


Publicado
¿Por qué no se mejoran los niños con trastornos por déficit de atención con hiperactividad?
¿Why don´t inprove children with attention-deficit and hyperactivity disorder?
Palabras clave:
trastorno deficitario de atención con hiperactividad, psiquiatría infantil, estudios de seguimiento, prescripción de medicamentos (es)attention deficit disorder with hyperactivity, child psychiatry, follow-up studies, prescriptions, drug (en)
Introducción. Durante el año 2004, en consulta externa e interconsultas del servicio de psiquiatría infantil, se hicieron 1454 valoraciones, correspondientes a 592 pacientes. De éstas, 536 fueron por trastorno deficitario de atención con hiperactividad (TDAH), correspondientes a 240 pacientes. Se preguntó al paciente y familiares si la condición que motivó la consulta se encontraba mejor, peor o igual. Según el registro en el sistema, 76% estaban igual o peor; 23% mejor y 1% no contestó. Se hizo el estudio para determinar qué sucedió con aquellos cuyos registros estadísticos no mostraban mejoría.
Objetivo. Caracterizar los pacientes que asistieron a la consulta de psiquiatría infantil en quienes se hizo diagnóstico de TDAH y no reportaron mejoría clínica.
Material y métodos. Revisión de historias clínicas y entrevista personal con pacientes que consultaron al servicio de psiquiatría del Hospital Pediátrico de la Misericordia durante 2004 en quienes se hizo diagnóstico de TDAH y no reportaron mejoría clínica.
Resultados. En 237 pacientes con sospecha de TDAH se confirmó el diagnóstico en 157 (66.2%); se inició tratamiento a 114 (48.1%). Tras seguimiento, se encontró que 94 mejoraron y 20 lo abandonaron; tres expusieron sus motivos.
Conclusiones. Como informa la literatura internacional, se logró mejoría clínica en 82.45%. En quienes no mejoran se encuentran múltiples razones para explicar el abandono del tratamiento.
Background. During the year 2004, 1454 evaluations, corresponding to 592 patients, were made in outward and inter consultation. Out of these evaluations, 536 were because of ADD, corresponding to 240 patients. We asked the patients and their families whether, the children's condition that brought them to consultation had improved, was worse or the same. According to the registration system, 76% were the same or worse, 23% were better and 1% did not answer. We made a study in order to determine what had happened to the patients whose statistic registration showed no improvement. Objective. Characterizing the patients who came to consultation at the Children's Psychiatric consultation in the Hospital de la Misericordia during 2004 and who were diagnosed as ADD not reporting clinical improvement.
Material and methods. Patients who came to consultation at the Pediatric Psychiatric service of the Hospital de la Misericordia during the year 2004, who were diagnosed as ADD and did not report clinical improvement.
Results. In 237 patients suspicious of having ADD was confirmed in 157 patients (66%). Treatment was begun in 114 (48%). In the follow up studies, it was found that 94 improved, 20 abandoned the treatment; of these, three let give us their motivation.
Conclusions. We found mistakes in the patients' registration, specifically in the improvement indicator, and that frequently it was not possible to confirm diagnosis, nor initiate treatments, because the patients did not come back after the first consultation or abandoned the treatment.
As reported by international literature, there was 82.45% clinical improvement. Multiple reasons were found to explain abandonment of the treatment.
INVESTIGACIÓN ORIGINAL
Heydy Luz Chica Úrzola1, Rafael Vásquez2
1.Residente de III Año de Psiquiatría, Facultad de Medicina, Universidad Nacional de Colombia. Bogotá.
2.Psiquiatra de niños y adolescentes. Profesor Titular de Psiquiatría, Facultad de Medicina. Universidad Nacional de Colombia, Bogotá.
Correspondencia:heluchi@aemail4u.com
Resumen
Introducción. Durante el año 2004, en consulta externa e interconsultas del servicio de psiquiatría infantil, se hicieron 1454 valoraciones, correspondientes a 592 pacientes. De éstas, 536 fueron por trastorno deficitario de atención con hiperactividad (TDAH), correspondientes a 240 pacientes. Se preguntó al paciente y familiares si la condición que motivó la consulta se encontraba mejor, peor o igual. Según el registro en el sistema, 76% estaban igual o peor; 23% mejor y 1% no contestó. Se hizo el estudio para determinar qué sucedió con aquellos cuyos registros estadísticos no mostraban mejoría.
Objetivo. Caracterizar los pacientes que asistieron a la consulta de psiquiatría infantil en quienes se hizo diagnóstico de TDAH y no reportaron mejoría clínica.
Material y métodos. Revisión de historias clínicas y entrevista personal con pacientes que consultaron al servicio de psiquiatría del Hospital Pediátrico de la Misericordia durante 2004 en quienes se hizo diagnóstico de TDAH y no reportaron mejoría clínica.
Resultados. En 237 pacientes con sospecha de TDAH se confirmó el diagnóstico en 157 (66.2%); se inició tratamiento a 114 (48.1%). Tras seguimiento, se encontró que 94 mejoraron y 20 lo abandonaron; tres expusieron sus motivos.
Conclusiones. Como informa la literatura internacional, se logró mejoría clínica en 82.45%. En quienes no mejoran se encuentran múltiples razones para explicar el abandono del tratamiento.
Palabras clave: trastorno deficitario de atención con hiperactividad, psiquiatría infantil, estudios de seguimiento, prescripción de medicamentos.
Summary
Background. During the year 2004, 1454 evaluations, corresponding to 592 patients, were made in outward and inter consultation. Out of these evaluations, 536 were because of ADD, corresponding to 240 patients. We asked the patients and their families whether, the children's condition that brought them to consultation had improved, was worse or the same. According to the registration system, 76% were the same or worse, 23% were better and 1% did not answer. We made a study in order to determine what had happened to the patients whose statistic registration showed no improvement. Objective. Characterizing the patients who came to consultation at the Children's Psychiatric consultation in the Hospital de la Misericordia during 2004 and who were diagnosed as ADD not reporting clinical improvement.
Material and methods. Patients who came to consultation at the Pediatric Psychiatric service of the Hospital de la Misericordia during the year 2004, who were diagnosed as ADD and did not report clinical improvement.
Results. In 237 patients suspicious of having ADD was confirmed in 157 patients (66%). Treatment was begun in 114 (48%). In the follow up studies, it was found that 94 improved, 20 abandoned the treatment; of these, three let give us their motivation.
Conclusions. We found mistakes in the patients' registration, specifically in the improvement indicator, and that frequently it was not possible to confirm diagnosis, nor initiate treatments, because the patients did not come back after the first consultation or abandoned the treatment.
As reported by international literature, there was 82.45% clinical improvement. Multiple reasons were found to explain abandonment of the treatment.
Key words: attention deficit disorder with hyperactivity, child psychiatry, follow-up studies, prescriptions, drug.
Introducción
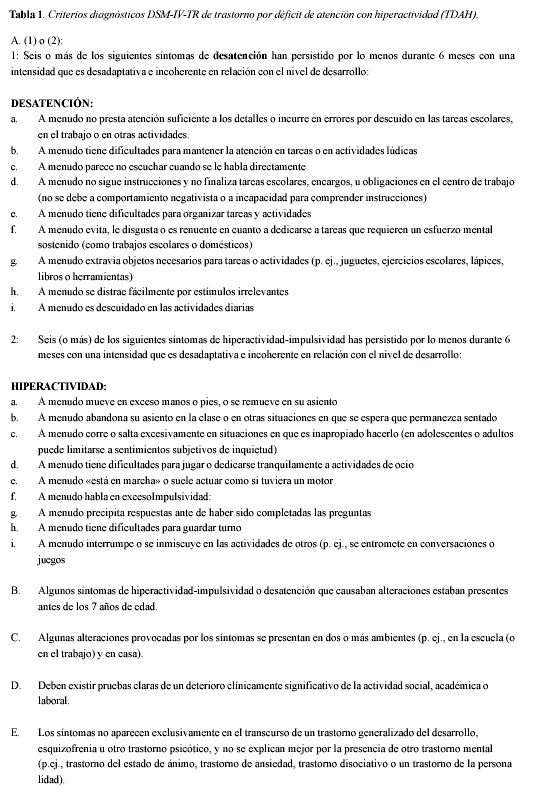
El trastorno por déficit de atención con hiperactividad (TDAH) es una condición que comienza en la infancia y se caracteriza por síntomas de desatención e impulsividad-hiperactividad. Se divide en subtipos según el síntoma dominante (1,2) (Tabla 1). Aceptados por clínicos y avalados por la literatura se encuentran disponibles como tratamientos efectivos: los estimulantes del sistema nervioso, la intervensión psicosocial y comportamental en la familia y en las relaciones escolares del paciente y la combinación de ellos (3-9). 50-80% los niños que reciben medicación mejoran según informes en la literatura (10-12). En los demás no se evidencia el efecto terapéutico esperado o se presentan efectos adversos importantes que limitan su utilización. El TDAH es una condición crónica que se complica principalmente por síntomas afectivos y alteraciones de la convivencia que dificultan su tratamiento, si estos no son intervenidos en forma adecuada y oportuna (13-17).
Con frecuencia se llega a estas situaciones al informar a los padres y al paciente respecto a la presencia de una condición psiquiátrica que requiere intervención, noticia recibida con temor, en ocasiones, a menudo negada pero que produce efectos sobre el grupo familiar y el ambiente escolar (18- 19).
Existen estudios que muestran el desenlace, seguimiento y pronóstico de los niños con TDAH, complicado en la mayoría de los casos, relacionado con el abuso de sustancias, efectos adversos a largo
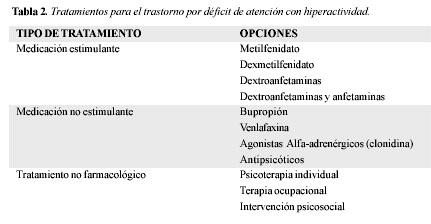
plazo y comorbilidades frecuentes (20-25). Sin embargo no se encuentran estudios que muestren los motivos por los cuales el tratamiento no funciona, pese a hacerse en forma adecuada. En el Hospital Pediátrico de la Misericordia se ofrece un tratamiento integral que abarca el farmacológico y el psicosocial con refuerzo en las áreas de mayor dificultad para los pacientes con TDAH y sus familias (Tabla 2).
Según la información almacenada en el sistema específico de psiquiatría, durante el año 2004 en la consulta externa e interconsultas, se hicieron 1454 valoraciones, correspondientes a 592 pacientes. De las valoraciones realizadas, 536 fueron por TDAH, correspondientes a 240 pacientes.
Como parte rutinaria de la consulta se pregunta al paciente y sus familiares si la condición que motivó la misma se encuentra mejor, peor o igual. Por medio del registro en el sistema específico de psiquiatría se evidenció que 76% estaban igual o peor; el 23% mejor y el 1% no contestó.
Ante este hallazgo y por las obvias divergencias con lo reportado por la literatura mundial en cuanto se refiere a la efectividad del tratamiento, se hizo este estudio para determinar qué sucedió con estos pacientes y caracterizar el grupo de quienes no experimentan mejoría clínica en el curso del tratamiento del TDAH.
Material y métodos
Sujetos. Pacientes que consultaron al Hospital Pediátrico de La Misericordia durante el año 2004, con diagnóstico de trastorno por déficit de atención con hiperactividad, consignados en el sistema específico del servicio de psiquiatría. Métodos. Se hizo un examen del sistema específico del servicio de psiquiatría, se revisaron las historias clínicas de los pacientes y se contactó telefónicamente a aquellos que no reportaron mejoría. Durante las entrevistas con estos pacientes se exploró su estado, el resultado del tratamiento y las razones por las cuales no regresó.
Resultados
Se encontraron registradas en la base de datos 536 valoraciones solicitadas, 384 reportaron encontrarse igual (71,6%); 24 dijeron encontrarse peor (4,47%) y 124 refirieron encontrarse mejor (23,1%), en cuatro casos (0.75%) no se obtuvo información.
Según este informe inicial, estas valoraciones correspondieron a 237 pacientes. En 80 no se confirmó el diagnóstico porque sólo asistieron a la primera consulta. 43 pacientes asistieron a una segunda consulta en la cual se confirmó el diagnóstico, pero no volvieron y no comenzaron tratamiento. Por tanto, 123 pacientes, se excluyeron del estudio por no tener diagnóstico confirmado o no haber iniciado tratamiento.
De 114 pacientes las historias clínicas permitieron apreciar que 86 (75%) estaban mejor, 24 (21%) se encontraban igual, de los cuales cinco no regresaron al tratamiento. Cuatro se encontraban peor 4% y tres no volvieron a la consulta. En los pacientes que no reportaron mejoría (igual o peor) se intentó comunicación telefónica, con el fin de conocer la causa de no mejoría y de deserción de la consulta. En 16 de ellos no fue posible la comunicación telefónica por datos erróneos en las historias clínicas o traslados de los pacientes y sus familias. En un caso se encontró que nunca había asistido a psiquiatría. Ocho se encontraban mejor; dos estaban igual y uno se encontraba peor.
En total se encontró que el 82,45% de los pacientes (94) con diagnóstico confirmado en quienes se inició tratamiento para el TDAH, reportaron mejoría clínica.
En aquellos que no mejoraron, con los cuales se logró establecer comunicación (n=3) se encontró que:
Sujeto 1. Refirió la madre que lo veía igual. 11 años de edad. Convive con los padres. Cursa quinto de primaria. Vive en estrato 3. No se le dio el medicamento. Está en tratamiento en otro sitio para la desatención sin necesidad de usar medicamentos, porque el pediatra les dijo que no los necesitaba y que no expusieran al niño al uso de "esos medicamentos". En el colegio no estaban de acuerdo con que los recibiera. Continúa el mal rendimiento académico y las dificultades en el aula de clase y con los profesores del colegio.
Sujeto 2. Refirió la tía que estaba igual. Nueve años de edad. Convive con la madre y una hermana. Cursa cuarto de primaria. Vive en estrato 2. No recuerdan si alguna vez le fue formulado el medicamento, pero si es así "no le sirvió". El niño considera que para "ser normal" no requiere la toma del medicamento y la madre no se lo administra. No ha mejorado académicamente, tiene pocos amigos.
Sujeto 3. La madre refirió que estaba peor. 12 años de edad. Vive con la mamá y un hermano. Cursa séptimo grado. Vive en estrato 3 en arriendo de una habitación compartida. El padre fue asesinado y el niño se encuentra más agresivo ahora. Le suspendieron la medicación para "ver si es eso lo que lo pone peor". Los compañeros le dicen loco. Recibe un trato despectivo por parte de la orientadora del colegio, quien le dice que "ya le han tenido mucha paciencia", razón por la cual el paciente se rehúsa a tomar el medicamento para no seguir siendo tratado así. La madre considera que las dificultades del niño se derivan de la muerte violenta del padre y no de otra situación.
Discusión
El objetivo central del presente estudio fue determinar las causas por las cuales los niños que asisten a consulta especializada de psiquiatría infantil en el Hospital Pediátrico de la Misericordia, con diagnóstico y tratamiento de TDAH no presentaron mejoría.
Los datos preliminares mostraban, a diferencia de los estudios poblacionales de la literatura mundial, que cerca de dos tercios de los pacientes no obtenían una mejoría en su condición. Ello llamó poderosamente la atención, por lo que se empezó a trabajar en el análisis de los datos que se tenían en ese momento.
Se encontraron grandes problemas en el registro dentro de la base de datos del servicio de psiquiatría infantil, causados principalmente por: las consultas de primera vez eran cualificadas dentro de los indicadores de seguimiento propuestos como "igual", sin tener en ese momento patrones de referencia ni indicadores de logros. Con lo cual el número de pacientes que para el registro no mejoraban se aumentaba enormemente.
Por la dinámica del proceso diagnóstico, se requiere el diligenciamiento de instrumentos por parte del centro educativo en el que se encuentra el niño. La confirmación del cuadro de TDAH se realiza en la mayoría de los casos en la segunda consulta, razón por la cual el indicador de seguimiento se puntuó en la inmensa mayoría de los casos como "igual", pese a que en ese momento no se tenía diagnóstico confirmado. Así, el número de pacientes que aparentemente no mejoran también se ve incrementado. En algunos casos de pacientes que no mejoran, se encontró que el TDAH fue el diagnóstico presuntivo en la primera consulta, pero que posteriormente se encontró otro diagnóstico el cual fue confirmado. De estos 14 casos, la mayoría correspondió a retardo mental. En los datos preliminares estos informes aumentan el número de niños que no mejoran.
Muchos de los problemas de registro encontrados lo fueron en fechas específicas, de movimiento de residentes, nuevos en el registro del sistema, lo cual supone un error en quien ingresa los datos al sistema. Tales fechas corresponden a los meses en los cuales hay cambios de rotación de quienes tienen acceso al registro de consultas, las historias y el sistema, en general médicos internos y residentes.
Aunque no se refleja en los resultados, en la depuración de la base de datos se encontró que los pacientes eran reportados como consultantes por primera vez hasta cuatro veces, lo que falsea los resultados iniciales con respecto al número de pacientes totales que asisten al servicio. Este inconveniente llevó a que se consideraran más pacientes de los que en realidad consultaron. Sin embargo esta dificultad fue obviada eliminando los registros adicionales.
En muchos casos se registró la comorbilidad del TDAH, apareciendo esta categoría diagnóstica como de menor relevancia, con lo cual, al codificar los diagnósticos, se encontraban menos pacientes de los que en realidad había. Adicionalmente se encontraron limitantes con respecto a los pacientes y sus familias porque con frecuencia brindan datos erróneos. Con ello se dificultó su contacto y tarda más el proceso de aceptar un diagnóstico y su tratamiento médico. Esta es una razón adicional de abandono y no regreso a la consulta.
Al intentar caracterizar a los niños que no mejoraron, se encontró que corresponden a estratos socioeconómicos 2 o 3; que en un caso, en busca de segundas opiniones, se encuentran con personas, incluso médicos especialistas, que consideran que el tratamiento sugerido por psiquiatría es innecesario e incluso peligroso, con lo cual contribuyen a la confusión de la familia y del paciente, influyen sobre la conceptualización y conciencia de enfermedad y a la deserción de la consulta psiquiátrica.
En algunos de los pacientes con los cuales no se logró establecer contacto (n=3), al revisar las historias clínicas se encontró que no cumplían con la prescripción médica, poca adherencia al tratamiento y abandono del mismo y de la asistencia a controles. Sin embargo estos pacientes no fueron incluidos en la caracterización dado que se desconoce la causa del abandono y la concepción que se tiene sobre esta condición. La presentación cultural y social de que quien asiste al psiquiatra está "loco" y que si se recibe un medicamento psiquiátrico esta opinión se confirma y generaliza, hace que con frecuencia se tenga temor a la consulta y aún más a recibir medicación.
Pese a todas estas limitantes, tras depurar la base de registros, al evaluar a los pacientes en los que se confirma el diagnóstico de TDAH y se inicia tratamiento se encontró que lo reportado por el Hospital Pediátrico de la Misericordia corresponde a la literatura mundial.
Sin embargo al hacer la búsqueda en diferentes bases de datos internacionales se encuentran muy pocos estudios de seguimiento específicos, que no incluyen el TDAH complicado y ninguno que caracterice a la población que no mejora. Estudios como este, que describen los procesos domésticos, son importantes para reconocer las condiciones propias de trabajo, limitaciones, fortalezas y reconocimiento de la población que consulta.
Conclusión
El 82,45% de los niños que consultan al Hospital Pediátrico de la Misericordia, en quienes se confirma diagnóstico y se inicia tratamiento para el TDAH reportan mejoría clínica.
En los niños que no reportan mejoría esta se debe principalmente al no cumplimiento y abandono del tratamiento sugerido, con lo que se llega a condiciones complicadas con comorbilidad especialmente escolar, pese a lo cual se encuentra una pobre conciencia de enfermedad. No se encontraron casos reportados de intolerancia por efectos adversos de los medicamentos formulados. Los datos informados en el Hospital Pediátrico de la Misericordia se corresponden con los de la literatura mundial con respecto a la eficacia de los tratamientos instaurados.
Agradecimientos
Agradecemos a los Doctores Doriam Mauricio Achury (Médico interno) y Diana Botero Franco (Psiquiatra de niños) por su colaboración en la revisión sistemática de las historias clínicas de los pacientes objeto de estudio en el Hospital Pediátrico de la Misericordia. Adicionalmente agradecemos a la sección de estadística del Hospital, de la cual hacen parte Cristian Camilo Pinilla, Julio Cesar Marentes Figueroa, Teodoro Páramo Galeano y Juan ángel Rivas Pinilla por su colaboración en la consecución de las historias clínicas.
Referencias
1. American Psychiatric Association. Manual diagnóstico y estadístico de los trastornos mentales, texto revisado. DSM-IV-TR 2002: 45 - 154.
2. Organización Mundial de la Salud. Trastornos mentales y del comportamiento. Descripciones clínicas y pautas para el diagnóstico. CIE 10. 1992: 319 - 355.
3. Pelham WE. Pharmacotherapy for children with attention-deficit hyperactivity disorder. School Psychol Rev. 1993; 22: 199 - 227.
4. Richters JE, Arnold LE, Jensen P, Abikoff H, Conners CK, Greenhill LL. NIMH collaborative multisite multimodal treatment study of children with ADHD: I. Background and rationale. J Am Acad Child Adolesc Psychiatry 1995; 34: 987 - 1000.
5. The MTA Cooperative Group. A 14-month randomized clinical trial of treatment strategies for attentiondeficit/ hyperactivity disorder. Arch Gen Psychiatry 1999; 56: 1073 - 1086.
6. Antshel KM, Remer R. Social skills training in children with attention deficit hyperactivity disorder: a randomized-controlled clinical trial. J Clin Child Ado-lesc Psychol. 2003; 32: 153 - 165.
7. The MTA Cooperative Group. Moderators and mediator of treatment response for children with attention-deficit/hyperactivity disorder. Arch Gen Psychiatry 1999; 56: 1088 - 1096.
8. Tutty S, Gephart H, Wurzbacher K. Enhancing behavioral and social skill functioning in children newly diagnosed with attention-deficit hyperactivity disorder in a pediatric setting. J Dev Behav Pediatr. 2003; 24: 51 - 57.
9. Klassen A, Miller A, Raina P, Lee S K, Olsen L. Attention-deficit hyperactivity disorder in children and youth: a quantitative systematic review of the efficacy of different management strategies. Canadian Journal of Psychiatry 1999; 44: 1007 - 1016.
10. Montiel-Nava C, Peña JA, Espina-Mariñes G, Ferrer-Hernández ME, López-Rubio A, Puertas-Sánchez S, Cardozo-Durán JJ. Estudio piloto de metilfenidato y entrenamiento a padres en el tratamiento de niños con trastorno por déficit de atención-hiperactividad. Rev Neurol 2002; 35: 201 - 205.
11. Gadow KD, Nolan EE, Sverd J, Sprafkin J, Paolicelli L. Methylphenidate in aggressive-hiperactivity boys. I. Effects on peer aggression in public school settings. J Am Acad Child Adolesc Psychiatry 1990;29: 710 - 718.
12. Charach A, Ickowicz A, Schachar R Stimulant treatment over five years: adherence, effectiveness, and adverse effects. J Am Acad Child Adolesc Psychiatry. 2004; 43: 559-567.
13. Lambert NM. Adolescent Outcomes for Hyperactive Children. Perspectives on General and Specific Patterns of Chidhood Risk for Adolescent Educational, Social, and Mental Health Problems. American Psychologist 1988; 43: 786 - 799.
14. Hinshaw SP. Academia underachievement, attention deficits, and agresión: comorbidity and implications for intervención. J Consul Clin Psychol 1992; 60: 893-903.
15. Pliszka SR, Carlson CL, Swanson JM. ADHD with conmorbid disorders. Clinical assessment and management. New York: The Guilford Press; 1999.
16. Newcorn JH, Spencer TJ, Biederman J, Milton DR, Michelson D. Atomoxetine treatment in children and adolescents with attention-deficit/hyperactivity disorder and comorbid oppositional defiant disorder. J Am Acad Child Adolesc Psychiatry. 2005; 44:240 -248.
17. Hinshaw S. Academic Underachievement, Attention Deficits, and Aggression: Comorbidity and Implications for Intervention. Journal Of Consulting and Clinical Psychology. 1992, 60: 893 - 903.
18. Biederman J, Faraone SV, Monuteaux MC, Grossbard JR. How informative are parent reports of attention-deficit/hyperactivity disorder symptoms for assessing outcome in clinical trials of long-acting treatments? A pooled analysis of parents' and teachers' reports. Pediatrics. 2004; 113: 1667 - 1671.
19. Silvertone PH, Salsali M. Low self-esteem and psychiatric patients: Part I: The relationship between low self-esteem and psychiatric diagnosis. Annals of General Hospital Psychiatry 2003; 2: 2.
20. MTA Cooperative Group. Nacional Institute of Mental Health Multimodal Tratament Study of ADHD Follow-up: 24-Month Outcomes of Tratament Strategies for Attention-Deficit/Hyperactivity Disorder. Pediatrics 2004; 113: 754 - 761.
21. Wilens TE, Faraone SV, Biederman J, Gunawardene. Does Stimulant Therapy of Attention-Deficit/ Hyperactivity Disorder Beget Later Substance Abuse? AS Meta-analytic Review of the Literature. Pediatrics 2003; 111: 179 - 185.
22. Mannuzza S, Klein RG, Moulton JL 3rd. Does stimulant treatment place children at risk for adult substance abuse? A controlled, prospective followup study. J Child Adolesc Psychopharmacol. 2003; 13: 273 - 282.
23. MTA Coopeative Group. Nacional Institute of Mental Health Multimodal Treatment Study of ADHD Follow-up: Changes in Effectiveness and Growth Alter the End of Treatment. Pediatrics 2004; 113: 762 - 769.
24. Hoza B, Gerdes AC, Mrug S, Hinshaw SP, Bukowski WM, Gold JA, Arnold LE, Abikoff HB, Conners CK, Elliott GR, Greenhill LL, Hechtman L, Jensen PS, Kraemer HC, March JS, Newcorn JH, Severe JB, Swanson JM, Vitiello B, Wells KC, Wigal T. Peer-assessed outcomes in the multimodal treatment study of children with attention deficit hyperactivity disorder. J Clin Child Adolesc Psychol. 2005; 34: 74 - 86.
25. Abikoff H, Klein RG. Attention-Deficit Hyperactivity and Conduct Disorder: Comorbidity and Implications for Treatment. Journal Of Consulting and Clinical Psychology. 1992, 60: 881 - 892.
Referencias
American Psychiatric Association. Manual diagnóstico y estadístico de los trastornos mentales, texto revisado. DSM-IV-TR 2002: 45 - 154.
Organización Mundial de la Salud. Trastornos mentales y del comportamiento. Descripciones clínicas y pautas para el diagnóstico. CIE 10. 1992: 319 - 355.
Pelham WE. Pharmacotherapy for children with attention-deficit hyperactivity disorder. School Psychol Rev. 1993; 22: 199 - 227.
Richters JE, Arnold LE, Jensen P, Abikoff H, Conners CK, Greenhill LL. NIMH collaborative multisite multimodal treatment study of children with ADHD: I. Background and rationale. J Am Acad Child Adolesc Psychiatry 1995; 34: 987 - 1000.
The MTA Cooperative Group. A 14-month randomized clinical trial of treatment strategies for attentiondeficit/ hyperactivity disorder. Arch Gen Psychiatry 1999; 56: 1073 - 1086.
Antshel KM, Remer R. Social skills training in children with attention deficit hyperactivity disorder: a randomized-controlled clinical trial. J Clin Child Ado-lesc Psychol. 2003; 32: 153 - 165.
The MTA Cooperative Group. Moderators and mediator of treatment response for children with attention-deficit/hyperactivity disorder. Arch Gen Psychiatry 1999; 56: 1088 - 1096.
Tutty S, Gephart H, Wurzbacher K. Enhancing behavioral and social skill functioning in children newly diagnosed with attention-deficit hyperactivity disorder in a pediatric setting. J Dev Behav Pediatr. 2003; 24: 51 - 57.
Klassen A, Miller A, Raina P, Lee S K, Olsen L. Attention-deficit hyperactivity disorder in children and youth: a quantitative systematic review of the efficacy of different management strategies. Canadian Journal of Psychiatry 1999; 44: 1007 - 1016.
Montiel-Nava C, Peña JA, Espina-Mariñes G, Ferrer-Hernández ME, López-Rubio A, Puertas-Sánchez S, Cardozo-Durán JJ. Estudio piloto de metilfenidato y entrenamiento a padres en el tratamiento de niños con trastorno por déficit de atención-hiperactividad. Rev Neurol 2002; 35: 201 - 205.
Gadow KD, Nolan EE, Sverd J, Sprafkin J, Paolicelli L. Methylphenidate in aggressive-hiperactivity boys. I. Effects on peer aggression in public school settings. J Am Acad Child Adolesc Psychiatry 1990;29: 710 - 718.
Charach A, Ickowicz A, Schachar R Stimulant treatment over five years: adherence, effectiveness, and adverse effects. J Am Acad Child Adolesc Psychiatry. 2004; 43: 559-567.
Lambert NM. Adolescent Outcomes for Hyperactive Children. Perspectives on General and Specific Patterns of Chidhood Risk for Adolescent Educational, Social, and Mental Health Problems. American Psychologist 1988; 43: 786 - 799.
Hinshaw SP. Academia underachievement, attention deficits, and agresión: comorbidity and implications for intervención. J Consul Clin Psychol 1992; 60: 893-903.
Pliszka SR, Carlson CL, Swanson JM. ADHD with conmorbid disorders. Clinical assessment and management. New York: The Guilford Press; 1999.
Newcorn JH, Spencer TJ, Biederman J, Milton DR, Michelson D. Atomoxetine treatment in children and adolescents with attention-deficit/hyperactivity disorder and comorbid oppositional defiant disorder. J Am Acad Child Adolesc Psychiatry. 2005; 44:240 -248.
Hinshaw S. Academic Underachievement, Attention Deficits, and Aggression: Comorbidity and Implications for Intervention. Journal Of Consulting and Clinical Psychology. 1992, 60: 893 - 903.
Biederman J, Faraone SV, Monuteaux MC, Grossbard JR. How informative are parent reports of attention-deficit/hyperactivity disorder symptoms for assessing outcome in clinical trials of long-acting treatments? A pooled analysis of parents' and teachers' reports. Pediatrics. 2004; 113: 1667 - 1671.
Silvertone PH, Salsali M. Low self-esteem and psychiatric patients: Part I: The relationship between low self-esteem and psychiatric diagnosis. Annals of General Hospital Psychiatry 2003; 2: 2.
MTA Cooperative Group. Nacional Institute of Mental Health Multimodal Tratament Study of ADHD Follow-up: 24-Month Outcomes of Tratament Strategies for Attention-Deficit/Hyperactivity Disorder. Pediatrics 2004; 113: 754 - 761.
Wilens TE, Faraone SV, Biederman J, Gunawardene. Does Stimulant Therapy of Attention-Deficit/ Hyperactivity Disorder Beget Later Substance Abuse? AS Meta-analytic Review of the Literature. Pediatrics 2003; 111: 179 - 185.
Mannuzza S, Klein RG, Moulton JL 3rd. Does stimulant treatment place children at risk for adult substance abuse? A controlled, prospective followup study. J Child Adolesc Psychopharmacol. 2003; 13: 273 - 282.
MTA Coopeative Group. Nacional Institute of Mental Health Multimodal Treatment Study of ADHD Follow-up: Changes in Effectiveness and Growth Alter the End of Treatment. Pediatrics 2004; 113: 762 - 769.
Hoza B, Gerdes AC, Mrug S, Hinshaw SP, Bukowski WM, Gold JA, Arnold LE, Abikoff HB, Conners CK, Elliott GR, Greenhill LL, Hechtman L, Jensen PS, Kraemer HC, March JS, Newcorn JH, Severe JB, Swanson JM, Vitiello B, Wells KC, Wigal T. Peer-assessed outcomes in the multimodal treatment study of children with attention deficit hyperactivity disorder. J Clin Child Adolesc Psychol. 2005; 34: 74 - 86.
Abikoff H, Klein RG. Attention-Deficit Hyperactivity and Conduct Disorder: Comorbidity and Implications for Treatment. Journal Of Consulting and Clinical Psychology. 1992, 60: 881 - 892.
Cómo citar
APA
ACM
ACS
ABNT
Chicago
Harvard
IEEE
MLA
Turabian
Vancouver
Descargar cita
Visitas a la página del resumen del artículo
Descargas
Licencia
Derechos de autor 2005 Revista de la Facultad de Medicina

Esta obra está bajo una licencia internacional Creative Commons Atribución 4.0.
-


















