


Publicado
Infected pulmonary infarction. Case report
Infarto pulmonar infectado. Reporte de caso
DOI:
https://doi.org/10.15446/cr.v3n1.60484Palabras clave:
Pulmonary infarction, Pulmonary embolism, Anticoagulation (en)Infarto pulmonar, Embolismo pulmonar, Anticoagulación (es)
Introduction. Pulmonary infarction occurs in 29% to 32% of patients with pulmonary thromboembolism (PTE). The infection of a pulmonary infarction is a complication in approximately 2 to 7% of the cases, which makes it a rare entity.
Case description. 49-year-old woman with pleuritic pain in the left hemithorax that irradiated to the dorsal region, associated with dyspnea and painful edema in the left lower limb of two days of evolution. Two weeks prior to admission, the patient suffered from a left knee trauma that required surgical intervention; however, due to unknown reasons, she did not receive antithrombotic prophylaxis. Physical examination showed tachycardia, tachypnea and painful edema with erythema in the left leg. After suspecting a pulmonary thromboembolism, anticoagulation medication was administered and a chest angiotomography was requested to confirm the diagnosis.
The patient experienced signs of systemic inflammatory response, and respiratory deterioration. A control tomography was performed, suggesting infected pulmonary infarction. Antibiotic treatment was initiated, obtaining progressive improvement; the patient was subsequently discharged, and continued with anticoagulation medication and follow-up on an outpatient basis.
Conclusions. Pulmonary infarction is a frequent complication in patients with PTE. Therefore, infected pulmonary infarction should be suspected in patients with clinical deterioration and systemic inflammatory response. The radiological difference between pulmonary infarction and pneumonia is not easily identified, thus the diagnostic approach is clinical, and anticoagulant and antimicrobial treatment should be initiated in a timely manner.
Introducción: el infarto pulmonar ocurre entre un 29 y un 32% de pacientes con tromboembolismo pulmonar (TEP). Por su parte, la infección de un infarto pulmonar complica aproximadamente del 2 al 7% de los casos, lo que hace que el infarto pulmonar infectado sea una entidad poco frecuente.
Descripción del caso: mujer de 49 años con dolor pleurítico en hemitórax izquierdo, irradiado a región dorsal, asociado a disnea y edema doloroso de miembro inferior izquierdo de dos días de evolución. Dos semanas antes de su ingreso la paciente sufrió trauma de rodilla izquierda, el cual que requirió intervención quirúrgica; sin embargo, por motivos desconocidos, no recibió profilaxis anti trombótica. En el examen físico se encontró taquicardia, taquipnea y edema doloroso con eritema en pierna izquierda. Al existir alta sospecha de tromboembolia pulmonar se inició anticoagulación y se solicitó angiotomografía de tórax, con la cual fue posible confirmar el diagnóstico.
Durante su evolución, la paciente experimentó signos de respuesta inflamatoria sistémica, deterioro respiratorio. Se realizó tomografía de control sugestiva de infarto pulmonar infectado. Se inició antibiótico y la paciente mejoró de forma progresiva; después de esta mejora, fue dada de alta para continuar anticoagulación y seguimiento ambulatorios.
Conclusiones: el infarto pulmonar es una complicación frecuente en pacientes con TEP. Por lo tanto, debe sospecharse infarto pulmonar infectado en pacientes con deterioro clínico y respuesta inflamatoria sistémica. La diferencia radiológica entre infarto pulmonar y neumonía no es fácil de identificar, su enfoque diagnóstico es clínico y el tratamiento anticoagulante y antimicrobiano debe iniciarse de manera oportuna.
https://revistas.unal.edu.co/index.php/care/article/view/60484
Infected pulmonary infarction. Case report
Palabras clave: Infarto pulmonar; Embolismo pulmonar; Anticoagulación.
Keywords: Pulmonary infarction; Pulmonary embolism; Anticoagulation.
Laura Marcela Velásquez Gaviria, MD
Andrés Garcés Arias, MD
Sebastián Felipe Sierra Umaña, MD
Andrés Fernando Rodríguez Gutierrez, MD
Department of Internal Medicine
Faculty of Medicine
– Universidad Nacional de Colombia -–
Bogotá D.C. - Colombia
Cristian Alejandro Castillo Rodriguez
Luis David Sáenz Pérez
Laura Salazar Franco
Sebastian Salinas Mendoza
Medical Program
Faculty of Medicine
– Universidad Nacional de Colombia -–
Bogotá D.C. - Colombia
Diego Fernando López Donato, MD
Department of Radiology
Faculty of Medicine
– Universidad Nacional de Colombia -–
Bogotá D.C. - Colombia
Luisa Fernanda Patiño Unibio, MD
Department of Internal Medicine
Faculty of Medicine
– Pontificia Universidad Javeriana -–
Bogotá D.C. - Colombia
Corresponding author
Sebastián Felipe Sierra Umaña.
Universidad Nacional de Colombia
Facultad de Medicina, Departamento de Medicina Interna
– Sede Bogotá – Colombia.
Email: sfsierrau@unal.edu.co
ABSTRACT
Introduction: Pulmonary infarction occurs in 29% to 32% of patients with pulmonary thromboembolism (PTE). The infection of a pulmonary infarction is a complication in approximately 2 to 7% of the cases, which makes it a rare entity.
Case Presentation: 49-year-old woman with pleuritic pain in the left hemithorax that irradiated to the dorsal region, associated with dyspnea and painful edema in the left lower limb of two days of evolution. Two weeks prior to admission, the patient suffered from a left knee trauma that required surgical intervention; however, due to unknown reasons, she did not receive antithrombotic prophylaxis. Physical examination showed tachycardia, tachypnea and painful edema with erythema in the left leg. After suspecting a pulmonary thromboembolism, anticoagulation medication was administered and a chest angiotomography was requested to confirm the diagnosis.
The patient experienced signs of systemic inflammatory response, and respiratory deterioration. A control tomography was performed, suggesting infected pulmonary infarction. Antibiotic treatment was initiated, obtaining progressive improvement; the patient was subsequently discharged, and continued with anticoagulation medication and follow-up on an outpatient basis.
Conclusions: Pulmonary infarction is a frequent complication in patients with PTE. Therefore, infected pulmonary infarction should be suspected in patients with clinical deterioration and systemic inflammatory response. The radiological difference between pulmonary infarction and pneumonia is not easily identified, thus the diagnostic approach is clinical, and anticoagulant and antimicrobial treatment should be initiated in a timely manner.
IntroducTIOn
Pulmonary thromboembolism (PTE) is the third leading cause of death related to cardiovascular disease, in which acute right ventricular failure and pulmonary infarction are the main complications (1). Some studies have reported that pulmonary infarction occurs in 29% to 32% of patients with PTE (1-3).
Pulmonary infarction secondary to pulmonary embolism is more common in patients with low cardiopulmonary reserve (4). A study showed that pulmonary infarctions in patients with PTE occurred in 36% of congestive heart failure cases, and in 54% of patients with hypotension and shock (5). Nevertheless, more recent studies have indicated that young patients with good health status prior to PTE can have a higher incidence of pulmonary infarction (6,3). In addition, a high thrombotic burden has been associated with an increased probability of pulmonary infarction, although this is observed in small pulmonary arteries (7).
In general, pulmonary infarction causes pleuritic pain, tachypnea, dyspnoea and, in extremely rare cases, coughing with hemoptysis (8); therefore, radiological differentiation from other entities such as masses, atelectasis and pneumonia is difficult.
Pulmonary infarction is usually observed in subpleural regions and occurs predominantly in the lower lobes, especially the right lobe. The most common radiological finding is a triangular consolidation of the pulmonary parenchyma (50%), although segments with a ground glass pattern (35.9%) and Hampton sign (14.5%) can also be observed, which help to differentiate it from masses and pneumonia (6,9,10).
Multiple complications have been associated with pulmonary infarction, including pneumonia, pneumothorax, bronchopulmonary fistula, alveolar hemorrhage, cavitations, empyema and pulmonary abscess (11). Infection associated with pulmonary infarction is a rare but important complication, as it may result in the formation of abscesses and empyemas that may require surgical drainage.
The obstruction of a pulmonary vessel secondary to a sterile plunger is suggested to be the cause of blood extravasation into the surrounding tissues, of edema in adjacent bronchial walls, and of the increase of endobronchial secretion, which forms a favorable environment for colonization and bacterial infection by air or blood (12). Bashir & Benson (13), based on a series of postmortem studies, estimated the incidence of lung infarction infection in 2 to 7% (13). The presence of fever, sweating, tachycardia, purulent sputum, as well as of deterioration of the general condition and leukocytosis after pulmonary infarction, is highly suggestive of infection, which is why the spectrum of etiological agents is considered similar to that described in nosocomial pneumonia (11). In cases of infected pulmonary infarction, anticoagulant and antibiotic therapies should be initiated timely and selected according to local resistance patterns, associated pathogens, patient characteristics and clinical context in general (5).
This paper reports a case compatible with pulmonary thromboembolism complicated by infected pulmonary infarction.
Case presentation
49-year-old female, public accountant, from Bogotá, Colombia who consulted due to a two-day long clinical picture involving pleuritic pain in the left hemithorax, irradiated to the dorsal region, associated with sudden dyspnea, edema, and warm sensation on the lower left limb; no fever, coughing or hemoptysis were reported. Two weeks prior to consultation, the patient underwent meniscus reconstruction, and anterior and posterior cruciate ligament and left knee chondroplasty secondary to a closed trauma. No postoperative antithrombotic prophylaxis was performed after the procedure due to unknown reasons. The patient had an important history of class 1 obesity, with no previous pathological, toxic or allergic symptoms nor previous hospitalizations.
Physical examination on admission showed a normal general condition, with blood pressure of 97/63 mmHg, heart rate of 106 bpm, respiratory rate of 20 rpm, oxygen saturation at 96%, oxygen inspired fraction of 0.21, and axillary temperature of 36.5°C. Her height was 160 cm and weight 83 kg, which showed a body mass index (BMI) of 32.4 kg/m2. Thorax auscultation showed P2> A2 without murmurs; fine crackles were also identified in the base of the left lung. Edema in the foot and proximal third of the leg was found in the lower left limb, with local erythema and superficial pain on palpation.
The following tests were performed: blood count, electrolytes, blood urea nitrogen (BUN) and creatinine, which were within normal limits. On the other hand, the electrocardiogram showed sinus tachycardia, while the echocardiogram had a structural and functionally normal heart. Finally, the chest X-ray revealed left basal lamellar atelectasis and right atrium growth (Figure 1).
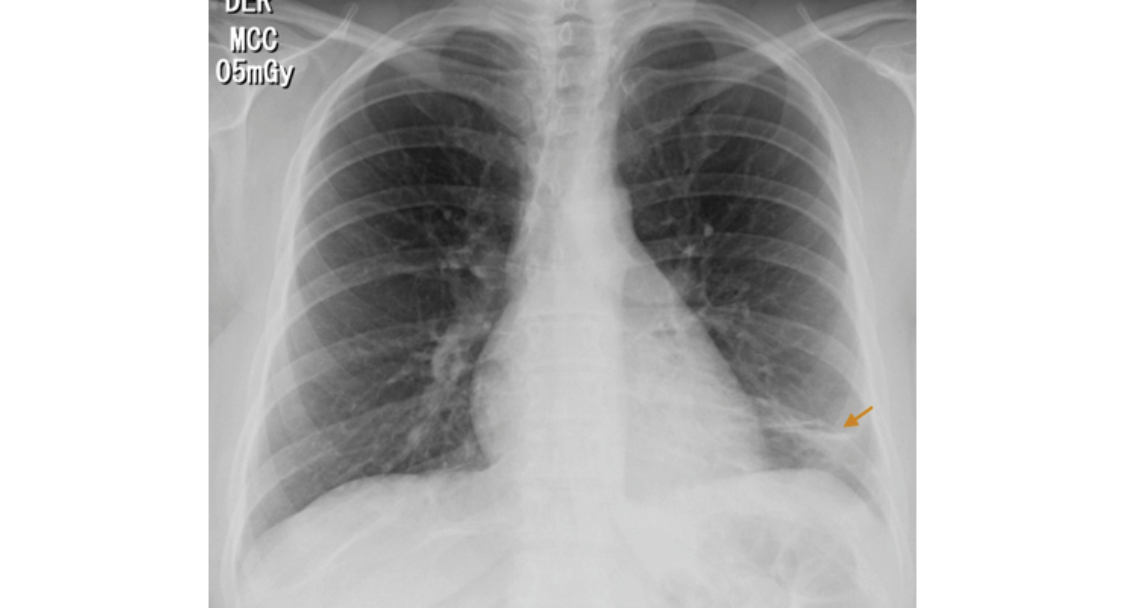
Fig 1. Posteroanterior chest X-ray. Image in left basal band corresponding to atelectasis (arrow).
Source: Own elaboration based on the data obtained in the study.
The Wells scale was applied, finding a high probability for pulmonary thromboembolism. Anticoagulation was initiated with low molecular weight heparin (enoxaparin) at a dose of 1 mg/kg every 12 hours, and a computed axial angiography (AngioCAT) of the chest was performed, confirming the diagnostic suspicion by reporting pulmonary artery obstruction in the trunk of the lower left basal segment (Figure 2).

Fig 2. Angiotomography of the chest. Axial plane. Pulmonary embolism, filling defect in the shape of a life preserver sign (arrow).
Source: Own elaboration based on the data obtained in the study.
Surprisingly, after initiating anticoagulation and other general treatment measures indicated for pulmonary thromboembolism, and about three days after her hospitalization, the patient required increased oxygen flow through nasal cannula, her chest pain worsened, and presented with dyspnea, fever, leukocytosis, tachycardia, and tachypnea. Control paraclinical exams were requested, revealing high C-reactive protein and a significant increase in leukocytes at neutrophils expense. A new chest tomographic evaluation was performed, in which wedge densities were identified in the middle and lower right lobes and in the lower left lobe, as well as an aerial bronchogram of the right lower lobe and bilateral pleural effusion (Figure 3 and 4). No blood cultures or sputum cultures were performed.

Fig 3. Angiotomography of the chest. Coronal plane. Pulmonary embolism, filling defect configuring the railway track sign (arrow), left basal consolidation of the pleural base and air bronchogram corresponding to pulmonary infarction (star).
Source: Own elaboration based on the data obtained in the study.

Fig 4. Chest AngioCAT. Broad base consolidation, hilar apex, obtuse borders that coincide with pulmonary infarction (star), pleural effusion (arrow).
Source: Own elaboration based on the data obtained in the study.

Fig 4. Timeline.
Source: Own elaboration based on the data obtained in the study.
With this in mind, infected pulmonary infarction was diagnosed and broad-spectrum antibiotic therapy with piperacillin + tazobactam was initiated at a dose of 4.5 g intravenously every six hours, considering that the infection was nosocomial and that the patient had undergone a recent hospitalization, thus increasing the risk of resistant germs.
The patient improved progressively, and oral anticoagulation with warfarin was initiated at a dose of 5 mg every 24 hours. After completing the seventh day of antibiotic treatment and with INR (International Normalized Ratio) within the therapeutic range, she was discharged with anticoagulation prescription for three months initially, and internal medicine outpatient controls. No adverse reactions to treatments during hospitalization were observed. Figure 4 shows the timeline of the reported case
Discussion
This case shows the clinical evolution of a patient with PTE, which progressed to pulmonary infarction and infection of the necrotic lung tissue. This case is relevant from several points of view, since it points the importance of thrombus prophylaxis in patients at risk, and exposes complications that endanger patients’ lives and generate diagnostic, therapeutic and research challenges.
Many risk factors are associated with pulmonary thromboembolism; in this case, the patient presented trauma, surgery, immobility and obesity (14). The incidence of PTE can be reduced by performing thrombus prophylaxis in patients undergoing orthopedic knee surgery, particularly in the presence of additional risk factors (15). Therefore, prophylaxis until patients recover mobility is highly recommended (16).
PTE diagnosis was obtained by following the guidelines for clinical practice (17), that is to say, by classifying the probabilities through Wells scale and confirming the diagnosis with the test of choice, in this case, chest AngioCAT.
On the other hand, the evolution of the patient’s clinical picture, besides the development of systemic inflammatory response, elevation of acute phase reactants, exacerbation of pleuritic pain and respiratory deterioration, caused the suspicion of infected pulmonary infarction (8). This clinical presentation, along with compatible diagnostic images, was the basis of the diagnosis. In this case, a significant improvement was achieved, allowing hospital discharge and a good short- and long-term prognosis.
Nevertheless, it is important to mention that this report has significant limitations: the lack of microbiological isolates to determine the etiological agent, the lack of clinical practice guidelines for the diagnosis and treatment of infected pulmonary infarction, and the radiological difficulty to differentiate bacterial pneumonia and pulmonary infarction (11). In addition, antibiotic treatment was selected based on the extrapolation of the local guidelines for the treatment of nosocomial pneumonia. Further research on the subject is necessary to better understand, diagnose, treat and prevent this entity, in order to improve care and clinical outcomes of patients.
In conclusion, pulmonary infarction is a common complication of pulmonary thromboembolism, which can become infected on rare occasions. Consequently, a high degree of clinical suspicion and adequate interpretation of the evolution are necessary to establish the diagnosis and to provide timely management.
Patient Perspective: the patient expressed gratitude for receiving medical care in an appropriate and humanized way.
Informed consent: the patient consented the publication of the information used in this case report.
Conflict of interest
None stated by the authors.
Funding
None stated by the authors.
References
1.Kirchner J, Obermann A, Stückradt S, Tüshaus C, Goltz J, Liermann D, et al. Lung Infarction Following Pulmonary Embolism: A Comparative Study on Clinical Conditions and CT Findings to Identify Predisposing Factors. Rofo. 2015;;187(6):440-4. http://doi.org/bx9z.
2.Gadkowski LB, Stout JE. Cavitary pulmonary disease. Clin Microbiol Rev. 2008;21(2):305-33, table of contents. http://doi.org/dq4kf8.
3.Miniati M, Bottai M, Ciccotosto C, Roberto L, Monti S. Predictors of Pulmonary Infarction. Medicine (Baltimore). 2015;94(41):e1488. http://doi.org/f3pjf5.
4.Morgenthaler TI, Ryu JH, Utz JP. Cavitary Pulmonary Infarct in Immunocompromised Hosts. Mayo Clin Proc. 1995;70(1):66-8. http://doi.org/dzxf35.
5.Hampton AO, Castleman B. Correlation of postmortem chest teleroentgenograms with autopsy findings with special reference to pulmonary embolism and infarction. AJR Am J Roentgenol. 1940;43:305-26.
6.Miniati M. Pulmonary Infarction: An Often Unrecognized Clinical Entity. Semin Thromb Hemost. 2016;42(8):865-9. http://doi.org/bx92.
7.Cha S-I, Shin K-M, Lee J, Hwangbo Y, Yoo S-S, Lee J, et al. Clinical relevance of pulmonary infarction in patients with pulmonary embolism. Thromb Res. 2012;130(3):e1-5. http://doi.org/bx93.
8.Stein PD, Henry JW. Clinical Characteristics of Patients With Acute Pulmonary Embolism Stratified According to Their Presenting Syndromes. Chest. 1997;112(4):974-9. http://doi.org/bkzg44.
9.Kuriakose J, Patel S. Acute Pulmonary Embolism. Radiol Clin N Am. 2010;48(1):31-50. http://doi.org/dgsj4k.
10.He H, Stein MW, Zalta B, Haramati LB. Pulmonary infarction: spectrum of findings on multidetector helical CT. J Thorac Imaging. 2006 Mar;21(1):1-7. http://doi.org/bj9n4b.
11.Djordjevic I, Pejcic T. Cavitary Pulmonary Infarct: The Differential Diagnostic Dilemma - A Case Report. In: Okuyan Erugrul (Ed.). Venous Thrombosis - Principles and Practice. InTech; 2012 http://doi.org/bx94.
12.Janes RM. Abscess of the Lung. Can Med Assoc J. 1942 [cited 2016 Jul 30];47(6):540-5. Available from: https://goo.gl/Hrn5Hj.
13.Bashir Y, Benson MK. Necrotising pneumonia and empyema due to Clostridium perfringens complicating pulmonary embolus. Thorax. 1990;45(1):72-3. http://doi.org/fqkc8t.
14.Steffen LM, Cushman M, Peacock JM, Heckbert SR, Jacobs DR Jr, Rosamond WD, et al. Metabolic syndrome and risk of venous thromboembolism: Longitudinal Investigation of Thromboembolism Etiology. J Thromb Haemost. 2009;7(5):746-51. http://doi.org/dqjbcx.
15.Kearon C. Natural History of Venous Thromboembolism. Circulation. 2003;107(23 suppl 1):I22-30.
16.National Institute for Health and Care Excellence (NICE). Venous thromboembolism: reducing the risk for patients in hospital. Londres: NICE; 2010 [cited 2016 Jul 30]. Clinical guideline [CG92]. Available from: https://goo.gl/wbRNc7.
17.Konstantinides S, Torbicki A, Agnelli G, Danchin N, Fitzmaurice D, Galiè N, et al. Guía de práctica clínica de la ESC 2014 sobre el diagnóstico y el tratamiento de la embolia pulmonar aguda. Rev Española Cardiol. 2015;68(1):64.e1-64.e45. http://doi.org/f2xz6j.
infarto pulmonar infectado. reporte de caso
Palabras clave: Infarto pulmonar; Embolismo pulmonar; Anticoagulación.
Sebastián Felipe Sierra Umaña
Andrés Garcés Arias
Fernando Rodríguez Gutierrez
Departamento de Medicina Interna
- Facultad de Medicina -
Universidad Nacional de Colombia
- Bogotá, D.C. - Colombia
Diego Fernando López Donato
Departamento de Radiología
- Facultad de Medicina -
Universidad Nacional de Colombia
- Bogotá, D.C. - Colombia
Luisa Fernanda Patiño Unibio
Departamento de Medicina Interna
- Facultad de Medicina -
Pontificia Universidad Javeriana
- Bogotá, D.C. - Colombia
Laura Salazar Franco
Sebastian Salinas Mendoza
Luis David Sáenz Pérez
Cristian Alejandro Castillo Rodriguez
Programa de Medicina
- Facultad de Medicina -
Universidad Nacional de Colombia
- Bogotá, D.C. - Colombia
Correspondencia
Sebastián Felipe Sierra Umaña
Correo electrónico: sfsierrau@unal.edu.co
RESUMEN
Introducción
El infarto pulmonar ocurre entre un 29 y un 32% de pacientes con tromboembolismo pulmonar (TEP). Por su parte, la infección de un infarto pulmonar complica aproximadamente del 2 al 7% de los casos, lo que hace que el infarto pulmonar infectado sea una entidad poco frecuente.
Descripción del caso
Mujer de 49 años con dolor pleurítico en hemitórax izquierdo, irradiado a región dorsal, asociado a disnea y edema doloroso de miembro inferior izquierdo de dos días de evolución. Dos semanas antes de su ingreso la paciente sufrió trauma de rodilla izquierda, el cual que requirió intervención quirúrgica; sin embargo, por motivos desconocidos, no recibió profilaxis anti trombótica. En el examen físico se encontró taquicardia, taquipnea y edema doloroso con eritema en pierna izquierda. Al existir alta sospecha de tromboembolia pulmonar se inició anticoagulación y se solicitó angiotomografía de tórax, con la cual fue posible confirmar
el diagnóstico.
Durante su evolución, la paciente experimentó signos de respuesta inflamatoria sistémica, deterioro respiratorio. Se realizó tomografía de control sugestiva de infarto pulmonar infectado. Se inició antibiótico y la paciente mejoró de forma progresiva; después de esta mejora, fue dada de alta para continuar anticoagulación y seguimiento ambulatorios.
Conclusiones
El infarto pulmonar es una complicación frecuente en pacientes con TEP. Por lo tanto, debe sospecharse infarto pulmonar infectado en pacientes con deterioro clínico y respuesta inflamatoria sistémica. La diferencia radiológica entre infarto pulmonar y neumonía no es fácil de identificar, su enfoque diagnóstico es clínico y el tratamiento anticoagulante y antimicrobiano debe iniciarse de manera oportuna.
INTRODUCCIÓN
El tromboembolismo pulmonar (TEP) es la tercera causa de muerte cardiovascular, siendo la falla cardíaca derecha aguda y el infarto pulmonar sus principales complicaciones (1). Algunos estudios han reportado que el infarto pulmonar ocurre en un 29 a 32% de pacientes con TEP (1–3).
El infarto pulmonar secundario a embolia pulmonar es más frecuente en pacientes con baja reserva cardiopulmonar (4); al respecto, un estudio evidenció que en pacientes con TEP, los infartos pulmonares se dieron un 36% en pacientes con falla cardíaca congestiva y un 54% en pacientes con hipotensión y shock (5). Sin embargo, estudios más recientes han indicado que pacientes jóvenes con buen estado de salud previo al TEP pueden tener incidencias más altas de infarto pulmonar (6,3). Además, una alta carga trombótica ha sido asociada con una mayor probabilidad de infarto pulmonar, aunque esta condición sucede en arterias pulmonares pequeñas (7).
Por lo general, el infarto pulmonar causa dolor pleurítico, taquipnea, disnea y, en muy raras ocasiones, tos con hemoptisis (8), por lo que diferenciarlo radiológicamente de otras entidades como masas, atelectasias y neumonía es complicado.
El infarto pulmonar suele observarse en regiones subpleurales y se presenta predominantemente en los lóbulos inferiores, en especial el derecho; el hallazgo radiológico más común es una consolidación triangular del parénquima pulmonar (50%), aunque también pueden observarse segmentos con patrón de vidrio esmerilado (35.9%) y el signo de Hampton (14.5%), características que ayudan a diferenciarlo de masas y neumonía (6,9,10).
Múltiples complicaciones se han asociado al infarto pulmonar, entre ellas neumonía, neumotórax, fistula broncopulmonar, hemorragia alveolar, cavitaciones, empiema y absceso pulmonar (11). Por su parte, la infección asociada a infarto pulmonar es una complicación poco frecuente pero importante, ya que puede resultar en la formación de abscesos y empiemas que pueden requerir drenaje quirúrgico.
Se ha sugerido que la obstrucción de un vaso pulmonar secundaria a un embolo estéril genera extravasación sanguínea dentro de los tejidos circundantes, edema de las paredes bronquiales adyacentes e incremento de la secreción endobronquial, lo que forma un ambiente propicio para la colonización e infección bacteriana, la cual puede provenir por vía aérea, o hematógena (12). Bashir & Benson (13), con base en series de estudios postmortem, estimaron la incidencia de infección de infartos pulmonares en 2 a 7% (13). El desarrollo de fiebre, sudoración, taquicardia, esputo purulento, deterioro del estado general y leucocitosis luego de un infarto pulmonar es altamente sugestivo de infección, razón por la cual se ha sugerido que el espectro de agentes etiológicos es similar al descrito en la neumonía nosocomial (11). En los casos de infarto pulmonar infectado, las terapias anticoagulante y antibiótica deben iniciarse oportunamente y seleccionarse según los patrones de resistencia local, los patógenos asociados, las características del paciente y el contexto clínico en general (5).
A continuación se describe un caso clínico compatible con tromboembolia pulmonar el cual se vio complicado con infarto pulmonar infectado.
Presentación del caso
Mujer de 49 años, procedente de Bogotá, Colombia, con oficio de contador público y quien consultó por presentar cuadró clínico de dos días consistente de dolor en hemitórax izquierdo de características pleuríticas, irradiado a región dorsal, asociado a disnea súbita, edema, rubor y calor a nivel de miembro inferior izquierdo. No refirió fiebre, tos, ni hemoptisis. Dos semanas antes de la consulta al servicio, había sido sometida a reconstrucción de menisco, ligamento cruzado anterior y posterior y condroplastia de la rodilla izquierda, secundaria a trauma cerrado. Por motivos desconocidos, no registrados en la historia clínica, no se le realizó profilaxis antitrombótica postoperatoria. Por último, como antecedente de importancia, la paciente presentaba obesidad grado 1, sin otros antecedentes patológicos, tóxicos, alérgicos, ni hospitalizaciones previas.
Al examen físico de ingreso, se encontraba en regulares condiciones generales, con tensión arterial de 97/63 mmHg, frecuencia cardíaca de 106 lpm, frecuencia respiratoria de 20 rpm, saturación de oxígeno al 96%, con fracción inspirada de oxígeno de 0.21, y temperatura axilar de 36.5° centígrados. La paciente medía 160 cm y pesaba 83 kg, lo que arrojó un índice de masa corporal (IMC) de 32.4 Kg/m2. En la auscultación del tórax se identificó P2>A2, sin hallar soplos; también se auscultaron estertores finos en la base pulmonar izquierda. En miembro inferior izquierdo se encontró edema del pie y del tercio proximal de la pierna, con eritema local y dolor a palpación superficial.
Se realizaron los siguientes exámenes: hemograma, electrolitos, nitrógeno ureico en la sangre (BUN) y creatinina, los cuales se encontraron dentro de los límites normales. Por otra parte, el electrocardiograma mostró taquicardia sinusal, mientras que el ecocardiograma, corazón estructural y funcionalmente normal. Finalmente, en la radiografía de tórax se evidenció atelectasia laminar basal izquierda y crecimiento de aurícula derecha (Figura 1).
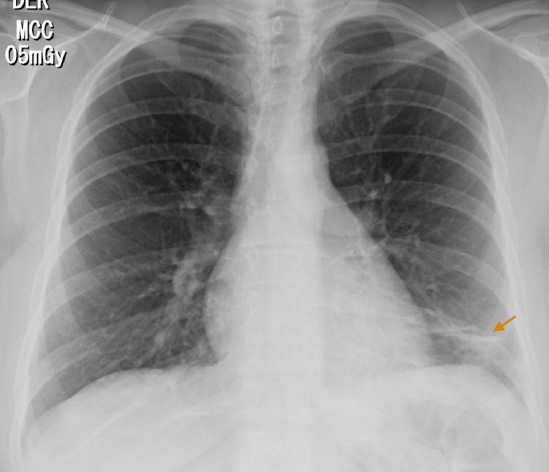
Figura 1. Radiografía de tórax postero-anterior. Imagen en banda basal izquierda que corresponde a atelectasia (flecha).
Fuente: Documento obtenido durante la realización del estudio.
Se aplicó la escala Wells, encontrando alta probabilidad para tromboembolia pulmonar, por lo que se inició anticoagulación con heparina de bajo peso molecular (enoxaparina) a dosis de 1 mg/kg cada 12 horas, y se solicitó angiotomografía axial computarizada (AngioTAC) de tórax, gracias a la cual se confirmó la sospecha diagnóstica, reportando obstrucción de arteria pulmonar en el tronco del segmento basal inferior izquierdo (Figura 2).

Figura 2. Angiotomografía de tórax. Plano axial. Embolismo pulmonar, defecto de llenado configurando el signo de salvavidas (flecha).
Fuente: Documento obtenido durante la realización del estudio.
Sorprendentemente, luego de iniciar la anticoagulación y otras medidas generales de tratamiento indicadas para tromboembolia pulmonar, y cerca de tres días después de su hospitalización, la paciente presentó empeoramiento del dolor torácico, disnea, aumento de requerimientos de flujo de oxígeno por cánula nasal, fiebre, leucocitosis, taquicardia y taquipnea. Se solicitaron paraclínicos de control, encontrándose proteína C reactiva elevada y aumento importante de leucocitos a expensas de neutrófilos. Se realizó nueva evaluación tomográfica de tórax, en la que se identificaron híper densidades en cuña en los lóbulos medio e inferior derecho y lóbulo inferior izquierdo, así como broncograma aéreo en lóbulo inferior derecho y derrame pleural bilateral (Figura 3 y 4). No se realizaron hemocultivos ni cultivos de esputo.

Figura 3. Angiotomografía de tórax. Plano coronal. Embolismo pulmonar, defecto de llenado configurando signo de la carrilera (flecha), consolidación basal izquierda de base pleural amplia y broncograma aéreo que corresponde a infarto pulmonar (estrella).
Fuente: Documento obtenido durante la realización del estudio.

Figura 4. AngioTAC de tórax. Consolidación de base amplia, vértice hiliar, bordes obtusos corresponde a infarto pulmonar (estrella), derrame pleural (flecha).
Fuente: Documento obtenido durante la realización del estudio.
Con base en lo anterior, se diagnosticó infarto pulmonar infectado y se inició tratamiento antibiótico de amplio espectro con piperacilina + tazobactam a dosis de 4.5 g por vía intravenosa cada seis horas, teniendo en cuenta que la infección se presentó de forma intrahospitalaria y que la paciente había pasado por una hospitalización reciente, lo que aumentaba el riesgo de gérmenes resistentes.
La paciente mejoró de manera progresiva, iniciando anticoagulación oral con warfarina 5 mg cada 24 horas; tras completar el séptimo día de tratamiento antibiótico y con INR (International Normalized Ratio) en rango terapéutico se dio de alta para continuar anticoagulación inicialmente por tres meses, y controles ambulatorios por medicina interna. No se presentaron reacciones adversas a los tratamientos durante la hospitalización. La Figura 4 muestra la línea del tiempo del caso reportado.
Figura 4. Línea de tiempo.
Fuente: Documento obtenido durante la realización del estudio.
Discusión
Este caso expone la evolución clínica de una paciente con TEP, el cual progresó a infarto pulmonar y a infección del tejido pulmonar necrótico. Es un caso relevante desde varios puntos de vista, pues denota la importancia de realizar trombo profilaxis en pacientes con factores de riesgo y expone complicaciones que ponen en riesgo la vida de la paciente y generan retos diagnósticos, terapéuticos y de investigación.
Muchos factores de riesgo han sido identificados en la tromboembolia pulmonar; en el presente caso, la paciente presentaba los siguientes: trauma, cirugía, inmovilidad y obesidad (14).
Se ha demostrado que la incidencia de TEP puede reducirse realizando trombo profilaxis en pacientes sometidos a cirugía ortopédica de rodilla, en particular cuando existen factores adicionales de riesgos (15). Por lo anterior, se recomienda mantener la profilaxis hasta que los pacientes recuperen su movilidad (16).
Por otro lado, el diagnóstico de TEP se realizó de acuerdo a las guías de práctica clínica (17), clasificando la probabilidad por escala de Wells y confirmando el diagnóstico con la prueba de elección, en este caso, la AngioTAC de tórax.
La evolución del cuadro clínico de la paciente, además del desarrollo de respuesta inflamatoria sistémica, elevación de reactantes de fase aguda, exacerbación del dolor pleurítico y deterioro respiratorio, causó la sospecha de infarto pulmonar infectado (8). Esta presentación clínica, junto con las imágenes diagnósticas compatibles, fueron la base del diagnóstico. En este caso, se logró una mejoría significativa, permitiendo el alta hospitalaria y un buen pronóstico a corto y largo plazo.
Ahora bien, es importante mencionar que este reporte tiene marcadas limitaciones: la falta de aislamientos microbiológicos que determinaran el agente etiológico, la falta de guías de práctica clínica para el diagnóstico y tratamiento del infarto pulmonar infectado y la dificultad radiológica para diferenciar neumonía bacteriana e infarto pulmonar (11). Además, la elección del tratamiento antibiótico se realizó basándose en la extrapolación de las guías locales para el tratamiento de neumonía nosocomial.
Se requiere mayor investigación en el tema de infarto pulmonar infectado para lograr una mejor comprensión, abordaje diagnóstico, tratamiento y prevención de esta entidad, lo anterior con el fin de mejorar la atención y mejorar los desenlaces clínicos de los pacientes.
En conclusión, el infarto pulmonar es una complicación común de la tromboembolia pulmonar, que, en raras ocasiones, puede infectarse. En consecuencia, una alta sospecha y adecuada interpretación de la evolución son necesarias para establecer el diagnóstico y lograr un manejo oportuno.
Perspectiva del paciente
La paciente manifestó gratitud por la atención médica prestada de forma idónea y humanizada.
Consentimiento informado
La paciente dio su consentimiento para la publicación de la información utilizada en este reporte de caso.
Conflictos de interés
Ninguno declarado por los autores.
Financiación
Ninguna declarada por los autores.
Referencias
1. Kirchner J, Obermann A, Stückradt S, Tüshaus C, Goltz J, Liermann D, et al. Lung Infarction Following Pulmonary Embolism: A Comparative Study on Clinical Conditions and CT Findings to Identify Predisposing Factors. Rofo. 2015;;187(6):440-4. http://doi.org/bx9z.
2.Gadkowski LB, Stout JE. Cavitary pulmonary disease. Clin Microbiol Rev. 2008;21(2):305-33, table of contents. http://doi.org/dq4kf8.
3.Miniati M, Bottai M, Ciccotosto C, Roberto L, Monti S. Predictors of Pulmonary Infarction. Medicine (Baltimore). 2015;94(41):e1488. http://doi.org/f3pjf5.
4.Morgenthaler TI, Ryu JH, Utz JP. Cavitary Pulmonary Infarct in Immunocompromised Hosts. Mayo Clin Proc. 1995;70(1):66-8. http://doi.org/dzxf35.
5.Hampton AO, Castleman B. Correlation of postmortem chest teleroentgenograms with autopsy findings with special reference to pulmonary embolism and infarction. AJR Am J Roentgenol. 1940;43:305-26.
6.Miniati M. Pulmonary Infarction: An Often Unrecognized Clinical Entity. Semin Thromb Hemost. 2016;42(8):865-9. http://doi.org/bx92.
7.Cha S-I, Shin K-M, Lee J, Hwangbo Y, Yoo S-S, Lee J, et al. Clinical relevance of pulmonary infarction in patients with pulmonary embolism. Thromb Res. 2012;130(3):e1-5. http://doi.org/bx93.
8.Stein PD, Henry JW. Clinical Characteristics of Patients With Acute Pulmonary Embolism Stratified According to Their Presenting Syndromes. Chest. 1997;112(4):974-9. http://doi.org/bkzg44.
9.Kuriakose J, Patel S. Acute Pulmonary Embolism. Radiol Clin N Am. 2010;48(1):31-50. http://doi.org/dgsj4k.
10.He H, Stein MW, Zalta B, Haramati LB. Pulmonary infarction: spectrum of findings on multidetector helical CT. J Thorac Imaging. 2006 Mar;21(1):1-7. http://doi.org/bj9n4b.
11.Djordjevic I, Pejcic T. Cavitary Pulmonary Infarct: The Differential Diagnostic Dilemma - A Case Report. In: Okuyan Erugrul (Ed.). Venous Thrombosis - Principles and Practice. InTech; 2012 http://doi.org/bx94.
12. Janes RM. Abscess of the Lung. Can Med Assoc J. 1942 [cited 2016 Jul 30];47(6):540-5. Available from: https://goo.gl/Hrn5Hj.
13.Bashir Y, Benson MK. Necrotising pneumonia and empyema due to Clostridium perfringens complicating pulmonary embolus. Thorax. 1990;45(1):72-3. http://doi.org/fqkc8t.
14.Steffen LM, Cushman M, Peacock JM, Heckbert SR, Jacobs DR Jr, Rosamond WD, et al. Metabolic syndrome and risk of venous thromboembolism: Longitudinal Investigation of Thromboembolism Etiology. J Thromb Haemost. 2009;7(5):746-51. http://doi.org/dqjbcx.
15.Kearon C. Natural History of Venous Thromboembolism. Circulation. 2003;107(23 suppl 1):I22-30.
16.National Institute for Health and Care Excellence (NICE). Venous thromboembolism: reducing the risk for patients in hospital. Londres: NICE; 2010 [cited 2016 Jul 30]. Clinical guideline [CG92]. Available from: https://goo.gl/wbRNc7.
17.Konstantinides S, Torbicki A, Agnelli G, Danchin N, Fitzmaurice D, Galiè N, et al. Guía de práctica clínica de la ESC 2014 sobre el diagnóstico y el tratamiento de la embolia pulmonar aguda. Rev Española Cardiol. 2015;68(1):64.e1-64.e45. http://doi.org/f2xz6j.
Referencias
Kirchner J, Obermann A, Stückradt S, Tüshaus C, Goltz J, Liermann D, et al. Lung Infarction Following Pulmonary Embolism: A Comparative Study on Clinical Conditions and CT Findings to Identify Predisposing Factors. Rofo. 2015;;187(6):440-4. http://doi.org/bx9z
Gadkowski LB, Stout JE. Cavitary pulmonary disease. Clin Microbiol Rev. 2008;21(2):305-33, table of contents. http://doi.org/dq4kf8
Miniati M, Bottai M, Ciccotosto C, Roberto L, Monti S. Predictors of Pulmonary Infarction. Medicine (Baltimore). 2015;94(41):e1488. http://doi.org/f3pjf5
Morgenthaler TI, Ryu JH, Utz JP. Cavitary Pulmonary Infarct in Immunocompromised Hosts. Mayo Clin Proc. 1995;70(1):66-8. http://doi.org/dzxf35
Hampton AO, Castleman B. Correlation of postmortem chest teleroentgenograms with autopsy findings with special reference to pulmonary embolism and infarction. AJR Am J Roentgenol. 1940;43:305-26
Miniati M. Pulmonary Infarction: An Often Unrecognized Clinical Entity. Semin Thromb Hemost. 2016;42(8):865-9. http://doi.org/bx92
Cha S-I, Shin K-M, Lee J, Hwangbo Y, Yoo S-S, Lee J, et al. Clinical relevance of pulmonary infarction in patients with pulmonary embolism. Thromb Res. 2012;130(3):e1-5. http://doi.org/bx93
Stein PD, Henry JW. Clinical Characteristics of Patients With Acute Pulmonary Embolism Stratified According to Their Presenting Syndromes. Chest. 1997;112(4):974-9. http://doi.org/bkzg44
Kuriakose J, Patel S. Acute Pulmonary Embolism. Radiol Clin N Am. 2010;48(1):31-50. http://doi.org/dgsj4k
He H, Stein MW, Zalta B, Haramati LB. Pulmonary infarction: spectrum of findings on multidetector helical CT. J Thorac Imaging. 2006 Mar;21(1):1-7. http://doi.org/bj9n4b
Djordjevic I, Pejcic T. Cavitary Pulmonary Infarct: The Differential Diagnostic Dilemma - A Case Report. In: Okuyan Erugrul (Ed.). Venous Thrombosis - Principles and Practice. InTech; 2012 http://doi.org/bx94
Janes RM. Abscess of the Lung. Can Med Assoc J. 1942 [cited 2016 Jul 30];47(6):540-5. Available from: https://goo.gl/Hrn5Hj
Bashir Y, Benson MK. Necrotising pneumonia and empyema due to Clostridium perfringens complicating pulmonary embolus. Thorax. 1990;45(1):72-3. http://doi.org/fqkc8t
Steffen LM, Cushman M, Peacock JM, Heckbert SR, Jacobs DR Jr, Rosamond WD, et al. Metabolic syndrome and risk of venous thromboembolism: Longitudinal Investigation of Thromboembolism Etiology. J Thromb Haemost. 2009;7(5):746-51. http://doi.org/dqjbcx
Kearon C. Natural History of Venous Thromboembolism. Circulation. 2003;107(23 suppl 1):I22-30
National Institute for Health and Care Excellence (NICE). Venous thromboembolism: reducing the risk for patients in hospital. Londres: NICE; 2010 [cited 2016 Jul 30]. Clinical guideline [CG92]. Available from: https://goo.gl/wbRNc7
Konstantinides S, Torbicki A, Agnelli G, Danchin N, Fitzmaurice D, Galiè N, et al. Guía de práctica clínica de la ESC 2014 sobre el diagnóstico y el tratamiento de la embolia pulmonar aguda. Rev Española Cardiol. 2015;68(1):64.e1-64.e45. http://doi.org/f2xz6j
Cómo citar
APA
ACM
ACS
ABNT
Chicago
Harvard
IEEE
MLA
Turabian
Vancouver
Descargar cita
Licencia
Derechos de autor 2017 Case reports

Esta obra está bajo una licencia internacional Creative Commons Atribución 4.0.
Los autores al someter sus manuscritos conservarán sus derechos de autor. La revista tiene el derecho del uso, reproducción, transmisión, distribución y publicación en cualquier forma o medio.
El Formulario de Divulgación Uniforme para posibles Conflictos de Interés y los oficios de cesión de derechos y de responsabilidad deben ser entregados junto con el original.
Aquellos autores/as que tengan publicaciones con esta revista, aceptan los términos siguientes:
Los autores/as conservarán sus derechos de autor y garantizarán a la revista el derecho de primera publicación de su obra, el cual estará simultáneamente sujeto a la Licencia de reconocimiento de Creative Commons 4.0 que permite a terceros compartir la obra siempre que se indique su autor y su primera publicación en esta revista.
Los autores/as podrán adoptar otros acuerdos de licencia no exclusiva de distribución de la versión de la obra publicada (p. ej.: depositarla en un archivo telemático institucional o publicarla en un volumen monográfico) siempre que se indique la publicación inicial en esta revista.
Se permite y recomienda a los autores/as difundir su obra a través de Internet (p. ej.: en archivos telemáticos institucionales o en su página web) antes y durante el proceso de envío, lo cual puede producir intercambios interesantes y aumentar las citas de la obra publicada. (Véase El efecto del acceso abierto).























