



Publicado
Algoritmo para el diagnóstico diferencial del trastorno por somatización en cuidado médico primario
Algorithm for differential diagnosis of somatization disorder in primary care
Palabras clave:
atención primaria de salud, diagnóstico diferencial, epidemiología, historia, trastornos. (es)Diagnosis, Differential, Epidemiology, History, Primary Health Care, Somatoform Disorders. (en)
Antecedentes. En la práctica clínica de atención primaria existe poca información sobre cómo hacer el diagnóstico de trastorno por somatización y cuáles son sus posibles entidades diferenciales, lo que lleva a un deterioro en la relación médico paciente, dificultades en el tratamiento de personas que sufren esta condición y retrasos en el diagnóstico de otras patologías médicas que se constituyen en los diagnósticos a excluir en pacientes con síntomas físicos inexplicables.
Objetivo. Determinar el diagnóstico diferencial del trastorno por somatización en cuidado médico primario y plantear un algoritmo para su abordaje.
Material y métodos. Se realizó búsqueda en las bases de datos PubMed, LILACS y Publindex, combinando las palabras clave Somatoform Disorders and Diagnosis, Differential, con 968 resultados, al agregar AND Primary Health Care, con 62 resultados en la fecha 28/07/2009; se leyeron los títulos y resúmenes, escogiendo los artículos relacionados con el objetivo de la revisión.
Resultados. Existen varias enfermedades crónicas que al comprometer varios órganos y sistemas causan síntomas inespecíficos semejantes al trastorno por somatización. Tenerlas presentes permite descartarlas de forma temprana por medio de exámenes de baja complejidad.
Conclusión. El diagnóstico de trastorno por somatización en cuidado médico primario, a pesar de ser altamente complejo, permite mediante el uso de este algoritmo orientar mejor la intervención del médico general, favoreciendo la reducción en procedimientos y consultas especializadas y el inicio temprano del tratamiento específico.
Background. There is little information about how to do the diagnosis of somatization disorder and which are the differential diseases in the primary health care, it deteriorates the doctor-patient relationship, it obstructs the treatment for people who has this illness and it delays the diagnosis of different pathologies which are in the differential diagnosis for patients with medically unexplained symptoms.
Objective. To determine the differential diagnosis of somatization disorder in primary medical care and pose an algorithm to address this.
Methods. We searched the databases, PubMed, LILACS and Publindex combining the key words Somatoform Disorders AND Diagnosis, Differential, with 968 results, add AND Primary Health Care, with 62 results on the date 28/07/2009, was read the titles and abstracts by selecting items related to the purpose of the review.
Results. There are several chronic diseases that compromise the various organ systems, causing symptoms, similar to somatization disorder. Have them present allow for early discard through tests of low complexity.
Conclusion: The diagnosis of somatization disorder in primary medical care, despite being highly complex, by allowing the use of this algorithm to better direct the intervention of the general practitioner by encouraging the reduction procedures and specialist consultations and early initiation of specific treatment.
ACTUALIZACIÓN
ALGORITMO PARA EL DIAGNÓSTICO DIFERENCIAL DEL TRASTORNO POR SOMATIZACIÓN EN CUIDADO MÉDICO PRIMARIO
Algorithm for differential diagnosis of somatization disorder in primary care
óscar Rangel-Urrea1, Nohora Barrera-Guío1, Franklin Escobar-Córdoba2
1 Residente tercer año de Psiquiatría, Facultad de Medicina, Universidad Nacional de Colombia, Bogotá. 2 Profesor Asociado, Departamento de Psiquiatría, Facultad de Medicina, Universidad Nacional de Colombia, Bogotá.Correspondencia:FEESCOBARC@BT.UNAL.EDU.CO
Recibido para publicación:24/08/09
Aceptado para publicación:16/11/09
Resumen
Antecedentes. En la práctica clínica de atención primaria existe poca información sobre cómo hacer el diagnóstico de trastorno por somatización y cuáles son sus posibles entidades diferenciales, lo que lleva a un deterioro en la relación médico paciente, dificultades en el tratamiento de personas que sufren esta condición y retrasos en el diagnóstico de otras patologías médicas que se constituyen en los diagnósticos a excluir en pacientes con síntomas físicos inexplicables.
Objetivo. Determinar el diagnóstico diferencial del trastorno por somatización en cuidado médico primario y plantear un algoritmo para su abordaje.
Material y métodos. Se realizó búsqueda en las bases de datos PubMed, LILACS y Publindex, combinando las palabras clave Somatoform Disorders and Diagnosis, Differential, con 968 resultados, al agregar AND Primary Health Care, con 62 resultados en la fecha 28/07/2009; se leyeron los títulos y resúmenes, escogiendo los artículos relacionados con el objetivo de la revisión.
Resultados. Existen varias enfermedades crónicas que al comprometer varios órganos y sistemas causan síntomas inespecíficos semejantes al trastorno por somatización. Tenerlas presentes permite descartarlas de forma temprana por medio de exámenes de baja complejidad.
Conclusión. El diagnóstico de trastorno por somatización en cuidado médico primario, a pesar de ser altamente complejo, permite mediante el uso de este algoritmo orientar mejor la intervención del médico general, favoreciendo la reducción en procedimientos y consultas especializadas y el inicio temprano del tratamiento específico.
Palabras claves: atención primaria de salud, diagnóstico diferencial, epidemiología, historia, trastornos.
Rangel-Urrea O, Barrera-Guío N, Escobar-Córdoba F. Algoritmo para el diagnóstico diferencial del trastorno de somatización en cuidado médico primario. rev.fac.med. 2009; 57: 334-346.
Summary
Background. There is little information about how to do the diagnosis of somatization disorder and which are the differential diseases in the primary health care, it deteriorates the doctor-patient relationship, it obstructs the treatment for people who has this illness and it delays the diagnosis of different pathologies which are in the differential diagnosis for patients with medically unexplained symptoms.
Objective. To determine the differential diagnosis of somatization disorder in primary medical care and pose an algorithm to address this.
Methods. We searched the databases, PubMed, LILACS and Publindex combining the key words Somatoform Disorders AND Diagnosis, Differential, with 968 results, add AND Primary Health Care, with 62 results on the date 28/07/2009, was read the titles and abstracts by selecting items related to the purpose of the review.
Results. There are several chronic diseases that compromise the various organ systems, causing symptoms, similar to somatization disorder. Have them present allow for early discard through tests of low complexity.
Conclusion: The diagnosis of somatization disorder in primary medical care, despite being highly complex, by allowing the use of this algorithm to better direct the intervention of the general practitioner by encouraging the reduction procedures and specialist consultations and early initiation of specific treatment .
Key words: Diagnosis, Differential, Epidemiology, History, Primary Health Care, Somatoform Disorders.
Rangel-Urrea O, Barrera-Guío N, Escobar-Córdoba F. Algorithm for differential diagnosis of somatization disorder in primary care. rev.fac.med. 2009; 57: 334-346.
Introducción
El trastorno por somatización es uno de los trastornos somatomorfos del manual diagnóstico y estadístico de los trastornos mentales de la Asociación Psiquiátrica en Americana (DSM-IV-TR) (1), correspondiendo a una entidad diagnóstica específica con criterios precisos que deben estar presentes para hacer el diagnóstico. Sin embargo, se evidencia en la práctica clínica de atención primaria en Colombia que existe poca información en los médicos sobre cómo hacer este diagnóstico y sus posibles entidades diferenciales, lo que finalmente lleva a un deterioro en la relación médico-paciente, a dificultades en el tratamiento de las personas que sufren esta condición (2), y a retrasos en el diagnóstico de otras patologías médicas que se constituyen en los diagnósticos diferenciales de dicha entidad (3).
Lipkowski definió la somatización en 1988 como "la tendencia a experimentar y expresar síntomas y malestares físicos, eventos no relacionados con hallazgos patológicos atribuyéndolos a enfermedades médicas". Este autor afirma que en la somatización las emociones que deberían ser expresadas simbólicamente por medio de palabras, son traducidas a percepciones corporales (4,5). Por lo anterior, los pacientes con trastorno por somatización deberían ser manejados por psiquiatras, pero lo que se ha encontrado es que la gran mayoría son tratados por otros especialistas que poseen conocimientos limitados sobre esta entidad (6).
La conceptualización alrededor de la somatización requiere hacer la distinción entre "estar enfermo" y "sentirse enfermo". Sentirse enfermo corresponde a la experiencia subjetiva derivada de la percepción individualizada de los síntomas corporales. Estar enfermo se define como la demostración objetiva de la alteración en el funcionamiento o estructura corporales (7). El desacuerdo entre "estar enfermo" y "sentirse enfermo" es lo que constituye el trastorno de somatización (8). Las dificultades en esta diferenciación pueden llevar muchas veces a los médicos a interpretaciones erróneas sobre dicha entidad, como las concluidas por Huapaya en su revisión del tema (9), en donde afirma que si un paciente escucha frases como "usted no tiene nada malo" o "esto es sólo producto de su imaginación", bastante frecuentes en los acercamientos de los pacientes a los servicios de salud, pierde confianza en el médico y queda con la percepción de que sus quejas no son tomada de forma seria. Lo anterior da explicación de las dificultades generadas en el contacto en cuidado primario entre los médicos y estos pacientes (10).
Es de aclarar que la ausencia de una enfermedad orgánica no indica la presencia de una enfermedad psiquiátrica necesariamente (11). Existe la percepción común entre los médicos de que los síntomas físicos en ausencia de hallazgos fisiopatológicos fuertes, por ejemplo signos al examen físico o hallazgos de laboratorio, son menos importantes que los apreciados en el contexto de una enfermedad identificable.
Los conflictos entre el médico y el paciente ocurren a menudo cuando el enfermo se presenta con síntomas físicos inexplicables, pues la valoración que cada uno hace al respecto es distinta; el médico por su parte considera estos síntomas como poco importantes lo que produce frustración en él e insatisfacción en el paciente (12). El 80 por ciento de las personas alguna vez en su vida ha presentado síntomas físicos sin hallazgos al examen físico o de laboratorio (13).
Material y métodos
Para desarrollar el algoritmo propuesto se realizó búsqueda en las bases de datos PubMed, Lilacs y Publindex, combinando las palabras clave "Somatoform Disorders" AND "Diagnosis, Differential", con 968 resultados, al agregar AND "Primary Health Care", con 62 resultados en la fecha 28/07/2009; se leyeron los títulos y resúmenes, escogiendo los artículos relacionados con el objetivo de la revisión, quedando un total de 50 artículos. No se colocaron límites a la búsqueda.
Resultados
Antecedentes históricos
Antiguamente los egipcios afirmaron que las mujeres con este síndrome tenían el útero displásico, lo que causaba alteraciones difusas en otros órganos, y con ellas, otros síntomas. Los griegos también pensaban que el útero era la fuente de los síntomas físicos inexplicables al observarlo como un síndrome casi exclusivo en mujeres. Thomas Sydenham, en el siglo XVII, reconoció que dicha alteración también estaba presente en los hombres. En los siglos XIX y XX Briquet, Freud y Breuer exploraron el fenómeno e hicieron importantes contribuciones a su entendimiento y estudio (8).
Se han encontrado otras culturas reconociendo la existencia de una importante interregu-lación entre lo que se ha denominado dualidad mente-cuerpo, como es el caso de la cultura hindú en la cual, por medio de la meditación, se busca la salud de la mente fortaleciendo así el cuerpo y el espíritu (6). Estudios naturalísticos validados en América del Norte mostraron un síndrome originalmente llamado histeria, luego síndrome de Briquet y finalmente trastorno de somatización, término que actualmente se encuentra en las nomenclaturas fenomeno¬lógicas (1,14).
La evolución del diagnóstico de trastorno de somatización muestra que los síntomas requeridos dentro de los criterios han sido arbitrariamente seleccionados en las sucesivas nomenclaturas, agregando o quitándolos por deliberación de comités de investigadores y expertos en el tema (14).
Definición
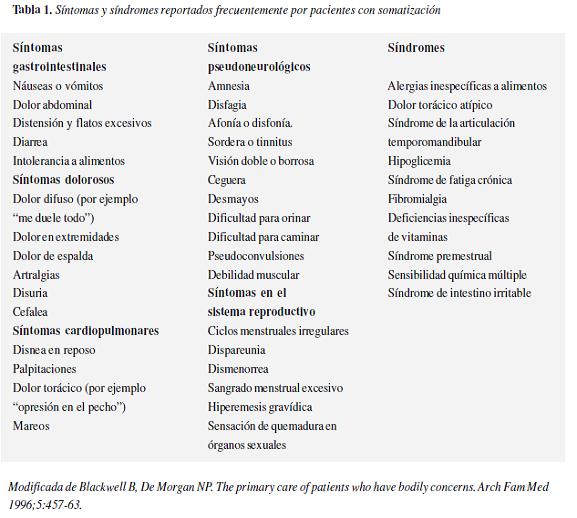
El trastorno de somatización está definido por el DSM-IV-TR como un patrón de síntomas somáticos, recurrentes, múltiples y clínicamente significativos (1). Se considera que un síntoma somático es clínicamente significativo si requiere tratamiento médico o causa un deterioro evidente de la actividad social, laboral o en otras áreas importantes de la actividad del individuo, siendo necesario que se inicie antes de los 30 años de edad y persista por varios años más. Cada uno de los síntomas puede aparecer o cesar en cualquier momento de la alteración, no siendo necesario que estén presentes todos en un mismo periodo. Con el fin de facilitar su exploración y abordaje han sido reunidos en cuatro grupos: cuatro síntomas dolorosos, dos síntomas gastrointestinales, un síntoma sexual y un síntoma pseudoneurológico (15).
El anterior cuadro clínico debe cumplir dos características: primero, no se puede explicar por la presencia de una enfermedad médica o los efectos de una sustancia, o en el caso de que exista una enfermedad médica, los síntomas o el deterioro funcional son excesivos en comparación con lo que se esperaría por la historia clínica, la exploración física o los hallazgos de laboratorio; segundo, estos síntomas no son producidos intencionalmente ni son simulados (16) tabla 1.
Es de vital importancia para el bienestar de los pacientes entender que muchos de los síntomas que se presentan en el trastorno de somatización también aparecen en pacientes con patología orgánica (17).
Etiología
Existen múltiples propuestas etiológicas sobre el trastorno, dentro de las cuales se exponen componentes genéticos y biológicos sumados a factores externos (18). Hakala y cols. publicaron en 2004 un estudio en el que se examinó el volumen del núcleo caudado, el putamen y las estructuras hipocampales cerebrales por resonancia nuclear magnética (RNM) en mujeres con trastorno de somatización o trastorno somatomorfo indiferenciado, haciendo comparaciones con voluntarias sanas, encontrando que las primeras tenían alargamiento bilateral de los volúmenes del núcleo caudado comparadas con las voluntarias sanas, sugiriendo así que estas diferencias podrían estar asociadas con la fisiopatología de la somatización (19).
Dentro de la exploración de los factores externos, situaciones como ser criado por padres enfermos o ser víctima de abuso psicológico o sexual en épocas tempranas de la vida, han sido definidos como predisponentes claros de síntomas físicos inexplicables (8).
Aunque la fisiopatología para su presentación no está establecida con claridad existen cuatro mecanismos frecuentemente desarrollados por estos individuos. Primero, la amplificación de las sensaciones corporales genera evidencia confirmatoria para el paciente frente a sus sospechas de estar enfermo. Segundo, cuando un sistema familiar está expuesto a algún tipo de estresor generalmente lleva a que uno de sus miembros exprese un síntoma como puerta de entrada para que el resto del sistema reciba atención. El tercer mecanismo sería la necesidad inconsciente de tomar el papel de enfermo como medio de expresión "de un dolor psicológico". El último mecanismo consistiría en la disociación, que se afirma por estudios de neuroimágenes durante experiencias disociativas como los sueños y las reviviscencias o flashbacks, las cuales sugieren que las mismas áreas sensoriales en el sistema nervioso central son activadas por eventos tanto externos por ejemplo: estresores psicosociales; como internos, por ejemplo: percepción de síntomas físicos e interpretación de éstos como enfermedades (17,20).
Epidemiología
Se encuentra la creencia generalizada entre muchos médicos de atención primaria que la presencia de síntomas físicos que no pueden ser explicados por una enfermedad médica es un fenómeno no sólo poco importante sino también infrecuente (21). Existen artículos publicados desde principios del siglo pasado, como el desarrollado por Cabot, en el Massachusetts General Hospital, donde se muestra que de 5.000 pacientes de consulta externa, en el 47 por ciento no se encontró causa orgánica de la sintomatología que originaba la consulta (22). Nimnuan y cols. publicaron los resultados de un ensayo en donde se halló que de una a dos terceras partes de los pacientes atendidos en clínicas generales (n = 550/890) no reciben explicación biomédica para sus quejas. Estos síntomas físicos inexplicables son más comunes en mujeres y en el grupo de jóvenes de los 16 a los 25 años de edad (23). Algunos estudios como el Epidemiologic Catchment Area han revelado prevalencias del trastorno de somatización en 0,1 por ciento a 0,8 por ciento en la población general occidental, con una razón mujer/hombre de 10 a 1 (24,25).
Diagnóstico diferencial
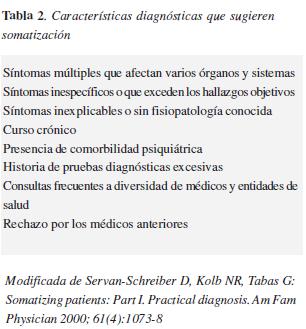
La experiencia clínica y las investigaciones existentes en cuanto a criterios diagnósticos para las formas severas de somatización, sugieren que la existencia de tan sólo dos características, proporciona una alta probabilidad de diagnóstico positivo acertado en un paciente en cuidado primario. La primera corresponde a la presencia de tres o más síntomas inespecíficos o exagerados, manifestados en diferentes órganos y sistemas y que aparecen frecuentemente. La segunda, un curso crónico de por lo menos dos años. Otras situaciones no tan específicas como las anteriores pero igual de sugerentes son las historias de malas relaciones con los tratantes previos, evidencia de múltiples visitas a diferentes especialistas con el consecuente sometimiento a procedimientos diagnósticos y terapéuticos, y por último, la presencia o historia de psicopatología (26) tabla 2.
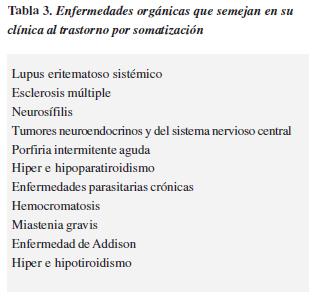
Lo anterior se constituye en información que permite iniciar el proceso de estudio en cuanto a su etiología, siendo de vital importancia descartar enfermedades crónicas con síntomas inespecíficos y en múltiples sistemas que evidentemente se asemejan en su presentación al trastorno de somatización (27,28) Tabla 3.
El lupus eritematoso sistémico (LES) es una patología que involucra al sistema nervioso central, periférico y autonómico. Constituye una entidad relativamente frecuente con una relación mujer/hombre de 5 a 1. Algunas de sus manifestaciones, que son comunes con el trastorno de somatización son cefalea, convulsiones, fotosensibilidad, rash, artralgias, movimientos anormales, cambios en el afecto, ansiedad y otras derivadas del compromiso nervioso periférico y autonómico, como disestesias, anestesias atípicas, neuropatías motoras y manifestaciones gastrointestinales, urinarias y sexuales cuando los afectados son los plexos mesentéricos y sacros (29). Ante la posibilidad diagnóstica de LES, ya sea derivada del cuadro clínico, las características epidemiológicas del paciente o su historia familiar, es indispensable realizar un estudio encaminado a descartarlo. Evaluar la función renal y el estado hematológico, buscar anticuerpos antinucleares y antifosfolípidos, y según el compromiso neuropsiquiátrico contar con una imagen cerebral, son requisitos mínimos para el abordaje inicial y adecuado de estos pacientes (30).
De bastante similitud con el LES, la esclerosis múltiple (EM) se caracteriza por una serie de manifestaciones en varios sistemas que ante los ojos de cualquier observador no neurólogo parecen inespecíficos (30). Son frecuentes las alteraciones sensitivas y motoras, cambios en el afecto, siendo la depresión lo más frecuente; déficits corticales focales, dolor y ceguera unilaterales, temblor, vértigo, debilidad, espasmos musculares dolorosos, estreñimiento, disfun¬ciones urinarias y sexuales, fatigabilidad y dolores inespecíficos y múltiples, que sumados al curso crónico y fluctuante requieren un estudio juicioso (31,32). Dentro de su abordaje en el diagnóstico diferencial son especialmente útiles una imagen cerebral y medular por RNM, siendo la más sensible; estudio del líquido cefalorraquídeo en busca de inflamación, y los potenciales evocados visuales en los casos que lo ameriten (33).
Por la misma línea de las dos entidades anteriores, la sífilis es una infección que puede tener compromiso de múltiples sistemas, con curso crónico y fluctuante. De acuerdo al órgano comprometido, las manifestaciones pueden ir desde cambios en el estado de ánimo y deterioro cognitivo, pasando por cefalea, parálisis de grupos musculares, alteraciones sensitivas, ataxia y afasias, hasta disfunciones urinarias, fecales, sexuales y dolor abdominal, rectal, vaginal, laríngeo, entre otros órganos. A diferencia del LES y la EM, su estudio inicial basta con la realización de serología (VDRL), un examen de bajo costo y fácil accesibilidad (34).
Son especialmente frecuentes las manifestaciones cutáneas de somatización, representadas en síndromes inexplicables dados por disestesias, dolor, anestesia y prurito. También surgen episodios pruriginosos locales o generalizados, urticaria, angioedema, enrojecimiento, sudoración profusa, lesiones autoinducidas de forma inconsciente como dermatosis artefactas y tricotilo¬manía, además de las preocupaciones alrededor del cabello y la piel, características del trastorno dismórfico corporal (35). Los síntomas gastrointestinales de mayor frecuencia de presentación en estos pacientes son dolor y distensión abdominales, diarrea, estreñimiento, gastralgia, náuseas y vómito, característicamente acompañados con cefalea, dolor torácico inespecífico, fatiga, síntomas ginecoló¬gicos y sexuales. Por lo tanto, es indispensable descartar la presencia de síndrome de intestino irritable, colitis, enfermedad acidopéptica, intolerancia alimentaria y patología en órganos reproductivos y urinarios vecinos (36).
Los carcinoides son tumores neuroendocrinos que se pueden originar en los bronquios, islotes pancreáticos y retroperitoneo, generalmente son de crecimiento lento y poco agresivo en sus inicios (37). Una característica especial que poseen es su capacidad para producir ciertos péptidos y hormonas como serotonina, histamina, hormona adenocorticótropa, péptido intestinal vasoactivo, insulina, glucagón y calcitonina, por lo que generan síndromes neuroendocrinos (38). Los síntomas clínicos van desde los locales por obstrucción de conductos o metástasis hepáticas, hasta rubor, diarrea, broncoespasmos e hipotensión, pasando por episodios de síncope, confusión, convulsiones, diaforesis, taquicardia y palpitaciones de acuerdo a las hormonas que produzcan de forma predominante (39). Ante la sospecha se deben medir los niveles de péptidos que posiblemente expliquen los síntomas y realizar una exploración imagenográfica de los lugares donde más frecuentemente se desarrollan (40).
En el caso de la porfiria intermitente aguda se pueden precipitar ataques debido a muchos factores incluyendo el medio ambiente, la privación de calorías, sustancias psicoactivas, hormonas esteroideas; crisis que generalmente comienzan con dolor abdominal y progresan con neuropatía periférica, presentando inicialmente dolor, debilidad, más comúnmente en los brazos. De Siervi y cols. encontraron en Argentina que el síntoma inicial es el dolor abdominal en el 100 por ciento de los casos (n = 240), a menudo acompañado de estreñimiento (37%), anorexia (37%) y taquicardia (30%). También se halló que el estrés se constituye en un factor precipitante. Dentro de los medicamentos que comúnmente precipitan la crisis están: eritromicina, sulfona¬midas, barbitúricos, benzodiacepinas, anticonvul¬sivantes, antihistamínicos y diuréticos (41).
Nordmann y Puy observaron, que en el 20 al 30 por ciento de los pacientes se presentan signos de perturbación mental tales como ansiedad, depresión, desorientación, alucinaciones y estados confusionales. Un signo que puede ayudar al médico junto con los síntomas descritos, principalmente dolor abdominal severo asociado a un cuadro de psicosis sin antecedentes psiquiátricos en la persona afectada, permite sospechar la presencia de un ataque agudo de porfiria, cuando aparece orina de color rojo o intensamente oscura, por lo general se presenta después de la exposición de la muestra a la luz y el aire (42).
Las enfermedades endocrinas se constituyen también en patologías que pueden presentar cuadros con múltiples síntomas. La hipocalcemia crónica se manifiesta a través de apatía, estupor, depresión, así como cambios cutáneos, alopecia, piel seca, onicorexis e hiperexitabilidad muscular. En ocasiones se manifiesta como un síndrome digestivo con náuseas, vómitos, úlcera péptica, pancreatitis y un síndrome nefrológico con poliuria, nefrolitiasis, calcinosis, hipertensión arterial, calcificaciones metastásicas, querato¬patía en banda o conjuntivitis cálcica.
En el caso del hipoparatiroidismo ayuda para hacer el diagnóstico tener en cuenta que las convulsiones ya sean focales o generalizadas se constituyen en el síntoma de presentación más frecuente en pacientes jóvenes; pero ha dee tenerse en cuenta que en muchas ocasiones no se encuentra aura, inconsciencia, trauma involuntario ni incontinencia de esfínteres, lo que podría llevar a los médicos a sospechar pseudocrisis y desviarse en el diagnóstico hacia somatización, más si se tiene en cuenta que el ataque podría estar precipitado por perturbaciones emocionales. La administración de calcio mejora los síntomas en esta entidad a diferencia de los anticonvulsivantes que suelen no ser efectivos (43).
En el hiperparatiroidismo Lundgren, y cols. encontraron que de 405 pacientes, el 4,2 por ciento presentaron síntomas mentales que van desde dolores y molestias vagas, pasando por fatiga y apatía, hasta llegar a marcada depresión, psicosis, delirium y coma, siendo en muchos pacientes la fatiga un síntoma clave en el diagnóstico (44). Los principales síntomas son: cálculos renales; debilidad y dolor en músculos, huesos y articulaciones; aumento de fatiga; pérdida de energía durante el día; depresión y fallas de memoria.
La neurocisticercosis se presenta con un cuadro clínico variable, aunque la amplia gama de signos y síntomas producidos se pueden agrupar en tres clases principales: convulsiones, hipertensión intracraneal y síntomas psiquiátricos. El diagnóstico es difícil y requiere de varios procedimientos. Una evaluación clínica junto con la adecuada interpretación de neuroima¬gen y las pruebas inmunológicas son esenciales para el diagnóstico y el tratamiento adecuado (45).
La hemocromatosis es una enfermedad hereditaria que afecta al metabolismo del hierro provocando un acúmulo excesivo e incorrecto de este metal en los órganos y sistemas del organismo. Semeja al trastorno de somatización por sus síntomas inespecíficos en varios órganos y sistemas además de su curso crónico. Dentro de sus manifestaciones tempranas más comunes se encuentran fatiga, debilidad, pérdida de peso, dolor abdominal y artralgias. Luego aparecen disnea y síntomas de falla gonadal como amenorrea, menopausia precoz, disminución de la libido e impotencia. Por último, se desarrollan fallas graves en diferentes órganos que llevan a la muerte. El abordaje inicial de pacientes en quienes se sospecha esta entidad se hace solicitando niveles séricos de hierro que luego se complementan con otros estudios según el caso (46).
La miastenia gravis es una enfermedad neuromuscular autoinmune y crónica caracterizada por grados variables de debilidad de los músculos esqueléticos. Debuta con un cuadro insidioso de pérdida de fuerzas, que rápidamente se recuperan con el descanso pero que reaparece al reiniciar el ejercicio. Suele iniciarse en los músculos perioculares. Inicialmente el paciente refiere fatigabilidad y debilidad, pero en los casos en donde ocurre progresión craneocaudal pueden aparecer disfonía, disfagia y disnea. En los pacientes en los que se sospeche, aparte de las pruebas clínicas, se puede realizar el test de edrofonio y solicitar anticuerpos contra el receptor de acetilcolina (47).
La enfermedad de Addison es una deficiencia hormonal causada por daño a la glándula adrenal, lo cual ocasiona una hipofunción o insuficiencia corticosuprarrenal primaria. Sus manifestaciones son inespecíficas y su curso es crónico. Se caracteriza por astenia y debilidad, hiperpigmen¬tación cutánea y de mucosas, pérdida de peso, síntomas gastrointestinales, hipotensión arterial, cambios perceptivos, inquietud e irritabilidad excesivas, pérdida de vello e hipertermia. Las pruebas diagnósticas iniciales están encaminadas a la búsqueda de hiponatremia, hiperkalemia e hipocortisolemia (48).
El hipertiroidismo es una patología causada por la hipersecreción de hormonas tiroideas, dando lugar a niveles plasmáticos anormalmente elevados. Las principales causas en los seres humanos son la enfermedad de Graves o bocio tóxico difuso como más frecuente, el adenoma tiroideo tóxico, el bocio multinodular tóxico y la tiroiditis subaguda. Se diferencia del síndrome de tirotoxicosis o tormenta tiroidea porque en este último hay un aumento simplemente de la concentración plasmática de hormonas tiroideas, mientras que el hipertiroidismo es una enfermedad donde prevalece aumentada la síntesis de estas hormonas.
Las principales características clínicas son pérdida de peso, hiperfagia, dolor o calambres intestinales, mayor número de deposiciones diarias o diarrea, náuseas, vómitos, diaforesis, intolerancia al calor, pelo fino y quebradizo, aumento de la pigmentación, fatiga, debilidad muscular, temblor, taquicardia, palpitaciones, hipertensión sistólica, disnea de esfuerzo, oligorrea o amenorrea, disminución de la libido, exoftalmos, retracción del párpado superior, edema periorbitario, diplopía, enrojecimiento de la conjuntiva y además síntomas psicológicos dados por ansiedad, nerviosismo, irritabilidad, insomnio, despertar precoz, problemas de concentración y disminución del umbral del estrés. Para su diagnóstico basta la medición de los niveles plasmáticos de T4 libre, que se pueden complementar con la medición de la hormona estimulante de tiroides (TSH) (49).
El hipotiroidismo es la disminución de los niveles de hormonas tiroideas en plasma sanguíneo y consecuentemente en tejidos, puede ser asintomática u ocasionar múltiples síntomas y signos inespecíficos en el organismo. Los pacientes en ocasiones, por su presentación larvada, pueden recibir tratamiento psiquiátrico o psicológico cuando en realidad lo que necesitan es tratamiento hormonal de sustitución. No es fácil de diagnosticar en sus estados iniciales. Dentro de los hallazgos clínicos se encuentran ptosis palpebral, edema periorbitario, voz ronca, caída del pelo de la cola de las cejas, disminución de la capacidad vital forzada en la espirometría, bradicardia, hiporexia, pesadez abdominal, estreñimiento, meteorismo, cefalea e hiporreflexia.
En mujeres existen ciclos anovulatorios con hipermenorrea y abortos. En los hombres produce impotencia y disminución de la libido. Dentro de las manifestaciones neuropsiquiátricas están: enlentecimiento de la función intelectual, bradipsiquia, bradilalia, abulia, somnolencia, apatía y trastornos psiquiátricos como psicosis, depresión y retraso mental. Para su diagnóstico se requiere de la medición de los niveles de TSH y hormonas tiroideas (49).
También es importante hacer diferenciación con otros trastornos psiquiátricos que se asemejan al de somatización. En la hipocondría predomina el miedo o convicción a padecer una enfermedad a partir de la interpretación de síntomas somáticos. En el trastorno de conversión los síntomas son sólo neurológicos de aparición aguda y rápida resolución. En el trastorno delirante somático los síntomas son limitados en número y generalmente involucran un solo sistema. En trastornos ansiosos y depresivos el eje de la sintomatología está en la esfera afectiva y las manifestaciones somáticas son accesorias a éste (1, 50).
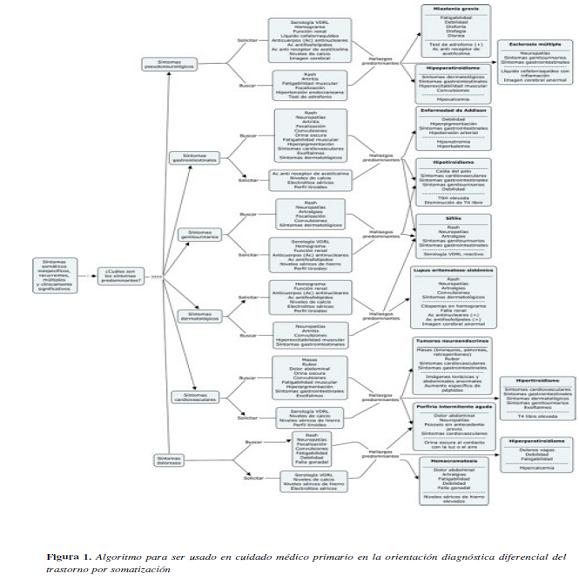
Finalmente se propone el siguiente algoritmo Figura 1 para ser usado en cuidado médico primario en la orientación diagnóstica diferencial del trastorno de somatización y de esta forma permitirle al médico no especialista en psiquiatría un abordaje integral, evitando procedimientos y pruebas paraclínicas innecesarias y llevando a cabo un tratamiento adecuado.
Conclusiones
Este artículo permite determinar el diagnóstico diferencial del trastorno por somatización en cuidado médico primario y el algoritmo propuesto para su abordaje orienta al médico no especialista en psiquiatría en el diagnóstico temprano y oportuno de esta entidad psiquiátrica frecuentemente encontrada y subtratada. Al médico de atención primaria el algoritmo propuesto le permite guiar al paciente en la consecución de un tratamiento integral, evitando complicaciones asociadas a la práctica de procedimientos y exámenes de laboratorio innecesarios.
Referencias
1. López-Ibor J, Valdés M. Manual diagnóstico y estadístico de los trastornos mentales. Texto revisado. 2002.
2. Bombana J. Síntomas somáticos inexplicados clinicamente: um campo impreciso entre a psiquiatria e a clínica médica. J. bras. psiquiatr. 2006; 55: 308-312.
3. Schweickhardt A, Larisch A, Fritzsche K. Differentiation of somatizing patients in primary care: why the effects of treatment are always moderate. J Nerv Ment Dis. 2005; 193: 813-9.
4. Lipkowski Z. Somatization: the concept and its clinical application. Am J Psychiatry 1988; 145:1358-1368
5. McWhinney IR, Epstein RM, Freeman TR: Rethinking somatization. Adv Mind Body Med 2001; 17: 232-9.
6. Chandrashekar CR, Math SB. Psychosomatic disorders in developing countries: current issues and future challenges. Curr Opin Psychiatry 2006; 19: 201-6.
7. Kanaan RA, Lepine JP, Wessely SC. The association or otherwise of the functional somatic syndromes. Psychosom Med. 2007; 69: 855-9.
8. Heinrich TW. Medically unexplained symptoms and the concept of somatization. Wmj. 2004; 103: 83-7.
9. Huapaya LV. Psychogenesis and somatogenesis of common symptoms. Can Med Assoc J. 1975; 112: 1109-13.
10. Jyvasjarvi S, Joukamaa M, Vaisanen E, Larivaara P, Kivela S, Keinanen-Kiukaanniemi S. Somatizing frequent attenders in primary health care. J Psychosom Res. 2001; 50: 185-92.
11. Lloyd G. Medicine without signs. Br Med J (Clin Res Ed). 1983; 287(6391): 539-42
12. Rief W, Rojas G. Stability of somatoform symptomsimplications for classification. Psychosom Med. 2007; 69: 864-9.
13. Richardson RD, Engel CC, Jr. Evaluation and management of medically unexplained physical symptoms. Neurologist. 2004; 10: 18-30.
14. Escobar JI, Hoyos-Nervi C, Gara M. Medically unexplained physical symptoms in medical practice: a psychiatric perspective. Environ Health Perspect. 2002; 110 Suppl 4: 631-6
15. Smith RC, Dwamena FC. Classification and diagnosis of patients with medically unexplained symptoms. J Gen Intern Med. 2007; 22: 685-91.
16. Sumathipala A, Siribaddana S, Hewege S, Sumathipala K, Prince M, Mann A. Understanding the explanatory model of the patient on their medically unexplained symptoms and its implication on treatment development research: a Sri Lanka Study. BMC Psychiatry. 2008; 8: 54.
17. Servan-Schreiber D, Kolb NR, Tabas G. Somatizing patients: Part I. Practical diagnosis. Am Fam Physician. 2000; 61: 1073-8.
18. Uribe R. Modelos conceptuales en medicina psicosomática. rev.colomb.psiquiatr. 2006; XXXV: 7-20
19. Hakala M, Karlsson H, Kurki T, Aalto S, Koponen S, Vahlberg T, Niemi PM. Volumes of the caudate nuclei in women with somatization disorder and healthy women. Psychiatry Res. 2004; 131: 71-8.
20. Lowe B, Spitzer RL, Williams JB, Mussell M, Schellberg D, Kroenke K. Depression, anxiety and somatization in primary care: syndrome overlap and functional impairment. Gen Hosp Psychiatry. 2008; 30: 191-9.
21. Fink P, Toft T, Hansen MS, Ornbol E, Olesen F. Symptoms and syndromes of bodily distress: an exploratory study of 978 internal medical, neurological, and primary care patients. Psychosom Med. 2007; 69: 30-9.
22. Cabot R. Suggestions for reorganisation of hospital outpatient departments with special reference to improvement of treatment. Md State MedJ. 1907; 50: 81-91.
23. Nimnuan C, Hotopf M, Wessely S. Medically unexplained symptoms: an epidemiological study in seven specialities. J Psychosom Res. 2001; 51: 361-7.
24. Robins LN, Price RK. Adult disorders predicted by childhood conduct problems: results from the NIMH Epidemiologic Catchment Area project. Psychiatry. 1991; 54: 116-32.
25. Karvonen JT, Veijola J, Jokelainen J, Laksy K, Jarvelin MR, Joukamaa M. Somatization disorder in young adult population. Gen Hosp Psychiatry. 2004; 26: 9-12.
26. Kroenke K, Spitzer RL, Williams JB, Linzer M, Hahn SR, deGruy FV, 3rd, Brody D. Physical symptoms in primary care. Predictors of psychiatric disorders and functional impairment. Arch Fam Med. 1994; 3: 774-9.
27. Rasmussen NH, Bernard ME, Harmsen WS. Physical symptoms that predict psychiatric disorders in rural primary care adults. J Eval Clin Pract. 2008; 14: 399-406.
28. Coelho L, ávila A. Controvérsias sobre a somatização. Rev. psiquiatr. clín. 2007; 34: 278-284.
29. Vadacca M, Buzzulini F, Rigon A, Coppolino G, Palma Modoni A, Massa R, Afeltra A. [Neuropsychiatric lupus erythematosus]. Reumatismo 2006; 58: 177-86.
30. Ferreira S, D'Cruz DP, Hughes GR. Multiple sclerosis, neuropsychiatric lupus and antiphospholipid syndrome: where do we stand? Rheumatology (Oxford) 2005; 44:434-42.
31. Compston A, Coles A. Multiple sclerosis. Lancet 2002; 359: 1221-31.
32. Miller D, Barkhof F, Montalban X, Thompson A, Filippi M. Clinically isolated syndromes suggestive of multiple sclerosis, part I: natural history, pathogenesis, diagnosis, and prognosis. Lancet Neurol. 2005; 4: 281-8.
33. Poser CM, Brinar VV. Diagnostic criteria for multiple sclerosis. Clin Neurol Neurosurg. 2001; 103: 1-11.
34. Hutto B. Syphilis in clinical psychiatry: a review. Psychosomatics 2001; 42: 453-60.
35. Gupta MA. Somatization disorders in dermatology. Int Rev Psychiatry. 2006; 18: 41-7.
36. Bass C, Bond A, Gill D, Sharpe M. Frequent attenders without organic disease in a gastroenterology clinic. Patient characteristics and health care use. Gen Hosp Psychiatry. 1999; 21: 30-8.
37. Granberg D, Oberg K. Neuroendocrine tumours. Cancer Chemother Biol Response Modif. 2005; 22: 471-83.
38. Toth M, Pronai L, Nemeth AM, Tulassay Z. [Carcinoid tumors]. Orv Hetil 2002; 143(19 Suppl):1087-92.
39. Lips CJ, Lentjes EG, Hoppener JW. The spectrum of carcinoid tumours and carcinoid syndromes. Ann Clin Biochem. 2003; 40 (Pt 6): 612-27.
40. Ruszniewski P, O'Toole D. [Clinical spectrum of digestive neuroendocrine tumors]. Rev Prat 2002; 52: 262-7.
41. De Siervi A, Rossetti MV, Parera VE, Mendez M, Varela LS, del CBAM. Acute intermittent porphyria: biochemical and clinical analysis in the Argentinean population. Clin Chim Acta. 1999; 288: 63-71.
42. Nordmann Y, Puy H. Human hereditary hepatic porphyrias. Clin Chim Acta. 2002; 325: 17-37.
43. Monneuse O, Causeret S, Lifante JC, Berger N, Lapras V, Peix JL. [Primary juvenile hyperparathyroidism. Report of 24 cases]. Ann Chir. 2002; 127: 276-80.
44. Lundgren E, Ljunghall S, Akerstrom G, Hetta J, Mallmin H, Rastad J. Case-control study on symptoms and signs of «asymptomatic» primary hyperparathyroidism. Surgery. 1998; 124: 980-5; discussion 985-6.
45. Meza NW, Rossi NE, Galeazzi TN, Sanchez NM, Colmenares FI, Medina OD, et al. Cysticercosis in chronic psychiatric inpatients from a Venezuelan community. Am J Trop Med Hyg. 2005; 73: 504-9.
46. Reyes M, Blanck HM, Grossniklaus D. Hemochromatosis: What every clinician and health care professional needs to know. Department of Health and Human Services Centers for Disease Control and Prevention. 2002; 1: 1-98.
47. Turner C. A review of myasthenia gravis: Pathogenesis, clinical features and treatment. Current Anaesthesia & Critical Care. 2007; 18: 15-23.
48. Anglin RE, Rosebush PI, Mazurek MF. The neuropsychiatric profile of Addison's disease: revisiting a forgotten phenomenon. J Neuropsychiatry Clin Neurosci. 2006; 18: 450-9.
49. Attia J, Margetts P, Guyatt G. Diagnosis of thyroid disease in hospitalized patients: a systematic review. Arch Intern Med. 1999; 159: 658-65.
50. Caixeta M, Chaves M, Reis OR. [Organic somatoform disorder. Case report]. Arq Neuropsiquiatr. 1999; 57: 120-5.
Referencias
López-Ibor J, Valdés M. Manual diagnóstico y estadístico de los trastornos mentales. Texto revisado. 2002.
Bombana J. Síntomas somáticos inexplicados clinicamente: um campo impreciso entre a psiquiatria e a clínica médica. J. bras. psiquiatr. 2006; 55: 308-312.
Schweickhardt A, Larisch A, Fritzsche K. Differentiation of somatizing patients in primary care: why the effects of treatment are always moderate. J Nerv Ment Dis. 2005; 193: 813-9.
Lipkowski Z. Somatization: the concept and its clinical application. Am J Psychiatry 1988; 145:1358-1368
McWhinney IR, Epstein RM, Freeman TR: Rethinking somatization. Adv Mind Body Med 2001; 17: 232-9.
Chandrashekar CR, Math SB. Psychosomatic disorders in developing countries: current issues and future challenges. Curr Opin Psychiatry 2006; 19: 201-6.
Kanaan RA, Lepine JP, Wessely SC. The association or otherwise of the functional somatic syndromes. Psychosom Med. 2007; 69: 855-9.
Heinrich TW. Medically unexplained symptoms and the concept of somatization. Wmj. 2004; 103: 83-7.
Huapaya LV. Psychogenesis and somatogenesis of common symptoms. Can Med Assoc J. 1975; 112: 1109-13.
Jyvasjarvi S, Joukamaa M, Vaisanen E, Larivaara P, Kivela S, Keinanen-Kiukaanniemi S. Somatizing frequent attenders in primary health care. J Psychosom Res. 2001; 50: 185-92.
Lloyd G. Medicine without signs. Br Med J (Clin Res Ed). 1983; 287(6391): 539-42
Rief W, Rojas G. Stability of somatoform symptoms—implications for classification. Psychosom Med. 2007; 69: 864-9.
Richardson RD, Engel CC, Jr. Evaluation and management of medically unexplained physical symptoms. Neurologist. 2004; 10: 18-30.
Escobar JI, Hoyos-Nervi C, Gara M. Medically unexplained physical symptoms in medical practice: a psychiatric perspective. Environ Health Perspect. 2002; 110 Suppl 4: 631-6
Smith RC, Dwamena FC. Classification and diagnosis of patients with medically unexplained symptoms. J Gen Intern Med. 2007; 22: 685-91.
Sumathipala A, Siribaddana S, Hewege S, Sumathipala K, Prince M, Mann A. Understanding the explanatory model of the patient on their medically unexplained symptoms and its implication on treatment development research: a Sri Lanka Study. BMC Psychiatry. 2008; 8: 54.
Servan-Schreiber D, Kolb NR, Tabas G. Somatizing patients: Part I. Practical diagnosis. Am Fam Physician. 2000; 61: 1073-8.
Uribe R. Modelos conceptuales en medicina psicosomática. rev.colomb.psiquiatr. 2006; XXXV: 7-20
Hakala M, Karlsson H, Kurki T, Aalto S, Koponen S, Vahlberg T, Niemi PM. Volumes of the caudate nuclei in women with somatization disorder and healthy women. Psychiatry Res. 2004; 131: 71-8.
Lowe B, Spitzer RL, Williams JB, Mussell M, Schellberg D, Kroenke K. Depression, anxiety and somatization in primary care: syndrome overlap and functional impairment. Gen Hosp Psychiatry. 2008; 30: 191-9.
Fink P, Toft T, Hansen MS, Ornbol E, Olesen F. Symptoms and syndromes of bodily distress: an exploratory study of 978 internal medical, neurological, and primary care patients. Psychosom Med. 2007; 69: 30-9.
Cabot R. Suggestions for reorganisation of hospital outpatient departments with special reference to improvement of treatment. Md State MedJ. 1907; 50: 81-91.
Nimnuan C, Hotopf M, Wessely S. Medically unexplained symptoms: an epidemiological study in seven specialities. J Psychosom Res. 2001; 51: 361-7.
Robins LN, Price RK. Adult disorders predicted by childhood conduct problems: results from the NIMH Epidemiologic Catchment Area project. Psychiatry. 1991; 54: 116-32.
Karvonen JT, Veijola J, Jokelainen J, Laksy K, Jarvelin MR, Joukamaa M. Somatization disorder in young adult population. Gen Hosp Psychiatry. 2004; 26: 9-12.
Kroenke K, Spitzer RL, Williams JB, Linzer M, Hahn SR, deGruy FV, 3rd, Brody D. Physical symptoms in primary care. Predictors of psychiatric disorders and functional impairment. Arch Fam Med. 1994; 3: 774-9.
Rasmussen NH, Bernard ME, Harmsen WS. Physical symptoms that predict psychiatric disorders in rural primary care adults. J Eval Clin Pract. 2008; 14: 399-406.
Coelho L, ávila A. Controvérsias sobre a somatização. Rev. psiquiatr. clín. 2007; 34: 278-284.
Vadacca M, Buzzulini F, Rigon A, Coppolino G, Palma Modoni A, Massa R, Afeltra A. [Neuropsychiatric lupus erythematosus]. Reumatismo 2006; 58: 177-86.
Ferreira S, D'Cruz DP, Hughes GR. Multiple sclerosis, neuropsychiatric lupus and antiphospholipid syndrome: where do we stand? Rheumatology (Oxford) 2005; 44:434-42.
Compston A, Coles A. Multiple sclerosis. Lancet 2002; 359: 1221-31.
Miller D, Barkhof F, Montalban X, Thompson A, Filippi M. Clinically isolated syndromes suggestive of multiple sclerosis, part I: natural history, pathogenesis, diagnosis, and prognosis. Lancet Neurol. 2005; 4: 281-8.
Poser CM, Brinar VV. Diagnostic criteria for multiple sclerosis. Clin Neurol Neurosurg. 2001; 103: 1-11.
Hutto B. Syphilis in clinical psychiatry: a review. Psychosomatics 2001; 42: 453-60.
Gupta MA. Somatization disorders in dermatology. Int Rev Psychiatry. 2006; 18: 41-7.
Bass C, Bond A, Gill D, Sharpe M. Frequent attenders without organic disease in a gastroenterology clinic. Patient characteristics and health care use. Gen Hosp Psychiatry. 1999; 21: 30-8.
Granberg D, Oberg K. Neuroendocrine tumours. Cancer Chemother Biol Response Modif. 2005; 22: 471-83.
Toth M, Pronai L, Nemeth AM, Tulassay Z. [Carcinoid tumors]. Orv Hetil 2002; 143(19 Suppl):1087-92.
Lips CJ, Lentjes EG, Hoppener JW. The spectrum of carcinoid tumours and carcinoid syndromes. Ann Clin Biochem. 2003; 40 (Pt 6): 612-27.
Ruszniewski P, O'Toole D. [Clinical spectrum of digestive neuroendocrine tumors]. Rev Prat 2002; 52: 262-7.
De Siervi A, Rossetti MV, Parera VE, Mendez M, Varela LS, del CBAM. Acute intermittent porphyria: biochemical and clinical analysis in the Argentinean population. Clin Chim Acta. 1999; 288: 63-71.
Nordmann Y, Puy H. Human hereditary hepatic porphyrias. Clin Chim Acta. 2002; 325: 17-37.
Monneuse O, Causeret S, Lifante JC, Berger N, Lapras V, Peix JL. [Primary juvenile hyperparathyroidism. Report of 24 cases]. Ann Chir. 2002; 127: 276-80.
Lundgren E, Ljunghall S, Akerstrom G, Hetta J, Mallmin H, Rastad J. Case-control study on symptoms and signs of «asymptomatic» primary hyperparathyroidism. Surgery. 1998; 124: 980-5; discussion 985-6.
Meza NW, Rossi NE, Galeazzi TN, Sanchez NM, Colmenares FI, Medina OD, et al. Cysticercosis in chronic psychiatric inpatients from a Venezuelan community. Am J Trop Med Hyg. 2005; 73: 504-9.
Reyes M, Blanck HM, Grossniklaus D. Hemochromatosis: What every clinician and health care professional needs to know. Department of Health and Human Services Centers for Disease Control and Prevention. 2002; 1: 1-98.
Turner C. A review of myasthenia gravis: Pathogenesis, clinical features and treatment. Current Anaesthesia & Critical Care. 2007; 18: 15-23.
Anglin RE, Rosebush PI, Mazurek MF. The neuropsychiatric profile of Addison's disease: revisiting a forgotten phenomenon. J Neuropsychiatry Clin Neurosci. 2006; 18: 450-9.
Attia J, Margetts P, Guyatt G. Diagnosis of thyroid disease in hospitalized patients: a systematic review. Arch Intern Med. 1999; 159: 658-65.
Caixeta M, Chaves M, Reis OR. [Organic somatoform disorder. Case report]. Arq Neuropsiquiatr. 1999; 57: 120-5.
Cómo citar
APA
ACM
ACS
ABNT
Chicago
Harvard
IEEE
MLA
Turabian
Vancouver
Descargar cita
Visitas a la página del resumen del artículo
Descargas
Licencia
Derechos de autor 2009 Revista de la Facultad de Medicina

Esta obra está bajo una licencia Creative Commons Reconocimiento 3.0 Unported.
-


















