


Publicado
Thromboelastographyguided transfusion therapy in a pregnant patient with hemorrhagic dengue fever hospitalized in icu. Case report
Tromboelastografía para dirigir la terapia transfusional en dengue hemorrágico en una paciente embarazada hospitalizada en UCI: Reporte de caso
DOI:
https://doi.org/10.15446/cr.v3n1.58952Palabras clave:
Severe Dengue, Thrombelastography, Pregnancy (en)Dengue hemorrágico, Tromboelastografía, Embarazo (es)
Dengue fever is the biggest public health issue in tropical countries. A significant percentage of patients who suffer from this disease require admission to the intensive care unit (ICU) due to the severity of the clinical picture. This case reports the clinical evolution of an eight-week pregnant woman with dengue fever associated with thrombocytopenia and leukopenia. The patient comes from an endemic area for tropical diseases, fact that led to diagnose dengue fever with hemorrhagic characteristics.
During her stay in the ICU, the patient presented with first trimester bleeding and placental hematoma. Therefore, and considering the pregnancy and the risk of loss, the hematological function was monitored through thromboelastography. The transfusion of blood products was decided according to the specific findings. Controlling and reversing the obstetric bleeding process was possible, the patient condition evolved favorably, and she was subsequently discharged from the ICU. This article reports on the usefulness of dynamic monitoring the hematological function using thromboelastography in patients with hemorrhagic dengue fever and special conditions such as pregnancy.
El dengue es una enfermedad considerada como el mayor problema de salud pública en países tropicales. Un importante porcentaje de pacientes que lo padecen requieren ingreso a la unidad de cuidados intensivos (UCI) debido a la severidad del cuadro clínico. El presente caso reporta la evolución clínica de una gestante de ocho semanas con cuadro febril asociado a trombocitopenia y leucopenia. La paciente procede de un área endémica para enfermedades tropicales, lo que lleva a realizar un diagnóstico de dengue con características hemorrágicas.
En la UCI, la paciente presenta hemorragia del primer trimestre y hematoma placentario, por lo que, ante el estado de embarazo y el riesgo de pérdida del mismo, se decide monitorizar la función hematológica con tromboelastrografía y transfundir hemoderivados según los hallazgos específicos. Se logra controlar y revertir el proceso de sangrado obstétrico con evolución favorable de la paciente y egreso de UCI. En el presente artículo se reporta la utilidad de la monitorización dinámica de la función hematológica con tromboelastografia en pacientes con dengue hemorrágico y condiciones especiales, tales como el embarazo.
https://doi.org/10.15446/cr.v3n1.58952
Thromboelastographyguided transfusion therapy in a pregnant patient with hemorrhagic dengue fever hospitalized in ICU. CASE REPORT
Palabras clave: Dengue hemorrágico; Tromboelastografía; Embarazo
Keywords: Severe Dengue; Thrombelastography; Pregnancy
José A. Rojas, MD
Daniel Molano-Franco, MD
Tito Jiménez, MD
Albert Valencia, MD
Rafael Leal, MD
Pablo Méndez, MD
Victor Nieto, MD
Diego Hernández, MD
Intensive Care Unit
– Clínica Universitaria Colombia –
Critical Medicine Research Group
– Fundación Universitaria Sanitas –
Bogotá, D.C. – Colombia
Corresponding author:
Daniel Molano-Franco.
Clínica Universitaria Colombia – Calle 22b # 66-46, piso 3, Unidad de cuidado intensivo. Bogotá D.C. – Colombia.
Phone number: +57 3112263388
ABSTRACT
Dengue fever is the biggest public health issue in tropical countries. A significant percentage of patients who suffer from this disease require admission to the intensive care unit (ICU) due to the severity of the clinical picture. This case reports the clinical evolution of an eight-week pregnant woman with dengue fever associated with thrombocytopenia and leukopenia. The patient comes from an endemic area for tropical diseases, fact that led to diagnose dengue fever with hemorrhagic characteristics.
During her stay in the ICU, the patient presented with first trimester bleeding and placental hematoma. Therefore, and considering the pregnancy and the risk of loss, the hematological function was monitored through thromboelastography. The transfusion of blood products was decided according to the specific findings. Controlling and reversing the obstetric bleeding process was possible, the patient condition evolved favorably, and she was subsequently discharged from the ICU. This article reports on the usefulness of dynamic monitoring the hematological function using thromboelastography in patients with hemorrhagic dengue fever and special conditions such as pregnancy.
IntroducTion
Dengue fever is a tropical disease characterized by high fever and bleeding caused by the dengue arbovirus. It is transmitted by the bite of Aedes aegypti, of the flavivirus genus, a species largely found in territories below 1800 masl. According to the World Health Organization (WHO), dengue fever is the biggest public health issue in tropical and subtropical countries, accounting for more than 500 000 hospitalizations per year, with a mortality rate of 1% (1).
In 2012, 54 726 cases of dengue fever were reported in Colombia, of which 1 641 corresponded to severe dengue, and 25 174 to patients under 15 years of age, with a mortality rate of 3.9%. Such figures labeled the country as an endemic territory for dengue fever in the past years (2). Data on its incidence in obstetric population are not clear; however, a susceptibility condition related to the development of infections has been reported, as well as an increase in their severity. In addition, growing evidence on predisposition to the development of activation pictures and severe immune response has been found, especially in cases of Plasmodium falciparum and Listeria monocytogenes infections, and viral infections such as influenza A(H1N1) (3).
Recently, guided transfusion therapy techniques, such as thromboelastography, have been implemented in patients with critical illnesses to evaluate the different phases of coagulation and clot lysis. The reduction of morbimortality and the cost associated with health care, as a result of the decrease in the number of transfusions, have been described as the main advantages of their use (4). Although reports evidencing the usefulness of thromboelastography in sepsis (5) can be found, its clinical applicability in patients with dengue fever infection and hemorrhagic complications requiring administration of blood products is unknown to date.
Considering the facts exposed above, this article presents the case of a pregnant patient infected with dengue hemorrhagic fever, treated in a university hospital of Colombia. This patient underwent a transfusion therapy through thromboelastography with the purpose of controlling obstetric bleeding and avoiding pregnancy loss.
Case presentation
Patient Information
33-year-old pregnant housewife, born in Bogotá D.C.
Clinical findings
33-year-old woman, with no previous medical-surgical history, and eight weeks into her second pregnancy by the time she attends the emergency department. She reported a clinical picture of five days of repeated intermittent fever of 38.3°C, associated with chills, generalized myalgias, musculoskeletal, recto-ocular and headache pain, as well as nausea, asthenia, adynamia and abdominal pain.
She denies any history of trauma and vaginal or urinary tract infections. Likewise, she reported that, by the time of consultation, she was getting prenatal care and that no abnormality had been found. She also reported that seven days before the consultation she had been in an endemic region for multiple tropical diseases, a place located at 300 masl; further investigation revealed that she received multiple insect bites during the trip.
Calendar and diagnostic evaluation
Based on clinical findings, a possible dengue virus infection was suspected and paraclinical tests were requested for admission (Table 1). Physical examination on admission did not show any lesion associated with hemorrhagic phenomena such as ecchymosis, petechia or hematoma. The only abnormal finding developed during her stay in the emergency room after presenting with an episode of acute, sparse and bright genital bleeding. Pelvic examination was omitted, and an obstetric ultrasound was performed, confirming fetal viability and the presence of a retroplacental hematoma of approximately 50%, which could be a sign of threatened abortion. Due to the risk of hemorrhagic complication, the patient was transferred to the ICU, where the dengue infection diagnosis was confirmed after obtaining positive IgG and IgM tests for dengue fever.
Table 1. Hemogram and blood chemistry from admission until day five.
|
Paraclinical exams |
||||||||||||
|
Leukocytes |
Neutrophils |
Platelet count c/mm3 |
Hgb/dl |
Hct (%) |
AST (U/L) |
ALT (U/L) |
TB (mg/dl) |
DB (mg/dl) |
PT |
PTT (seg) |
LDH (mg/dl) |
|
|
Day 1 |
2500 |
1800 |
117000 |
13.6 |
41 |
-- |
-- |
-- |
-- |
-- |
-- |
-- |
|
Day 2 |
3250 |
1340 |
45000 |
14 |
41 |
1022 |
1172 |
0.29 |
0.15 |
11 |
46 |
1118 |
|
Day 3 (0 hour) |
3000 |
1250 |
30000 |
14 |
42 |
919 |
954 |
-- |
-- |
11 |
46 |
-- |
|
Day 3 |
-- |
-- |
20700 |
14.2 |
42 |
-- |
-- |
-- |
-- |
-- |
-- |
-- |
|
Day 4 |
4250 |
2300 |
42000 |
13 |
43 |
382 |
457 |
0.5 |
0.29 |
11 |
28 |
320 |
|
Day 5 |
5300 |
2700 |
65000 |
13 |
40 |
-- |
-- |
-- |
-- |
-- |
-- |
-- |
|
AST: Aspartato transferasa; ALT: Alanino transferasa; BT: Bilirrubina Total; BD: Bilirrubina Directa; c: células; Ct: Control; LDH: Lactato Deshidrogenasa; PT: Tiempo de Protrombina; PTT: Tiempo Parcial de Tromboplastina; Rto: Recuento; Hgb: hemoglobina, Hcto: hematocrito; PT: tiempo protrombina; PTT: tiempo de tromboplastina; LDH: deshidrogenasa láctica. |
||||||||||||
Source: Own elaboration based on the data obtained in the study.
Therapeutic management
On the third day of hospitalization and facing an abrupt reduction of platelet count, a platelet transfusion was indicated and a thromboelastogram (TbEg) was performed to determine the coagulation status. TbEg reported R: 12.5, K: 13.0, alpha: 20.4, MA: 27.2 (Figure 1A). Furthermore, a control complete blood count taken six hours after the platelet transfusion yielded the following results: Hg: 14.4 g/dL, Hct: 42.3%, Polys: 50%, Lymphs: 40.1%, platelet count: 20 700 c/mm3. Taking into account the risk of miscarriage due to persistent vaginal bleeding, a transfusion of blood products was administered again, this time with platelets and fresh frozen plasma (FFP); phytonadione 10mg was initiated intravenously (IV). The control thromboelastograms requested within the next 24 hours are shown below (Figure 1 A, B, C and D).
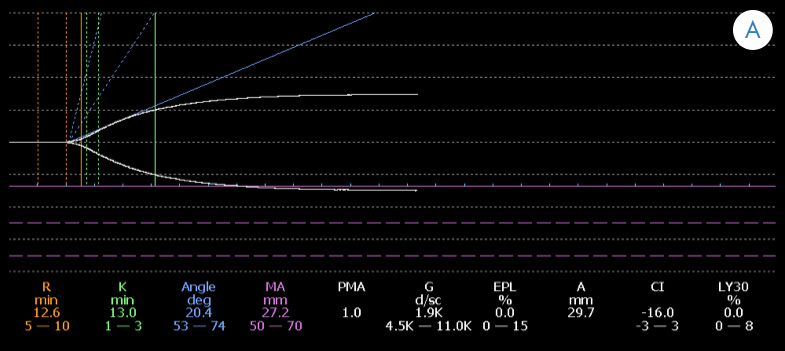
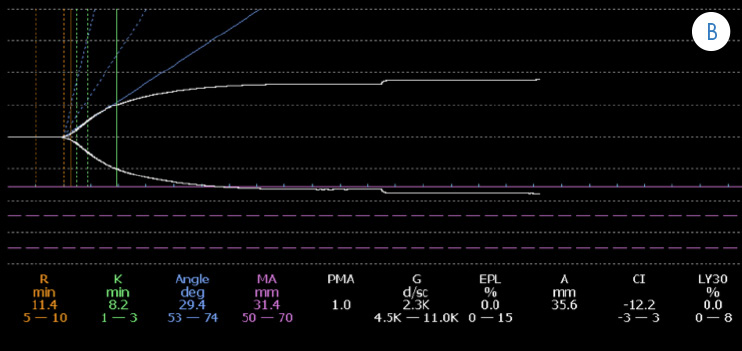
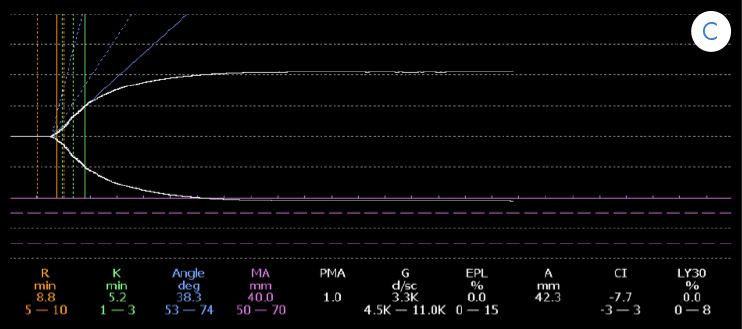
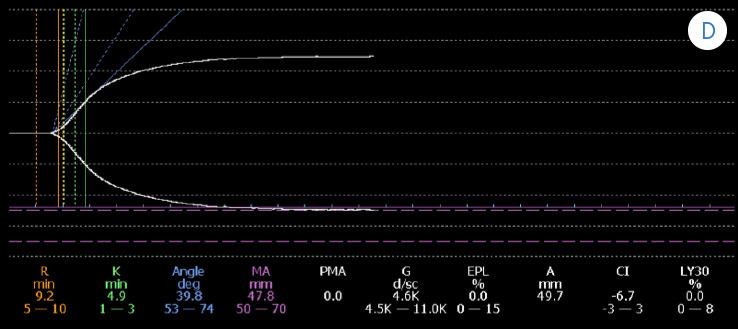
Figure 1 A. Initial thromboelastogram showing an anticoagulation pattern and deficiency of coagulation factors (prolonged k time, decreased alpha angle, and decreased maximum amplitude).
Figure 1 B. Control thromboelastogram (TbEg) # 1 done after the transfusion of platelets and of 10U FFP (gradual correction in K time values, alpha angle, and maximum amplitude).
Figure 1 C. Control TbEg # 2 done after the second transfusion of platelet concentrate.
Figure 1 D. Control TbEg # 3 done after the FFP transfusion (correction of K time, alpha angle, and maximum amplitude close to reference values).
Monitoring and evolution
During ICU stay, a positive IgM and IgG serum antigen for dengue fever was reported. In addition, the evolution of the patient was satisfactory, and no new episodes of bleeding occurred. On the sixth day of evolution of the disease and with TbEg in the correction phase, the patient was discharged from the ICU without complications. Multidisciplinary follow-up by obstetrics, infectology and psychology was indicated. Seven days after the discharge, an obstetric ultrasound was performed, which showed that retroplacental hematoma persisted with a 50% decrease of the original size and fetal viability.
Discussion
The clinical presentation of dengue is broad and depends on the phases of the disease, which range between asymptomatic or febrile cases during the febrile phase (0-3 days), severe cases of bleeding, shock or organ dysfunction during the critical phase (3-6 days), and the resolution of symptoms in the convalescent phase (>6 days). Recently, a classification of this disease was made according to its clinical presentation to timely identify severe cases and establish proper treatment. Such classification is based on the presence or absence of warning signs and severe dengue states characterized by shock, bleeding or organ involvement such as myocarditis, hepatitis, encephalitis, and renal failure (6).
The risk of hemorrhagic dengue fever during pregnancy is determined according to the trimester in which it is contracted, and includes vaginal bleeding, threatened abortion, and abruptio placentae. In this regard, Carles et al. (7) determined an increased preterm delivery rate of 55% in French Guyana, which is similar to the findings reported by Poli et al. (8). Restrepo et al. (9) reported an increase in the incidence of threatened abortion and preterm delivery in patients with dengue hemorrhagic fever in Colombia.
A more recent study reports that 10% of cases show hemorrhagic events associated with maternal dengue infection, stressing that an association with retroplacental hematoma is observed during the first trimester (10). Evidence suggesting that there is no relationship between dengue and congenital malformations during the first trimester of pregnancy has been compiled. However, in India, Sharma & Gulati (11) have reported some cases of neural tube defects following a regional dengue epidemic, without finding associated chromosomal defects (11).
Most individuals who are infected and develop the disease, evolve to classic dengue fever, a self-limited febrile disease that usually does not represent any complication. Nevertheless, a variable amount of patients develop spontaneous bleeding, decreased platelet count and signs of plasma extravasation; all these manifestations define the dengue hemorrhagic fever.
Hemorrhagic manifestations have been reported in 35-50% of cases, the most common being epistaxis, gingivorrhagia, and gastrointestinal bleeding (12-13). Despite this trend, some authors, such as Chaudhary et al. (14), consider that there is no association between hemorrhagic manifestations and platelet count, although, this claim has not been confirmed yet due to the heterogeneity of patient selection. Deep thrombocytopenia may be strongly related to the severity of dengue in special populations such as children and pregnant women, for whom it is estimated in terms of major and minor bleedings and signs of plasma extravasation.
Discussions around transfusions, particularly about platelets, have been held regarding pregnant women. To date, no information has been published that could certainly associate abortion with dengue infection during the first trimester, whereas an association between the presence of a placental hematoma and the risk of miscarriage has been reported in 5 to 17% of losses in patients with hematomas, with an OR of 2.18 (1.20-3.67) (15-17).
Although multiple etiologic causes of retroplacental hematomas have been found, including fetal malformations, corpus luteum insufficiency, trauma and perinatal infections such as parvovirus and toxoplasmosis, they have also been reported in infections contracted at the uterine and systemic level (18). When considering the case presented here, it is possible to affirm that the placental hematoma was associated with a systemic viral infection, which worsens due to the presence of hematological dysfunction with severe thrombocytopenia.
In this context, there is no protocol to determine whether the correction of coagulopathy improves obstetric prognosis and reduces the risk of abortion. In a series of 53 patients, Basurko et al. (10) reported two cases of early abortion due to utero-vaginal bleeding and five hemorrhagic complications at the time of delivery. Another study by Chotigeat et al. (19) made a comparison between patients who were transfused platelets before delivery and patients who were not transfused, finding a reduction of associated bleeding events in the first group.
Thromboelastography assesses hemostasis from a functional point of view, and is represented by the interpretation of the cellular coagulation model. Its application in different clinical scenarios, especially in cardiovascular surgery patients and trauma patients, is a proper option to correct acute hematological alterations and to decrease the unnecessary use of blood products. (20). It is worth noting that conventional coagulation tests do not allow managing the underlying coagulation disorder, which often results in unnecessary replacement of blood components. Thus, thromboelastography allows physicians to recognize a coagulopathy and, more importantly, to understand the underlying coagulation disorder (20).
In this case, the alteration was determined at its full extent by using thromboelastography, which allowed transfusing platelets to correct this variable and to ensure adequate platelet function, therefore, resolving the vaginal bleeding. Although determining if this behavior was beneficial to the patient or if the resolution of vaginal bleeding and subsequent reabsorption of the hematoma could have been achieved only through resting and medical management of the viral infection symptoms can be further discussed, this report raises the possibility of including this treatment in the medical practice.
The literature does not provide records regarding the assessment of the performance and the usefulness of thromboelastography as a dynamic test to define the correctness of coagulopathy and, specifically, thrombocytopenia in patients with dengue hemorrhagic fever, as well as in pregnant patients with dengue fever. Its use has been reported in relation to other obstetric conditions, such as acute fatty liver of pregnancy (21), which is another reason to consider this report as relevant.
However, this reports also lacks information on other causes of placental hematoma, such as fetal malformations, which were not determined since the described clinical management was selected due to the gestational age of the patient and the acute course of the disease.
Conclusion
Patients with retroplacental hematoma and dengue fever infection associated with severe thrombocytopenia are at increased risk of miscarriage and fetal loss. In consequence, coagulopathy correction may improve pregnancy prognosis. Conventional coagulation tests may underestimate the risk of coagulopathy and increased bleeding secondary to hematoma. Thromboelastography may be a useful tool for identifying patients at high risk of bleeding due to severe thrombocytopenia in cases of dengue fever during pregnancy, so its use in institutions where this technology is available should be considered.
Conflict of interests
None stated by the authors.
Funding
None stated by the authors.
References
1.World Health Organization. Dengue Haemorrhagic Fever: early recognition, diagnosis and hospital management. An audiovisual guide for health-care workers responding to outbreaks. WHO; 2006 [cited Feb 02 2017]. Available from: https://goo.gl/Mv8kph.
2.Ministerio de Salud y Protección Social. Circular 8. Instrucciones para la intensificación de las acciones de vigilancia, prevención, atención y control del dengue y dengue grave en Colombia. Bogota, D.C.: MinSalud;2013.
3.Kourtis AP, Read JS, Jamieson DJ. Pregnancy and infection. N Engl J Med. 2014;370(23):2211-18. http://doi.org/bx5c.
4.Levi M, Hunt BJ. A critical appraisal of point-of-care coagulation testing in critically ill patients. J Thromb Haemost. 2015;13(11):1960-7. http://doi.org/bx5d.
5.Zhong S, Zhang C, Hu J, Tang Z. Evaluation of coagulation disorders with thrombelastography in patients with sepsis. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2016;28(2):153-8. 10.3760/cma.j.issn.2095-4352.2016.02.013.
6.Ministerio de la Protección Social, Instituto Nacional de Salud, Organización Panamericana de la Salud.. Guía para la atención clínica integral del paciente con dengue. Bogotá: MinSalud;2010 [cited Feb 02 2017]. Available from: https://goo.gl/0niJbQ.
7.Carles G, Peiffer H, Talarmin A. Effects of dengue fever during pregnancy in French Guiana. Clin Infect Dis. 1999;28(3):637-40. http://doi.org/cg8wdr.
8.Poli L, Chungue E, Soulignac O, Gestas P, Kuo P, Papouin-Rauzy M. Materno-Fetal Dengue. Apropos o 5 cases observed during the epidemics in Tahiti (1989). Bull Soc Pathol Exot. 1991;84(5 Pt 5):513-21.
9.Restrepo BN, Isaza DM, Salazar CL, Ramírez JL, Upegui GE, Ospina M, et al. Efectos por la infección del virus del dengue sobre el feto y el recién nacido. Biomedica. 2003;23(4):416-23. http://doi.org/bx5v.
10.Basurko C, Carles G, Youssef M, Guindi W. Maternal and Fetal consequences of dengue fever during pregnancy. Eur J Obstet Gynecol Reprod Biol. 2009;147 (1):29-32. http://doi.org/dvg8hq.
11.Sharma JB, Gulati N. Potential relationship between dengue fever and neural tube defects in a northern district on India. Int J Gynaecol Obstet. 1992;39(4):291-5. http://doi.org/bwzcmf.
12.Makroo RN, Raina V, Kumar P, Kanth RK. Role of platelet transfusion in the management of dengue patients in a tertiary care hospital. Asian J Tranfus Sci. 2007;1(1):4-7. http://doi.org/b7bkqg.
13.Chairulfatah A, Setiabudi D, Agoes R, Colebunder R. Thrombocytopenia and platelet transfusion in dengue haemorrhagic fever and dengue shock syndrome. WHO Dengue bulletin. 2003;27: 141-3
14.Chaudhary R, Khetan D, Sinha S, Sinha P, Sonker A, Pandey P, et al. Transfusion support to dengue patients in a hospital based blood transfusion service in north India. Transfus Apheric Sci. 2006;35(3):239-44. http://doi.org/cz5m85.
15. Şükür YE, Göç G, Köse O, Açmaz G, Özmen B, Atabekoğlu CS, et al. The effects of subchorionic hematoma on pregnancy outcome in patients with threatened abortion. J Turk Ger Gynecol Assoc. 2014;15(4):239-42. http://doi.org/bx5z.
16.Soldo V, Cutura N, Zamurovic M. Threatened miscarriage in the first trimester and retrochorial hematomas: sonographic evaluation and significance. Clin Exp Obstet Gynecol. 2013;40(4): 548-50.
17.Tuuli MG, Norman SM, Odibo AO, Macones GA, Cahill AG. Perinatal outcomes in women with subchorionic hematoma: a systematic review and meta-analysis. Obstet Gynecol. 117(5):1205-12. http://doi.org/bgqbhk.
18.Xiang L, Wei Z, Cao Y. Symptoms of an intrauterine hematoma associated with pregnancy complications: a systematic review. PLoS One. 2014;9(11):e111676. http://doi.org/bx53.
19.Chotigeat U, Kalayanaroojs S, Nisalak A. Vertical transmission of dengue infection in Thai infants: two case reports. J Med Assoc Thai. 2003;86 (Suppl 3):S628-32.
20.Haas T, Görlinger K, Grassetto A, Agostini V, Simioni P, Nardi G, et al. Thromboelastometry for guiding bleeding management of the critically ill patient: a systematic review of the literature. Minerva Anestesiol. 2014;80(12):1320-35.
21.Crochemore T, de Toledo Piza FM, Silva E, Corrêa TD. Thromboelastometry-guided hemostatic therapy: an efficacious approach to manage bleeding risk in acute fatty liver of pregnancy: a case report. J Med Case Rep. 2015;9:202. http://doi.org/bx54.
https://revistas.unal.edu.co/index.php/care/article/view/58952
Tromboelastografía para dirigir la terapia transfusional en dengue hemorrágico en una paciente embarazada hospitalizada en UCI: Reporte de caso
Palabras clave: Dengue hemorrágico; Tromboelastografía; Embarazo.
Keywords: Severe Dengue; Thrombelastography; Pregnancy.
José A. Rojas, MD
Daniel Molano-Franco, MD
Tito Jiménez, MD
Albert Valencia, MD
Rafael Leal, MD
Pablo Méndez, MD
Victor Nieto, MD
Diego Hernández, MD
Unidad de Cuidados Intensivos
– Clínica Universitaria Colombia –
Grupo de investigación en Medicina Crítica
– Fundación Universitaria Sanitas –
Bogotá, D.C. – Colombia
Correspondencia:
Grupo de Investigación en Medicina Crítica.
dalemofra@gmail.com. Clínica Universitaria Colombia Calle 22b #66-46, 3er piso, Unidad de cuidado intensivo. Bogotá D.C. – Colombia
resumen
El dengue es una enfermedad considerada como el mayor problema de salud pública en países tropicales. Un importante porcentaje de pacientes que lo padecen requieren ingreso a la unidad de cuidados intensivos (UCI) debido a la severidad del cuadro clínico. El presente caso reporta la evolución clínica de una gestante de ocho semanas con cuadro febril asociado a trombocitopenia y leucopenia. La paciente procede de un área endémica para enfermedades tropicales, lo que lleva a realizar un diagnóstico de dengue con características hemorrágicas.
En la UCI, la paciente presenta hemorragia del primer trimestre y hematoma placentario, por lo que, ante el estado de embarazo y el riesgo de pérdida del mismo, se decide monitorizar la función hematológica con tromboelastrografía y transfundir hemoderivados según los hallazgos específicos. Se logra controlar y revertir el proceso de sangrado obstétrico con evolución favorable de la paciente y egreso de UCI. En el presente artículo se reporta la utilidad de la monitorización dinámica de la función hematológica con tromboelastografia en pacientes con dengue hemorrágico y condiciones especiales, tales como el embarazo.
Introducción
El dengue es una enfermedad tropical, caracterizada por fiebre y hemorragia, causada por el arbovirus dengue, genero flavivirus (transmitido por artrópodos), el cual es transmitido por la picadura de mosquitos del genero Aedes aegypti, especie con una amplia distribución en territorios inferiores a 1800 m s n m. Según datos de la Organización Mundial de la Salud (OMS) el dengue es el mayor problema de salud pública en países tropicales y subtropicales, siendo la causa de más de 500 000 hospitalizaciones por año, con una mortalidad de 1% (1).
Para 2012, en Colombia se reportaron 54 726 casos de dengue, de los cuales 1 641 corresponden a dengue grave y 25 174, a pacientes menores de 15 años, con una letalidad del 3.9%, lo que sitúa al país como territorio endémico para dengue en los últimos años (2). Ahora bien, no existen datos claros sobre su incidencia en población obstétrica; sin embargo, se ha reportado una condición de susceptibilidad para el desarrollo de infecciones con aumento en la severidad de las mismas. Además, hay evidencia creciente de la predisposición al desarrollo de cuadros de activación y respuesta inmune severa especialmente en casos de infecciones por Plasmodium falciparum y Listeria monocytogenes y cuadros virales como influenza AH1N1 (3).
Recientemente se han implementado técnicas para direccionar la terapia transfusional en pacientes con enfermedades críticas, como la tromboelastografía, que avalúa las diferentes fases de la coagulación y lisis del coágulo. La reducción en la morbimortalidad y el costo asociado a la atención en salud, producto de la disminución en el número de transfusiones, se han descrito como las principales ventajas en su uso (4). Aunque existen reportes que evidencian la utilidad de la tromboelastografia en sepsis (5), hasta el momento se desconoce su aplicabilidad clínica en pacientes con infección por dengue y complicaciones hemorrágicas que requieran administración de hemoderivados.
Teniendo en cuenta lo anterior, se presenta el caso de una paciente embarazada con dengue hemorrágico, tratada en un hospital universitario de Colombia, a la que se le aplicó terapia transfusional mediante la utilización seriada de tromboelastografía con el de fin controlar el sangrado obstétrico y evitar la pérdida de la gestación.
Presentación del caso
Información del paciente
Mujer de 33 años de edad, embarazada, natural y procedente de Bogotá D.C. y dedicada a labores domésticas.
Hallazgos clínicos
Mujer de 33 años, sin antecedentes médico-quirurgicos previos, quien cursa su segunda gestación, con ocho semanas de embarazo para el momento en el que acude a hospital. La paciente ingresa al servicio de urgencias por un cuadro clínico de cinco días de evolución de fiebre intermitente, de 38.3°C en repetidas ocasiones, asociado a escalofríos, mialgias generalizadas, dolor osteomuscular, reto-ocular y cefalea, además de nauseas, astenia, adinamia y dolor abdominal.
Niega antecedentes de trauma o infecciones vaginales o del tracto urinario. Igualmente, informa que para el momento de la consulta se encontraba en controles prenatales sin ningún hallazgo anormal. Como evento importante asociado comenta que siete días antes a la consulta viajó a región endémica para múltiples enfermedades tropicales, pues está ubicada a una altitud de 300 m s nivel mar. Al preguntársele de nuevo, manifiesta haber recibido múltiples picaduras por insecto en el destino de su viaje.
Calendario y evaluación diagnóstica
Con base en los hallazgos clínicos se hizo una sospecha de infección por virus de dengue y se solicitaron paraclínicos de ingreso (ver Tabla 1). El examen físico de ingreso no evidenció lesiones asociadas a fenómenos hemorrágicos como son equimosis, petequias o hematomas. El único hallazgo anormal al examen físico se dio durante la estancia en la unidad de urgencias, donde la paciente presentó un episodio de sangrado genital agudo, escaso y rutilante. Se omitió realizar tacto vaginal y se optó por hacer ecografía obstétrica, la cual confirmó viabilidad fetal con presencia de un hematoma retroplacentario de aproximadamente 50%, lo que permitió hacer un diagnóstico de amenaza de aborto; ante el riesgo de complicación hemorrágica, la paciente fue trasladada a la UCI, donde se confirmó el diagnóstico de infección por dengue a través de la identificación de IgG e IgM positivos para dengue.
Tabla 1. Hemograma y química sanguínea desde el ingreso hasta el día cinco.
|
Leucocitos c/mm3 |
Neutrófilos c/mm3 |
Rto plaquetas c/mm3 |
Hgb/dl |
Hcto (%) |
AST (U/L) |
ALT (U/L) |
BT (mg/dl) |
BD (mg/dl) |
PT (seg) |
PTT (seg) |
LDH (mg/dl) |
|
|
Día 1 |
2500 |
1800 |
117000 |
13.6 |
41 |
-- |
-- |
-- |
-- |
-- |
-- |
-- |
|
Día 2 |
3250 |
1340 |
45000 |
14 |
41 |
1022 |
1172 |
0.29 |
0.15 |
11 (Ct 10) |
46 (Ct 26) |
1118 |
|
Día 3 (hora 0) |
3000 |
1250 |
30000 |
14 |
42 |
919 |
954 |
-- |
-- |
11 (Ct 10) |
46 (Ct 28) |
-- |
|
Día 3 (hora 6)* |
-- |
-- |
20700 |
14.2 |
42 |
-- |
-- |
-- |
-- |
-- |
-- |
-- |
|
Día 4 |
4250 |
2300 |
42000 |
13 |
43 |
382 |
457 |
0.5 |
0.29 |
11 (Ct 10) |
28 (Ct 26) |
320 |
|
Día 5 |
5300 |
2700 |
65000 |
13 |
40 |
-- |
-- |
-- |
-- |
-- |
-- |
-- |
|
AST: Aspartato transferasa; ALT: Alanino transferasa; BT: Bilirrubina Total; BD: Bilirrubina Directa; c: células; Ct: Control; LDH: Lactato Deshidrogenasa; PT: Tiempo de Protrombina; PTT: Tiempo Parcial de Tromboplastina; Rto: Recuento; Hgb: hemoglobina, Hcto: hematocrito; PT: tiempo protrombina; PTT: tiempo de tromboplastina; LDH: deshidrogenasa láctica. |
||||||||||||
Fuente: elaboración propia a partir de los datos obtenidos en el estudio.
Durante la vigilancia en cuidado intensivo permanece hemodinámicamente estable, aunque con sangrado vaginal escaso y persistente, sin compromiso en la función respiratoria, renal o neurológica.
Intervención terapéutica
Al tercer día de hospitalización y ante el descenso abrupto del recuento plaquetario, se decidió realizar transfusión de plaquetas y solicitar tromboelastograma (TbEg) para determinar el estado de coagulación. Se reportó TbEg con R: 12.5, K: 13.0, ángulo DEG: 20.4, MA: 27.2 (Figura 1 A). Por su parte, un hemograma de control tomado seis horas después de la transfusión de plaquetas arrojó los siguientes resultados: Hg: 14.4g/dL, Hcto: 42.3%, N: 50%, L: 40.1%, conteo de plaquetas: 20 700cel/mm3. Teniendo en cuenta el riesgo de aborto por persistencia del sangrado vaginal, se optó de nuevo por transfundir hemoderivados, esta vez con plaquetas y plasma fresco congelado (PFC), e iniciar administración de fitomenadiona 10mg intravenosa (IV). Los tromboelastogramas de control solicitados durante las siguientes 24 horas se muestran en la (Figura 1 B, C y D ).
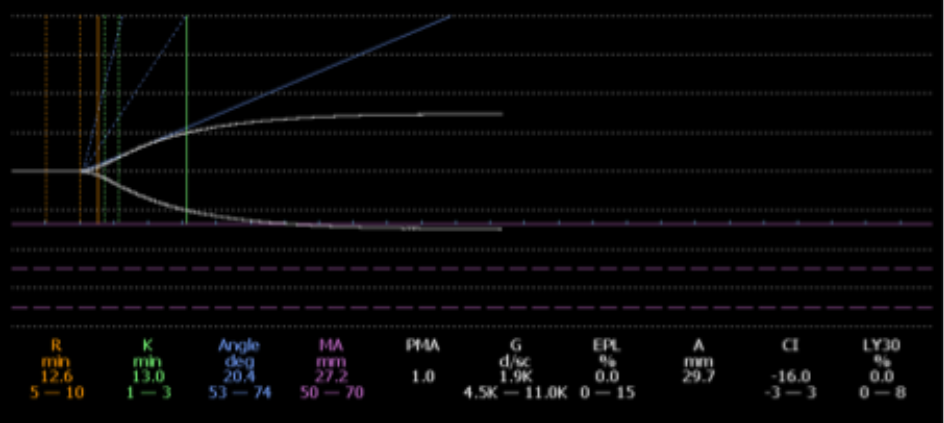
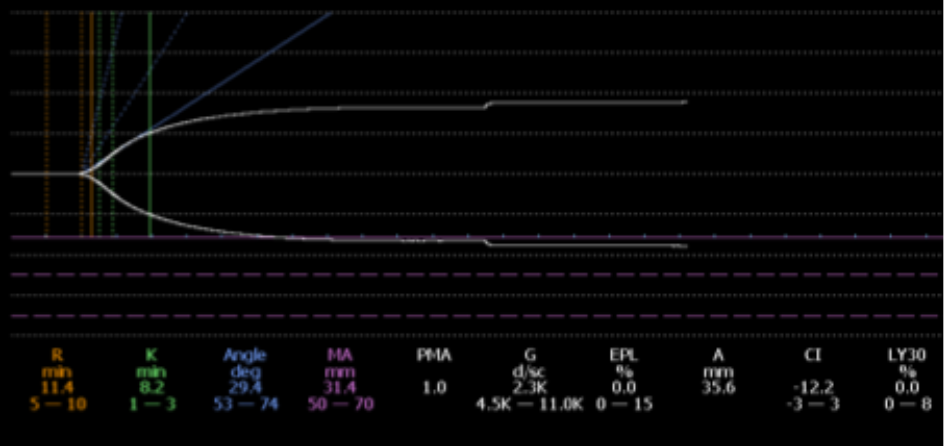
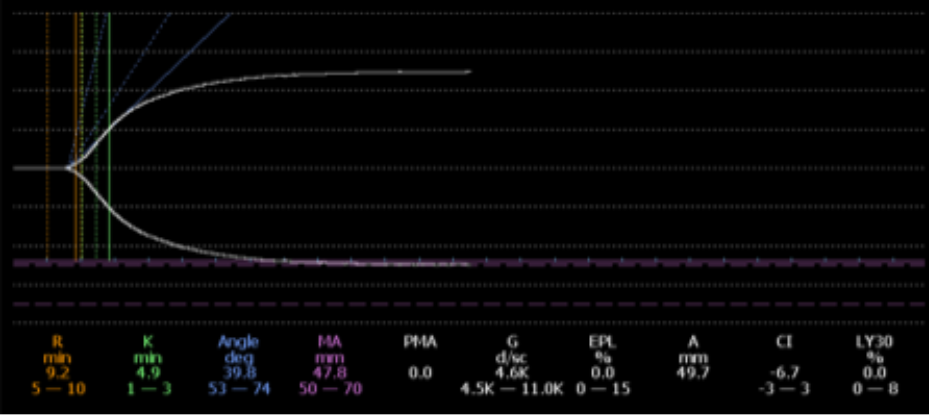
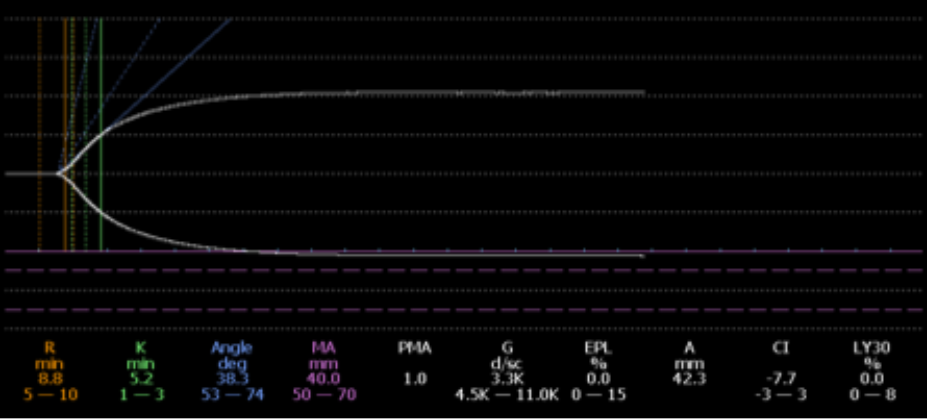
Figura 1. A. Tromboelastograma inicial con patrón de anticoagulación y deficiencia de factores de coagulación (tiempo k prolongado, ángulo alfa disminuido, amplitud máxima disminuida).
Figura 1. B. Tromboelastograma (TbEg) # 1 de control posterior a transfusión de plaquetas y 10U de PFC (corrección gradual en valores de tiempo K, ángulo alfa, amplitud máxima).
Figura 1. C. TbEg # 2 control posterior a segunda transfusión de concentrado de Plaquetas.
Figura 1. D. TbEg # 3 control posterior a transfusión de PFC (corrección de tiempo K, ángulo alfa,amplitud máxima, cercano a valores de referencia).
Fuente: Elaboración propia.
Seguimiento y evolución
Durante su estancia en la UCI se reportó un antígeno sérico de dengue positivo tipo IgM e IgG. Por su parte, la paciente tuvo evolución satisfactoria, sin presentar nuevos episodios de sangrado. Al sexto día de evolución de la enfermedad y con TbEg con corrección de las fases la paciente fue retirada de la UCI sin complicaciones, con seguimiento multidisciplinario por servicios hospitalarios de obstetricia, infectología y psicología. A los siete días de egreso se realizó ecografía obstétrica de control en la cual se observó que persistía hematoma retroplacentario, pero con una disminución en el 50% del tamaño original, continuando con viabilidad fetal.
Discusión
La presentación clínica del dengue es muy amplia y depende de las fases de la enfermedad, variando desde casos asintomáticos o con febrículas en la fase febril (0-3 días), hasta casos severos de hemorragias, estados de choque o disfunción orgánica en la fase crítica (3-6 días) y posterior resolución de los síntomas en la fase convaleciente (>6 días). En años recientes, se realizó una clasificación de esta enfermedad de acuerdo a su presentación clínica con el fin de identificar a tiempo los casos severos y guiar su tratamiento; esta clasificación se basa en la presencia o ausencia de signos de alarma y los estados de dengue grave, caracterizados por choque, hemorragias o compromiso orgánico como miocarditis, hepatitis, encefalitis, insuficiencia renal (6).
Los riesgos de presentar cuadros de dengue hemorrágico en el embarazo se determinan por el trimestre en el cual se contraiga, incluyendo hemorragia vaginal, amenaza de aborto y cuadros de abruptio placentae; al respecto, Carles et al. (7) determinaron una frecuencia aumentada de parto pretérmino del 55% en la Guyana francesa, datos similares a los reportados por Poli et al. (8). Por su parte, Restrepo et al. (9) reportaron un aumento en la incidencia de amenaza de aborto y parto pretérmino en pacientes con dengue hemorrágico en Colombia.
Un estudio más reciente reporta la presencia de eventos hemorrágicos asociados a la infección materna por dengue, en el 10% de los casos, remarcando que en el primer trimestre hay asociación a hematoma retroplacentario (10). Se ha recopilado evidencia que sugiere que no existe relación entre los casos de dengue y la presencia de malformaciones congénitas durante el primer trimestre del embarazo. Sin embargo en la India, Sharma & Gulati (11) reportan algunos casos de defectos en el tubo neural posteriores a una epidemia regional de dengue, sin que se lograran encontrar defectos cromosómicos asociados (11).
La mayoría de los individuos que adquieren la infección y desarrollan la enfermedad, evolucionan hacia dengue clásico, enfermedad febril autolimitada que usualmente no presenta complicaciones. Sin embargo, una proporción variable de pacientes desarrolla hemorragias espontáneas, disminución del recuento de plaquetas y signos de extravasación del plasma. El conjunto de estas manifestaciones define el síndrome de dengue hemorrágico
En varios estudios se han reportado manifestaciones hemorrágicas entre el 35 a 50%, siendo las más comunes epistaxis, gingivorragia y sagrado gastrointestinal (12-13). A pesar de este comportamiento, algunos autores, como Chaudhary et al. (14), consideran que no hay asociación entre las manifestaciones hemorrágicas y el conteo plaquetario, aunque, debido a la heterogenicidad en la selección de los pacientes, esta afirmación no se ha podido confirmar. Finalmente, en poblaciones especiales como niños y embarazadas, es posible que la trombocitopenia profunda esté fuertemente relacionada con la severidad del dengue, estimada esta última en términos de hemorragias (mayores y menores) y signos de extravasación plasmática.
Es precisamente en este grupo de pacientes donde existe discusión sobre realizar transfusiones, especialmente de plaquetas. Hasta el momento no hay datos que con certeza asocien aborto a infección por dengue en el primer trimestre; no obstante lo anterior, sí hay una asociación entre la presencia de un hematoma placentario y el riesgo de aborto, llegando a reportes del 5 al 17% de pérdidas en pacientes con hematomas, con un OR de 2.18 (1.20-3.67) (15-17).
Si bien existen múltiples causas etiológicas de hematomas retroplacentarios, incluyendo malformaciones fetales, insuficiencia de cuerpo lúteo, trauma e infecciones perinatales como parvovirus y toxoplamosis, también se han reportado en infecciones adquiridas a nivel uterino y sistémico (18). Al considerar el caso aquí presentado, es posible afirmar que el hematoma placentario estuvo asociado a una infección de tipo viral sistémico y se agravó por la presencia de disfunción hematológica con trombocitopenia severa.
En este contexto, y conociendo el riesgo de aborto, no existe un protocolo que determine si la corrección o no de la coagulopatía mejora el pronóstico obstétrico y disminuye el riesgo de aborto. Basurko et al. (10), en su serie de 53 pacientes, reportan dos casos de aborto temprano por sangrado utero-vaginal y cinco complicaciones hemorrágicas en el momento del parto. En otro estudio, Chotigeat et al. (19) compararon pacientes a las que se les transfundió plaquetas antes del parto con aquellas a las que no se les transfundió, encontrando una reducción de eventos hemorrágicos asociados en el primer grupo.
La disfunción hematológica observada en el estudio de tromboelastografia, considerando que este es un test que evalúa la hemostasia desde un punto de vista funcional representado por la interpretación del modelo celular de coagulación, y que su aplicación en diferentes escenarios clínicos, especialmente en pacientes de cirugía cardiovascular y en pacientes de trauma, representa una opción indicada para corregir las alteraciones hematológicas agudas y disminuir el uso innecesario de hemoderivados (20). Es importante enfatizar que las pruebas de coagulación convencionales no permiten abordar el trastorno de coagulación subyacente, lo que con frecuencia resulta en un reemplazo innecesario de los componentes de la sangre. Así, el análisis de tromboelastografía permite a los médicos reconocer la presencia de coagulopatía y, lo que es más importante, comprender el trastorno de coagulación subyacente (20).
En el presente caso la alteración en la máxima amplitud fue determinada mediante tromboelastografía, con lo que fue posible realizar la transfusión de plaquetas hasta corregir esta variable y asegurar una adecuada funcionalidad plaquetaria, lo que permitió solventar el sangrado vaginal. Si bien es discutible determinar si esta conducta resultó benéfica para la paciente o si la terminación del sangrado vaginal y reabsorción del hematoma se hubiera podido lograr tan solo a través de reposo y manejo médico de los síntomas de la infección viral, el presente reporte plantea la posibilidad de incluir esta conducta en el ejercicio médico.
No existen registros en la literatura que evalúen el rendimiento y utilidad de la tromboelastografía como un test dinámico para definir la corrección de la coagulopatía y, específicamente, la trombocitopenia en pacientes con dengue hemorrágico, así como tampoco en pacientes embarazadas con dengue. Se están reportando casos de uso en otras condiciones obstétricas, como hígado grado agudo del embarazo (21), un motivo más para considerar de relevancia este reporte.
Ahora bien, los autores también aceptan que el caso aquí reportado presenta debilidades, pues en el mismo no se determinaron otras causas de hematoma placentario, por ejemplo malformaciones fetales, pero, debido a la edad gestacional de la paciente y el curso agudo de la enfermedad, se optó por el manejo clínico descrito.
Conclusión
En pacientes con hematoma retroplacentario e infección por dengue asociada a trombocitopenia severa existe un riesgo aumentado de aborto y pérdida fetal. La corrección de la coagulopatía puede mejorar el pronóstico del embarazo. Las pruebas convencionales de coagulación pueden subvalorar el riesgo de coagulopatía y de aumento del sangrado secundario al hematoma. La tromboelastografía puede ser una herramienta útil en lo que refiere a identificar pacientes con alto riesgo de sangrado debido a trombocitopenia severa en casos de dengue durante el embarazo, por lo que su uso en instituciones donde se cuente con esta tecnología debe ser considerado.
Conflicto de intereses
Ninguno declarado por los autores.
Financiación
Ninguna declarada por los autores.
Referencias
1.World Health Organization. Dengue Haemorrhagic Fever: early recognition, diagnosis and hospital management. An audiovisual guide for health-care workers responding to outbreaks. WHO; 2006 [cited Feb 02 2017]. Available from: https://goo.gl/Mv8kph.
2.Ministerio de Salud y Protección Social. Circular 8. Instrucciones para la intensificación de las acciones de vigilancia, prevención, atención y control del dengue y dengue grave en Colombia. Bogota, D.C.: MinSalud;2013.
3.Kourtis AP, Read JS, Jamieson DJ. Pregnancy and infection. N Engl J Med. 2014;370(23):2211-18. http://doi.org/bx5c.
4.Levi M, Hunt BJ. A critical appraisal of point-of-care coagulation testing in critically ill patients. J Thromb Haemost. 2015;13(11):1960-7. http://doi.org/bx5d.
5.Zhong S, Zhang C, Hu J, Tang Z. Evaluation of coagulation disorders with thrombelastography in patients with sepsis. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2016;28(2):153-8. 10.3760/cma.j.issn.2095-4352.2016.02.013.
6.Ministerio de la Protección Social, Instituto Nacional de Salud, Organización Panamericana de la Salud.. Guía para la atención clínica integral del paciente con dengue. Bogotá: MinSalud;2010 [cited Feb 02 2017]. Available from: https://goo.gl/0niJbQ.
7.Carles G, Peiffer H, Talarmin A. Effects of dengue fever during pregnancy in French Guiana. Clin Infect Dis. 1999;28(3):637-40. http://doi.org/cg8wdr.
8.Poli L, Chungue E, Soulignac O, Gestas P, Kuo P, Papouin-Rauzy M. Materno-Fetal Dengue. Apropos o 5 cases observed during the epidemics in Tahiti (1989). Bull Soc Pathol Exot. 1991;84(5 Pt 5):513-21.
9.Restrepo BN, Isaza DM, Salazar CL, Ramírez JL, Upegui GE, Ospina M, et al. Efectos por la infección del virus del dengue sobre el feto y el recién nacido. Biomedica. 2003;23(4):416-23. http://doi.org/bx5v.
10.Basurko C, Carles G, Youssef M, Guindi W. Maternal and Fetal consequences of dengue fever during pregnancy. Eur J Obstet Gynecol Reprod Biol. 2009;147 (1):29-32. http://doi.org/dvg8hq.
11.Sharma JB, Gulati N. Potential relationship between dengue fever and neural tube defects in a northern district on India. Int J Gynaecol Obstet. 1992;39(4):291-5. http://doi.org/bwzcmf.
12.Makroo RN, Raina V, Kumar P, Kanth RK. Role of platelet transfusion in the management of dengue patients in a tertiary care hospital. Asian J Tranfus Sci. 2007;1(1):4-7. http://doi.org/b7bkqg.
13.Chairulfatah A, Setiabudi D, Agoes R, Colebunder R. Thrombocytopenia and platelet transfusion in dengue haemorrhagic fever and dengue shock syndrome. WHO Dengue bulletin. 2003;27: 141-3
14.Chaudhary R, Khetan D, Sinha S, Sinha P, Sonker A, Pandey P, et al. Transfusion support to dengue patients in a hospital based blood transfusion service in north India. Transfus Apheric Sci. 2006;35(3):239-44. http://doi.org/cz5m85.
15. Şükür YE, Göç G, Köse O, Açmaz G, Özmen B, Atabekoğlu CS, et al. The effects of subchorionic hematoma on pregnancy outcome in patients with threatened abortion. J Turk Ger Gynecol Assoc. 2014;15(4):239-42. http://doi.org/bx5z.
16.Soldo V, Cutura N, Zamurovic M. Threatened miscarriage in the first trimester and retrochorial hematomas: sonographic evaluation and significance. Clin Exp Obstet Gynecol. 2013;40(4): 548-50.
17.Tuuli MG, Norman SM, Odibo AO, Macones GA, Cahill AG. Perinatal outcomes in women with subchorionic hematoma: a systematic review and meta-analysis. Obstet Gynecol. 117(5):1205-12. http://doi.org/bgqbhk.
18.Xiang L, Wei Z, Cao Y. Symptoms of an intrauterine hematoma associated with pregnancy complications: a systematic review. PLoS One. 2014;9(11):e111676. http://doi.org/bx53.
19.Chotigeat U, Kalayanaroojs S, Nisalak A. Vertical transmission of dengue infection in Thai infants: two case reports. J Med Assoc Thai. 2003;86 (Suppl 3):S628-32.
20.Haas T, Görlinger K, Grassetto A, Agostini V, Simioni P, Nardi G, et al. Thromboelastometry for guiding bleeding management of the critically ill patient: a systematic review of the literature. Minerva Anestesiol. 2014;80(12):1320-35.
21.Crochemore T, de Toledo Piza FM, Silva E, Corrêa TD. Thromboelastometry-guided hemostatic therapy: an efficacious approach to manage bleeding risk in acute fatty liver of pregnancy: a case report. J Med Case Rep. 2015;9:202. http://doi.org/bx54.
Referencias
World Health Organization. Dengue Haemorrhagic Fever: early recognition, diagnosis and hospital management. An audiovisual guide for health-care workers responding to outbreaks. WHO; 2006 [cited Feb 02 2017]. Available from: https://goo.gl/Mv8kph
Ministerio de Salud y Protección Social. Circular 8. Instrucciones para la intensificación de las acciones de vigilancia, prevención, atención y control del dengue y dengue grave en Colombia. Bogota, D.C.: MinSalud;2013
Kourtis AP, Read JS, Jamieson DJ. Pregnancy and infection. N Engl J Med. 2014;370(23):2211-18. http://doi.org/bx5c
Levi M, Hunt BJ. A critical appraisal of point-of-care coagulation testing in critically ill patients. J Thromb Haemost. 2015;13(11):1960-7. http://doi.org/bx5d
Zhong S, Zhang C, Hu J, Tang Z. Evaluation of coagulation disorders with thrombelastography in patients with sepsis. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2016;28(2):153-8. 10.3760/cma.j.issn.2095-4352.2016.02.013
Ministerio de la Protección Social, Instituto Nacional de Salud, Organización Panamericana de la Salud.. Guía para la atención clínica integral del paciente con dengue. Bogotá: MinSalud;2010 [cited Feb 02 2017]. Available from: https://goo.gl/0niJbQ
Carles G, Peiffer H, Talarmin A. Effects of dengue fever during pregnancy in French Guiana. Clin Infect Dis. 1999;28(3):637-40. http://doi.org/cg8wdr
Poli L, Chungue E, Soulignac O, Gestas P, Kuo P, Papouin-Rauzy M. Materno-Fetal Dengue. Apropos o 5 cases observed during the epidemics in Tahiti (1989). Bull Soc Pathol Exot. 1991;84(5 Pt 5):513-21
Restrepo BN, Isaza DM, Salazar CL, Ramírez JL, Upegui GE, Ospina M, et al. Efectos por la infección del virus del dengue sobre el feto y el recién nacido. Biomedica. 2003;23(4):416-23. http://doi.org/bx5v
Basurko C, Carles G, Youssef M, Guindi W. Maternal and Fetal consequences of dengue fever during pregnancy. Eur J Obstet Gynecol Reprod Biol. 2009;147 (1):29-32. http://doi.org/dvg8hq
Sharma JB, Gulati N. Potential relationship between dengue fever and neural tube defects in a northern district on India. Int J Gynaecol Obstet. 1992;39(4):291-5. http://doi.org/bwzcmf
Makroo RN, Raina V, Kumar P, Kanth RK. Role of platelet transfusion in the management of dengue patients in a tertiary care hospital. Asian J Tranfus Sci. 2007;1(1):4-7. http://doi.org/b7bkqg
Chairulfatah A, Setiabudi D, Agoes R, Colebunder R. Thrombocytopenia and platelet transfusion in dengue haemorrhagic fever and dengue shock syndrome. WHO Dengue bulletin. 2003;27: 141-3
Chaudhary R, Khetan D, Sinha S, Sinha P, Sonker A, Pandey P, et al. Transfusion support to dengue patients in a hospital based blood transfusion service in north India. Transfus Apheric Sci. 2006;35(3):239-44. http://doi.org/cz5m85
Şükür YE, Göç G, Köse O, Açmaz G, Özmen B, Atabekoğlu CS, et al. The effects of subchorionic hematoma on pregnancy outcome in patients with threatened abortion. J Turk Ger Gynecol Assoc. 2014;15(4):239-42. http://doi.org/bx5z
Soldo V, Cutura N, Zamurovic M. Threatened miscarriage in the first trimester and retrochorial hematomas: sonographic evaluation and significance. Clin Exp Obstet Gynecol. 2013;40(4): 548-50
Tuuli MG, Norman SM, Odibo AO, Macones GA, Cahill AG. Perinatal outcomes in women with subchorionic hematoma: a systematic review and meta-analysis. Obstet Gynecol. 117(5):1205-12. http://doi.org/bgqbhk
Xiang L, Wei Z, Cao Y. Symptoms of an intrauterine hematoma associated with pregnancy complications: a systematic review. PLoS One. 2014;9(11):e111676. http://doi.org/bx53
Chotigeat U, Kalayanaroojs S, Nisalak A. Vertical transmission of dengue infection in Thai infants: two case reports. J Med Assoc Thai. 2003;86 (Suppl 3):S628-32
Haas T, Görlinger K, Grassetto A, Agostini V, Simioni P, Nardi G, et al. Thromboelastometry for guiding bleeding management of the critically ill patient: a systematic review of the literature. Minerva Anestesiol. 2014;80(12):1320-35
Crochemore T, de Toledo Piza FM, Silva E, Corrêa TD. Thromboelastometry-guided hemostatic therapy: an efficacious approach to manage bleeding risk in acute fatty liver of pregnancy: a case report. J Med Case Rep. 2015;9:202.http://doi.org/bx54
Cómo citar
APA
ACM
ACS
ABNT
Chicago
Harvard
IEEE
MLA
Turabian
Vancouver
Descargar cita
Licencia
Derechos de autor 2017 Case reports

Esta obra está bajo una licencia internacional Creative Commons Atribución 4.0.
Los autores al someter sus manuscritos conservarán sus derechos de autor. La revista tiene el derecho del uso, reproducción, transmisión, distribución y publicación en cualquier forma o medio.
El Formulario de Divulgación Uniforme para posibles Conflictos de Interés y los oficios de cesión de derechos y de responsabilidad deben ser entregados junto con el original.
Aquellos autores/as que tengan publicaciones con esta revista, aceptan los términos siguientes:
Los autores/as conservarán sus derechos de autor y garantizarán a la revista el derecho de primera publicación de su obra, el cual estará simultáneamente sujeto a la Licencia de reconocimiento de Creative Commons 4.0 que permite a terceros compartir la obra siempre que se indique su autor y su primera publicación en esta revista.
Los autores/as podrán adoptar otros acuerdos de licencia no exclusiva de distribución de la versión de la obra publicada (p. ej.: depositarla en un archivo telemático institucional o publicarla en un volumen monográfico) siempre que se indique la publicación inicial en esta revista.
Se permite y recomienda a los autores/as difundir su obra a través de Internet (p. ej.: en archivos telemáticos institucionales o en su página web) antes y durante el proceso de envío, lo cual puede producir intercambios interesantes y aumentar las citas de la obra publicada. (Véase El efecto del acceso abierto).























