients, such as a better adherence to the treatments for these diseases, such as CRPs.
Several authors have used the guidelines described by PAHO32 for the development and validation of health education materials. For example, Herrera-Guerra et al.,48 in a study in which they designed and submitted an educational brochure aimed at adults with heart failure for validation by experts (n=7) and by the target audience (n=10), found that, according to the score obtained, 71.5% of the experts and 60% of the patients reported that the material could be used as it was. In contrast, Martínez-Rincón & Cano-Ordoñez49 conducted a study in which 8 experts validated a booklet aimed at patients with acute myocardial infarction and found that the scores on all criteria were in the range of 21 to 39, indicating that the material “needed improvements”.
In our study, the score obtained in the quantitative evaluation of the technical validation ranged between 48 and 55 points in 96.3% of the educational pieces, so it was concluded that they could be used as they were. This was reflected in the results of the validation stage by the audience, in which all the items of the educational material were valid. In this sense, the fact of using the PAHO32 guidelines allowed us to develop the content in an organized manner and with a pedagogical approach, which was incorporated into the version that was validated until the final version was obtained. In a subsequent study by this group, the impact on changes in knowledge about risk factors will be evaluated.
In our study, WhatsApp was chosen as the mechanism for dissemination of the health education strategy because of its wide accessibility and ease of use. Also, the decision to implement the strategy through this application was based on the results of studies such as the one by Tang et al.,50 who conducted a quasi-experimental trial in a hospital in Klang Valley (Malaysia) with an intervention group (n=47) and a control group (n=47) to measure the effect of sending text messages for a month with information on risk factors, signs and symptoms, and prevention of coronary artery disease. They found that WhatsApp is an effective health intervention to increase the knowledge of patients with coronary artery disease and, subsequently, increase their adherence to healthy lifestyles.
Similarly, Muntaner et al.25 evaluated the feasibility and effectiveness of a 10-week WhatsApp intervention to improve health-related fitness components and CVD risk factors vs. a face-to-face intervention in adults from Balares Island, Spain. For this purpose, they selected a sample of 32 participants who were assigned to one of three groups: training (n=16), mobile (n=7) and control (n=9), concluding that the use of this application resulted in slight changes in some health-related fitness components and CVD risk factors, but that, compared to the training group and the mobile group, the WhatsApp-based physical activity intervention was less effective than the face-to-face intervention.
Along the same lines, Gallagher et al.51 described the use of mobile technology in 282 adult patients (mean age 66.5 years) with coronary artery disease treated in 9 hospitals and community centers in metropolitan and rural areas of New South Wales (Australia), showing that 91.1% used at least one technological device and 70.9% used mobile technologies (tablets or smartphones); these authors noted that individuals under 56 years of age are more likely to use any type of technology. Similarly, Piette et al.24 conducted a literature review in which they analyzed evidence on whether mobile health (mHealth) tools, including interactive voice response calls, short message service or text messaging, and smartphones, can improve lifestyle habits and cardiovascular disease management, finding that these tools could bridge the gap between what patients need and what their health systems can provide given cost constraints.
It should be noted that health education is a dynamic process that should be adjusted to the age, needs, and CRP phase in which the users are, so the development of participatory and creative educational programs according to the capabilities of human talent and institutional support allows empowering people to better manage their health.
Limitations of the study include the small number of patients who participated in the target audience validation because the research was conducted during the COVID-19 pandemic and a significant number of CRP users were not knowledgeable in the use of video call platforms. Moreover, since this was a low-budget study, it was not possible to use digital tools that provided greater versatility, and graphic design professionals were not involved, as recommended in previous studies.44
Finally, it is important to keep in mind that the implementation of the strategy presented here could be limited to a population group because in low-income countries, such as Colombia, Internet access is not as widespread as in developed countries. Also, digital illiteracy in this region is high, which is an obstacle to taking full advantage of the opportunities that the use of these tools offers in the context of health care.52,53
Conclusion
The present study made it possible to design and validate educational material aimed at users of a CRP. Because it is patient-centered and easily disseminated via a widely used social network, this material becomes a tool that can help to improve adherence to CRPs, which will result in a longer duration of their benefits. Given these good results, it is recommended to use this material in future research and to test its efficacy in research and clinical practice.
Conflicts of interest
None stated by the authors.
Funding
This study was funded by the Universidad de Santander through the internal call for proposals 021-74.
Acknowledgments
To the professionals Laura Susana Martínez, Ludivia Montaño, Erika Avellaneda, María Fernanda Monsalve, Javier Carreño, Rocío Martínez, Diana Marcela González, and Ligia Betty Arboleda, for their voluntary participation as experts in the technical validation, and to the patients from IPS Profesionales de Salud Ltda. who participated.
References
1.World Health Organization (WHO). Cardiovascular diseases (CVDs). Geneva: WHO; 2021 [cited 2024 Sep 13]. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds).
2.Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937-52. https://doi.org/d557rz.
3.Pilmore TD, Badenhop DT, Tobar DA, Keylock KT. Impact of 12-Minute Walk Test Distance on Mortality in a Group of Phase II Cardiac Rehabilitation Patients. J Clin Exerc Physiol. 2023;12(3):80-6. https://doi.org/nhjw.
4.Basuni DT, Fitria F. Six-Minute Walking Test as Prognosis Indicator in Stable Chronic CHF Patients in Second Phase Cardiac Rehabilitation. Journal Of The Indonesian Medical Association. 2023;73(2):97-101. https://doi.org/nhjx.
5.Rao A, Zecchin R, Newton PJ, Phillips JL, DiGiacomo M, Denniss AR, et al. The prevalence and impact of depression and anxiety in cardiac rehabilitation: A longitudinal cohort study. Eur J Prev Cardiol. 2020;27(5):478-89. https://doi.org/nhjz.
6.Organización Mundial de la Salud (OMS). Serie de informes técnicos No. 270. La rehabilitación en las enfermedades cardiovasculares : informe de un Comité́ de Expertos de la OMS. Geneva: OMS; 1964.
7.Saeidi M, Mostafavi S, Heidari H, Masoudi S. Effects of a comprehensive cardiac rehabilitation program on quality of life in patients with coronary artery disease. ARYA Atheroscler. 2013;9(3):179-85.
8.Rincón-Rueda ZR, Carrillo-Vásquez AC, Cepeda-Flórez KT, Quintero-Santos LS, Sánchez-Delgado JC. Impact of an 8 and 12-week Cardiac Rehabilitation Program on the Perception of Quality of Life in Patients with Coronary Angioplasty. A Randomized Controlled Trial. Rev. Investig. Innov. Cienc Salud. 2023;5(1):91-1102. https://doi.org/nhj8.
9.Sánchez-Delgado JC, Jácome-hortúa A, Martinez-Marín RdP, Suárez-López CE, Vanegas-pallares LM, Sánchez-Arias E, et al. Calidad de vida en quienes asisten o no a un programa de rehabilitación cardíaca después de ser sometidos a angioplastia coronaria. Rev Mex Enferma Cardiol. 2020;28(1):1-7.
10.Zack O, Melamed S, Silber H, Cinamon T, Levy D, Moshe S. The Effectiveness of Case-management Rehabilitation Intervention in Facilitating Return to Work and Maintenance of Employment After Myocardial Infarction: Results of a Randomized Controlled Trial. Clin Rehabil. 2022;36(6):753-66. https://doi.org/nhkb.
11.Fiabane E, Giorgi I, Candura SM, Argentero P. Return to work after coronary revascularization procedures and a patient’s job satisfaction: A prospective study. Int J Occup Med Environ Health. 2015;28(1):52-61. https://doi.org/nhkc.
12.Herdy AH, López-Jiménez F, Terzic CP, Milani M, Stein R, de Carvalho T, et al. South American guidelines for cardiovascular disease prevention and rehabilitation. Arq Bras Cardiol. 2014;103(2 Suppl 1):1-31. https://doi.org/nhkd.
13.Sánchez-Delgado JC, Camargo-Sepulveda DC, Cardona-Zapata A, Franco-Pico MY, Santos-Blanco LM, Jácome-Hortúa AM, et al. The Effects of Maintenance Cardiac Rehabilitation: A SYSTEMATIC REVIEW. J Cardiopulm Rehabil Prev. 2020;40(4):224-44. https://doi.org/nhkf.
14.Naranjo-Estupiñan NF, Díaz-Quijano FA, García RG. Influencia de la rehabilitación cardíaca sobre la tasa de re-hospitalización en pacientes con infarto agudo de miocardio, Santander, Colombia. Rev. Salud Publica. 2012;14(5):831-41.
15.Moseley AM, Elkins MR, Van der Wees PJ, Pinheiro MB. Using research to guide practice: The Physiotherapy Evidence Database (PEDro). Braz J Phys Ther. 2020;24(5):384-91. https://doi.org/ggkrwb.
16.Anderson L, Thompson DR, Oldridge N, Zwisler AD, Rees K, Martin N, et al. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst Rev. 2016;2016(1):CD001800. https://doi.org/nhkj.
17.Sisti LG, Dajko M, Campanella P, Shkurti E, Ricciardi W, de Waure C. The effect of multifactorial lifestyle interventions on cardiovascular risk factors: a systematic review and meta-analysis of trials conducted in the general population and high risk groups. Prev Med. 2018;109:82-97. https://doi.org/gc74rk.
18.Resurrección DM, Motrico E, Rubio-Valera M, Mora-Pardo JA, Moreno-Peral P. Reasons for dropout from cardiac rehabilitation programs in women: A qualitative study. PLoS One. 2018;13(7):e0200636. https://doi.org/gdvs66.
19.Arantes EC, Dessotte CAM, Dantas RAS, Rossi LA, Furuya RK. Educational program for coronary artery disease patients: results after one year. Rev Bras Enferm. 2018;71(6):2938-44. https://doi.org/gfqpz2.
20.Saffi MA, Polanczyk CA, Rabelo-Silva ER. Lifestyle interventions reduce cardiovascular risk in patients with coronary artery disease: a randomized clinical trial. Eur J Cardiovasc Nurs. 2014;13(5):436-43. https://doi.org/nhkk.
21.Wu Q, Zhang D, Zhao Q, Liu L, He Z, Chen Y, et al. Effects of transitional health management on adherence and prognosis in elderly patients with acute myocardial infarction in percutaneous coronary intervention: A cluster randomized controlled trial. PLoS One. 2019;14(5):e0217535. https://doi.org/gqcczr.
22.Molina DI, Valencia-Uribe S, Agudelo-Rojas LM. La educación a pacientes y su corresponsabilidad como herramientas terapéuticas. Rev Colomb Cardiol. 2017;24(2):176-81. https://doi.org/nhkm.
23.Coleman E, O’Connor E. The role of WhatsApp® in medical education; A scoping review and instructional design model. BMC Med Educ. 2019;19(1):279. https://doi.org/gg52s7.
24.Piette JD, List J, Rana GK, Townsend W, Striplin D, Heisler M. Mobile health devices as tools for worldwide cardiovascular risk reduction and disease management. Circulation. 2015;132(21):2012-27. https://doi.org/dscn.
25.Muntaner-Mas A, Vidal-Conti J, Borras PA, Ortega FB, Palou P. Effects of a Whatsapp-delivered physical activity intervention to enhance health-related physical fitness components and cardiovascular disease risk factors in older adults.pdf. J Sports Med Phys Fitness. 2017;57(1-2):90-102. https://doi.org/nhkn.
26.WhatsApp Inc. WhatsApp. Menlo Park: WhatsApp LLC; 2020 [cited 2024 Sep 13]. Available from: https://www.whatsapp.com/.
27.Maitra C, Rowley J. Delivering eye health education to deprived communities in India through a social media-based innovation. Health Info Libr J. 2021;38(2):139-42. https://doi.org/gm3m7g.
28.Fetters MD, Curry LA, Creswell JW. Achieving integration in mixed methods designs - Principles and practices. Health Serv Res. 2013;48(6 Pt 2):2134-56. https://doi.org/gbd7p5.
29.Guetterman TC, Fetters MD, Creswell J. Integrating quantitative and qualitative results in health science mixed methods research through joint displays. Ann Farm Med. 2015;13(6):554-61. https://doi.org/f7zj9r.
30.Colombia. Ministerio de Ciencia, Tecnología e Innovación (Minciencias). Innovación Investigación + Creación : Definiciones y reflexiones. Bogotá D.C.: Minciencias; 2021.
31.Ballesteros-Mejía M, Beltrán-Luengas EM. ¿Investigar creando? Una guía para investigación-creación en la academia. Bogotá D.C.: Universidad El Bosque; 2018.
32.Organización Panamericana de la Salud (OPS). Guía para el diseño, utilización y evaluación de material educativo de salud. Washington D.C.: OPS; 1984.
33.Hernández-Sánchez J. La ruta de la educación y comunicación para la salud. Orientaciones para su aplicación estratégica. Bogotá D.C.: Ministerio de Salud y Protección Social; 2014.
34.Hernández-Nieto H. Contributions to statistical analysis: The Coefficients of Proportional Variance, Content Validity and Kappa. Mérida: Universidad de Los Andes; 2002.
35.Barrera-Sánchez LF, Manrique-Abril FG, Ospina-Díaz JM. Propiedades psicométricas de instrumentos utilizados para evaluar material educativo en salud. Hacia Promoc. Salud. 2011;16(1):13-26.
36.Ziemandorff S, Krause A. Guía de validación de materiales educativos (con enfoque en materiales de educación sanitaria). Chiclayo: Programa de Agua y Saneamiento PROAGUA/GTZ; 2003.
37.World Medical Association (WMA). WMA Declaration of Helsinki - Ethical principles for medical research involving human subjects. In Fortaleza: 64th WMA General Assembly; 2013.
38.Colombia. Ministerio de Salud. Resolución 8430 de 1993 (octubre 4): Por la cual se establecen las normas científicas, técnicas y administrativas para la investigación en salud. Bogotá D.C.; october 4 1993.
39.Colombia. Congreso de la República. Ley Estatutaria 1581 de 2012 (octubre 17): Por la cual se dictan disposiciones generales para la protección de datos personales. Bogotá D.C.: Diario Oficial 48587; october 18 2012.
40.López-Jiménez F, Pérez-Terzic C, Zeballos PC, Anchique CV, Burdiat G, Gonzáles K, et al. Consenso de rehabilitación cardiovascular y prevención secundaria de las sociedades interamericana y sudamericana de cardiología. Rev. Urug Cardiol. 2013;28(2):189-224.
41.da Cruz FO, Ferreira EB, Vasques CI, Da Mata LR, Reis PE. Validation of an educative manual for patients with head and neck cancer submitted to radiation therapy. Rev Lat Am Enfermagem. 2016;24:e2706. https://doi.org/nhks.
42.Jolly SE, Navaneethan SD, Schold JD, Arrigain S, Konig V, Burrucker YK, et al. Development of a chronic kidney disease patient navigator program. BMC Nephrol. 2015;16:69. https://doi.org/gb4936.
43.Eschalier B, Descamps S, Boisgard S, Pereira B, Lefevre-Colau MM, Claus D, et al. Validation of an educational booklet targeted to patients candidate for total knee arthroplasty. Orthop Traumatol Surg Res. 2013;99(3):313-9. https://doi.org/f4wwcf.
44.Moura IH, Silva AFRD, Rocha ADESH, Lima LHO, Moreira TMM, Silva ARVD. Construction and validation of educational materials for the prevention of metabolic syndrome in adolescents. Rev Lat Am Enfermagem. 2017;25:e2934. https://doi.org/nhkt.
45.Brütting J, Reinhardt L, Bergmann M, Schadendorf D, Weber C, Tilgen W, et al. Quality, readability and understandability of german booklets addressing melanoma patients. J Cancer Educ. 2019;34(4):760-7. https://doi.org/nhkv.
46.Lipari M, Berlie H, Saleh Y, Hang P, Moser L. Understandability, actionability, and readability of online patient education materials about diabetes mellitus. Am J Health Syst Pharm. 2019;76(3):182-6. https://doi.org/gjqtg5.
47.Arismendi-Bustamante LJ, Carmona-Garcés IC, Rodríguez-Villamil LN, Alzate-Yepes T. Validación del juego reglado “Chefcitos”, para promover hábitos de vida saludable y el consumo de frutas y verduras en escolares mayores de siete años. Colombia, 2014. Perspect Nut Hum. 2015;17(1):67-76. https://doi.org/nn8r.
48.Herrera-Guerra EdP, Céspedes-Cuevas VM. Diseño y validación de material educativo dirigido a adultos con falla cardíaca. Revista Ciencia y Cuidado. 2020;17(1):31-42. https://doi.org/nhkw.
49.Martínez-Rincón CA, Cano-Ordoñez N. Validación de contenidos de la herramienta educativa “fortaleciendo su cuidado infarto agudo al miocardio” [thesis]. Bogotá D.C.: Facultad de Enfermería, Universidad Nacional de Colombia; 2012.
50.Tang YH, Chong MC, Chua YP, Chui PL, Tang LY, Rahmat N. The effect of mobile messaging apps on cardiac patient knowledge of coronary artery disease risk factors and adherence to a healthy lifestyle. J Clin Nurs. 2018;27(23-24):4311-20. https://doi.org/ggsgcz.
51.Gallagher R, Roach K, Sadler L, Glinatsis H, Belshaw J, Kirkness A, et al. Mobile Technology Use Across Age Groups in Patients Eligible for Cardiac Rehabilitation : Survey Study. JMIR Mhealth Uhealth. 2017;5(10):e161. https://doi.org/gcfxf5.
52.Pacheco-Gallego MC, Rubiano-Pavía LP. La tecnología y sus brechas en el impacto para la atención en salud. Acta Médica Colombiana. 2023;48(3). https://doi.org/nhkx.
53.Blumenberg C, Peiris D, de Mola CL, Sinnadurai M, Tian M, Beleigoli AM, et al. Going digital: opportunities and barriers in the use of technology for health research. Salud Publica Mex. 2022;64:S22S30.
References
1. World Health Organization (WHO). Cardiovascular diseases (CVDs). Geneva: WHO; 2021 [cited 2024 Sep 13]. Available from: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds).
2. Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937-52. https://doi.org/d557rz. DOI: https://doi.org/10.1016/S0140-6736(04)17018-9
3. Pilmore TD, Badenhop DT, Tobar DA, Keylock KT. Impact of 12-Minute Walk Test Distance on Mortality in a Group of Phase II Cardiac Rehabilitation Patients. J Clin Exerc Physiol. 2023;12(3):80-6. https://doi.org/nhjw. DOI: https://doi.org/10.31189/2165-6193-12.3.80
4. Basuni DT, Fitria F. Six-Minute Walking Test as Prognosis Indicator in Stable Chronic CHF Patients in Second Phase Cardiac Rehabilitation. Journal Of The Indonesian Medical Association. 2023;73(2):97-101. https://doi.org/nhjx. DOI: https://doi.org/10.47830/jinma-vol.73.2-2023-786
5. Rao A, Zecchin R, Newton PJ, Phillips JL, DiGiacomo M, Denniss AR, et al. The prevalence and impact of depression and anxiety in cardiac rehabilitation: A longitudinal cohort study. Eur J Prev Cardiol. 2020;27(5):478-89. https://doi.org/nhjz. DOI: https://doi.org/10.1177/2047487319871716
6. Organización Mundial de la Salud (OMS). Serie de informes técnicos No. 270. La rehabilitación en las enfermedades cardiovasculares : informe de un Comité́ de Expertos de la OMS. Geneva: OMS; 1964.
7. Saeidi M, Mostafavi S, Heidari H, Masoudi S. Effects of a comprehensive cardiac rehabilitation program on quality of life in patients with coronary artery disease. ARYA Atheroscler. 2013;9(3):179-85. DOI: https://doi.org/10.1136/heartjnl-2013-304613.387
8. Rincón-Rueda ZR, Carrillo-Vásquez AC, Cepeda-Flórez KT, Quintero-Santos LS, Sánchez-Delgado JC. Impact of an 8 and 12-week Cardiac Rehabilitation Program on the Perception of Quality of Life in Patients with Coronary Angioplasty. A Randomized Controlled Trial. Rev. Investig. Innov. Cienc Salud. 2023;5(1):91-1102. https://doi.org/nhj8. DOI: https://doi.org/10.46634/riics.151
9. Sánchez-Delgado JC, Jácome-hortúa A, Martinez-Marín RdP, Suárez-López CE, Vanegas-pallares LM, Sánchez-Arias E, et al. Calidad de vida en quienes asisten o no a un programa de rehabilitación cardíaca después de ser sometidos a angioplastia coronaria. Rev Mex Enferma Cardiol. 2020;28(1):1-7.
10. Zack O, Melamed S, Silber H, Cinamon T, Levy D, Moshe S. The Effectiveness of Case-management Rehabilitation Intervention in Facilitating Return to Work and Maintenance of Employment After Myocardial Infarction: Results of a Randomized Controlled Trial. Clin Rehabil. 2022;36(6):753-66. https://doi.org/nhkb. DOI: https://doi.org/10.1177/02692155221076826
11. Fiabane E, Giorgi I, Candura SM, Argentero P. Return to work after coronary revascularization procedures and a patient’s job satisfaction: A prospective study. Int J Occup Med Environ Health. 2015;28(1):52-61. https://doi.org/nhkc. DOI: https://doi.org/10.2478/s13382-014-0313-5
12. Herdy AH, López-Jiménez F, Terzic CP, Milani M, Stein R, de Carvalho T, et al. South American guidelines for cardiovascular disease prevention and rehabilitation. Arq Bras Cardiol. 2014;103(2 Suppl 1):1-31. https://doi.org/nhkd. DOI: https://doi.org/10.5935/abc.2014S003
13. Sánchez-Delgado JC, Camargo-Sepulveda DC, Cardona-Zapata A, Franco-Pico MY, Santos-Blanco LM, Jácome-Hortúa AM, et al. The Effects of Maintenance Cardiac Rehabilitation: A SYSTEMATIC REVIEW. J Cardiopulm Rehabil Prev. 2020;40(4):224-44. https://doi.org/nhkf. DOI: https://doi.org/10.1097/HCR.0000000000000520
14. Naranjo-Estupiñan NF, Díaz-Quijano FA, García RG. Influencia de la rehabilitación cardíaca sobre la tasa de re-hospitalización en pacientes con infarto agudo de miocardio, Santander, Colombia. Rev. Salud Publica. 2012;14(5):831-41.
15. Moseley AM, Elkins MR, Van der Wees PJ, Pinheiro MB. Using research to guide practice: The Physiotherapy Evidence Database (PEDro). Braz J Phys Ther. 2020;24(5):384-91. https://doi.org/ggkrwb. DOI: https://doi.org/10.1016/j.bjpt.2019.11.002
16. Anderson L, Thompson DR, Oldridge N, Zwisler AD, Rees K, Martin N, et al. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst Rev. 2016;2016(1):CD001800. https://doi.org/nhkj. DOI: https://doi.org/10.1002/14651858.CD001800.pub3
17. Sisti LG, Dajko M, Campanella P, Shkurti E, Ricciardi W, de Waure C. The effect of multifactorial lifestyle interventions on cardiovascular risk factors: a systematic review and meta-analysis of trials conducted in the general population and high risk groups. Prev Med. 2018;109:82-97. https://doi.org/gc74rk. DOI: https://doi.org/10.1016/j.ypmed.2017.12.027
18. Resurrección DM, Motrico E, Rubio-Valera M, Mora-Pardo JA, Moreno-Peral P. Reasons for dropout from cardiac rehabilitation programs in women: A qualitative study. PLoS One. 2018;13(7):e0200636. https://doi.org/gdvs66. DOI: https://doi.org/10.1371/journal.pone.0200636
19. Arantes EC, Dessotte CAM, Dantas RAS, Rossi LA, Furuya RK. Educational program for coronary artery disease patients: results after one year. Rev Bras Enferm. 2018;71(6):2938-44. https://doi.org/gfqpz2. DOI: https://doi.org/10.1590/0034-7167-2017-0280
20. Saffi MA, Polanczyk CA, Rabelo-Silva ER. Lifestyle interventions reduce cardiovascular risk in patients with coronary artery disease: a randomized clinical trial. Eur J Cardiovasc Nurs. 2014;13(5):436-43. https://doi.org/nhkk. DOI: https://doi.org/10.1177/1474515113505396
21. Wu Q, Zhang D, Zhao Q, Liu L, He Z, Chen Y, et al. Effects of transitional health management on adherence and prognosis in elderly patients with acute myocardial infarction in percutaneous coronary intervention: A cluster randomized controlled trial. PLoS One. 2019;14(5):e0217535. https://doi.org/gqcczr. DOI: https://doi.org/10.1371/journal.pone.0217535
22. Molina DI, Valencia-Uribe S, Agudelo-Rojas LM. La educación a pacientes y su corresponsabilidad como herramientas terapéuticas. Rev Colomb Cardiol. 2017;24(2):176-81. https://doi.org/nhkm. DOI: https://doi.org/10.1016/j.rccar.2016.07.013
23. Coleman E, O’Connor E. The role of WhatsApp® in medical education; A scoping review and instructional design model. BMC Med Educ. 2019;19(1):279. https://doi.org/gg52s7. DOI: https://doi.org/10.1186/s12909-019-1706-8
24. Piette JD, List J, Rana GK, Townsend W, Striplin D, Heisler M. Mobile health devices as tools for worldwide cardiovascular risk reduction and disease management. Circulation. 2015;132(21):2012-27. https://doi.org/dscn. DOI: https://doi.org/10.1161/CIRCULATIONAHA.114.008723
25. Muntaner-Mas A, Vidal-Conti J, Borras PA, Ortega FB, Palou P. Effects of a Whatsapp-delivered physical activity intervention to enhance health-related physical fitness components and cardiovascular disease risk factors in older adults.pdf. J Sports Med Phys Fitness. 2017;57(1-2):90-102. https://doi.org/nhkn. DOI: https://doi.org/10.23736/S0022-4707.16.05918-1
26. WhatsApp Inc. WhatsApp. Menlo Park: WhatsApp LLC; 2020 [cited 2024 Sep 13]. Available from: https://www.whatsapp.com/.
27. Maitra C, Rowley J. Delivering eye health education to deprived communities in India through a social media-based innovation. Health Info Libr J. 2021;38(2):139-42. https://doi.org/gm3m7g. DOI: https://doi.org/10.1111/hir.12370
28. Fetters MD, Curry LA, Creswell JW. Achieving integration in mixed methods designs - Principles and practices. Health Serv Res. 2013;48(6 Pt 2):2134-56. https://doi.org/gbd7p5. DOI: https://doi.org/10.1111/1475-6773.12117
29. Guetterman TC, Fetters MD, Creswell J. Integrating quantitative and qualitative results in health science mixed methods research through joint displays. Ann Farm Med. 2015;13(6):554-61. https://doi.org/f7zj9r. DOI: https://doi.org/10.1370/afm.1865
30. Colombia. Ministerio de Ciencia, Tecnología e Innovación (Minciencias). Innovación Investigación + Creación : Definiciones y reflexiones. Bogotá D.C.: Minciencias; 2021.
31. Ballesteros-Mejía M, Beltrán-Luengas EM. ¿Investigar creando? Una guía para investigación-creación en la academia. Bogotá D.C.: Universidad El Bosque; 2018.
32. Organización Panamericana de la Salud (OPS). Guía para el diseño, utilización y evaluación de material educativo de salud. Washington D.C.: OPS; 1984.
33. Hernández-Sánchez J. La ruta de la educación y comunicación para la salud. Orientaciones para su aplicación estratégica. Bogotá D.C.: Ministerio de Salud y Protección Social; 2014.
34. Hernández-Nieto H. Contributions to statistical analysis: The Coefficients of Proportional Variance, Content Validity and Kappa. Mérida: Universidad de Los Andes; 2002.
35. Barrera-Sánchez LF, Manrique-Abril FG, Ospina-Díaz JM. Propiedades psicométricas de instrumentos utilizados para evaluar material educativo en salud. Hacia Promoc. Salud. 2011;16(1):13-26.
36. Ziemandorff S, Krause A. Guía de validación de materiales educativos (con enfoque en materiales de educación sanitaria). Chiclayo: Programa de Agua y Saneamiento PROAGUA/GTZ; 2003.
37. World Medical Association (WMA). WMA Declaration of Helsinki - Ethical principles for medical research involving human subjects. In Fortaleza: 64th WMA General Assembly; 2013.
38. Colombia. Ministerio de Salud. Resolución 8430 de 1993 (octubre 4): Por la cual se establecen las normas científicas, técnicas y administrativas para la investigación en salud. Bogotá D.C.; october 4 1993.
39. Colombia. Congreso de la República. Ley Estatutaria 1581 de 2012 (octubre 17): Por la cual se dictan disposiciones generales para la protección de datos personales. Bogotá D.C.: Diario Oficial 48587; october 18 2012.
40. López-Jiménez F, Pérez-Terzic C, Zeballos PC, Anchique CV, Burdiat G, Gonzáles K, et al. Consenso de rehabilitación cardiovascular y prevención secundaria de las sociedades interamericana y sudamericana de cardiología. Rev. Urug Cardiol. 2013;28(2):189-224.
41. da Cruz FO, Ferreira EB, Vasques CI, Da Mata LR, Reis PE. Validation of an educative manual for patients with head and neck cancer submitted to radiation therapy. Rev Lat Am Enfermagem. 2016;24:e2706. https://doi.org/nhks. DOI: https://doi.org/10.1590/1518-8345.0949.2706
42. Jolly SE, Navaneethan SD, Schold JD, Arrigain S, Konig V, Burrucker YK, et al. Development of a chronic kidney disease patient navigator program. BMC Nephrol. 2015;16:69. https://doi.org/gb4936. DOI: https://doi.org/10.1186/s12882-015-0060-2
43. Eschalier B, Descamps S, Boisgard S, Pereira B, Lefevre-Colau MM, Claus D, et al. Validation of an educational booklet targeted to patients candidate for total knee arthroplasty. Orthop Traumatol Surg Res. 2013;99(3):313-9. https://doi.org/f4wwcf. DOI: https://doi.org/10.1016/j.otsr.2013.01.007
44. Moura IH, Silva AFRD, Rocha ADESH, Lima LHO, Moreira TMM, Silva ARVD. Construction and validation of educational materials for the prevention of metabolic syndrome in adolescents. Rev Lat Am Enfermagem. 2017;25:e2934. https://doi.org/nhkt. DOI: https://doi.org/10.1590/1518-8345.2024.2934
45. Brütting J, Reinhardt L, Bergmann M, Schadendorf D, Weber C, Tilgen W, et al. Quality, readability and understandability of german booklets addressing melanoma patients. J Cancer Educ. 2019;34(4):760-7. https://doi.org/nhkv. DOI: https://doi.org/10.1007/s13187-018-1369-x
46. Lipari M, Berlie H, Saleh Y, Hang P, Moser L. Understandability, actionability, and readability of online patient education materials about diabetes mellitus. Am J Health Syst Pharm. 2019;76(3):182-6. https://doi.org/gjqtg5. DOI: https://doi.org/10.1093/ajhp/zxy021
47. Arismendi-Bustamante LJ, Carmona-Garcés IC, Rodríguez-Villamil LN, Alzate-Yepes T. Validación del juego reglado “Chefcitos”, para promover hábitos de vida saludable y el consumo de frutas y verduras en escolares mayores de siete años. Colombia, 2014. Perspect Nut Hum. 2015;17(1):67-76. https://doi.org/nn8r. DOI: https://doi.org/10.17533/udea.penh.v17n1a06
48. Herrera-Guerra EdP, Céspedes-Cuevas VM. Diseño y validación de material educativo dirigido a adultos con falla cardíaca. Revista Ciencia y Cuidado. 2020;17(1):31-42. https://doi.org/nhkw. DOI: https://doi.org/10.22463/17949831.1366
49. Martínez-Rincón CA, Cano-Ordoñez N. Validación de contenidos de la herramienta educativa “fortaleciendo su cuidado infarto agudo al miocardio” [thesis]. Bogotá D.C.: Facultad de Enfermería, Universidad Nacional de Colombia; 2012.
50. Tang YH, Chong MC, Chua YP, Chui PL, Tang LY, Rahmat N. The effect of mobile messaging apps on cardiac patient knowledge of coronary artery disease risk factors and adherence to a healthy lifestyle. J Clin Nurs. 2018;27(23-24):4311-20. https://doi.org/ggsgcz. DOI: https://doi.org/10.1111/jocn.14538
51. Gallagher R, Roach K, Sadler L, Glinatsis H, Belshaw J, Kirkness A, et al. Mobile Technology Use Across Age Groups in Patients Eligible for Cardiac Rehabilitation : Survey Study. JMIR Mhealth Uhealth. 2017;5(10):e161. https://doi.org/gcfxf5. DOI: https://doi.org/10.2196/mhealth.8352
52. Pacheco-Gallego MC, Rubiano-Pavía LP. La tecnología y sus brechas en el impacto para la atención en salud. Acta Médica Colombiana. 2023;48(3). https://doi.org/nhkx. DOI: https://doi.org/10.36104/amc.2023.2945
53. Blumenberg C, Peiris D, de Mola CL, Sinnadurai M, Tian M, Beleigoli AM, et al. Going digital: opportunities and barriers in the use of technology for health research. Salud Publica Mex. 2022;64:S22S30. DOI: https://doi.org/10.21149/12977
How to Cite
APA
ACM
ACS
ABNT
Chicago
Harvard
IEEE
MLA
Turabian
Vancouver
Download Citation
CrossRef Cited-by
Dimensions
PlumX
Article abstract page views
Downloads
License
Copyright (c) 2024 Revista de la Facultad de Medicina

This work is licensed under a Creative Commons Attribution 3.0 Unported License.
-


















