



Publicado
Cambio en la clasificación macroscópica de la apendicitis. ¿Tiene algún impacto? Estudio retrospectivo en un Hospital Universitario Pediátrico
Change in the macroscopic classification of appendicitis. Does it have any impact? Retrospective study in a Pediatric teaching hospital
DOI:
https://doi.org/10.15446/revfacmed.v63n2.49316Palabras clave:
Antibióticos, Apendicitis, Sépsis abdominal, Complicaciones Posoperatorias, Antibiótico post-operatorio (es)Anti-Bacterial Agents, Appendicitis, Sepsis, Postoperative care, Postoperative antibiotic (en)
Antecedentes. La definición actual de apendicitis diferencia la aguda en apéndices no perforados y perforados. Esta clasificación describe los apéndices perforados como aquellos con la presencia de un orificio visible en el apéndice o la presencia de un fecalito libre en la cavidad y ha cambiado el manejo postoperatorio actual.
Objetivo. Determinar si el cambio en la definición macroscópica de la apendicitis aguda tiene alguna influencia en la duración de la estancia hospitalaria y la tasa de complicaciones dado el cambio en el manejo antibiótico postoperatorio.
Materiales y métodos. Se llevó a cabo un rastreo de aquellos pacientes llevados a cirugía con diagnóstico de apendicitis aguda durante el primer semestre del año 2009 y el segundo semestre del año 2011 en la Fundación HOMI. Se excluyeron los pacientes llevados a laparoscopia diagnóstica por estudio del dolor abdominal, apendicectomias incidentales y los pacientes manejados en el protocolo de apendicectomía de Intervalo.
Resultados. Se observó una disminución en el número de días de hospitalización/año y en el número de dosis de antibiótico/año y reducción en el número de complicaciones, lo cual demuestra que la clasificación y el protocolo de manejo actual no se correlacionan con un aumento en el número de complicaciones y se asocia con menores costos.
Conclusión. El cambio en la clasificación macroscópica y el aportar la nueva definición sobre apendicitis perforada ha logrado disminuir la estancia hospitalaria y la cantidad de antibióticos utilizados sin una repercusión significativa en la tasa de complicaciones.
Background. The current definition differences the acute appendix in nonperforated and perforated. This classification describes the perforated appendicitis as those with the presence of a visible hole in the appendix or the presence of a free fecalito in the cavity and changed the postoperative current management.
Objective. Determine whether the change in the macroscopic definition of acute appendicitis have any influence on the length of hospital stay and complication rates given the change in the post-operative antibiotic treatment.
Materials and Methods. Patients undergoing surgery with a diagnosis of acute appendicitis in the first half of 2009 and the second half of 2011. Patients excluded were those taken to surgery for diagnostic laparoscopy by study of abdominal pain, also incidental appendectomy and patients managed in the protocol of appendectomy interval.
Results. A decrease in the number of hospital days /year and the number of doses of antibiotic/ year and decrease in the number of complications was observed which demonstrates that the classification and current management protocol are not correlated with an increase in number of complications and is associated with lower costs.
Conclusions. The change in the macroscopic classification and provide the new definition of perforated appendicitis has reduced hospital stay and the amount of antibiotics used without a significant impact on the rate of complications.
DOI: https://doi.org/10.15446/revfacmed.v63n2.49316
INVESTIGACIÓN ORIGINAL
Cambio en la clasificación macroscópica de la apendicitis. ¿Tiene algún impacto? Estudio retrospectivo en un Hospital Universitario Pediátrico
Change in the macroscopic classification of appendicitis. Does it have any impact? Retrospective study in a Pediatric teaching hospital
Sergio David Castañeda-Espinosa1,2, Iván Molina-Ramírez1,2, Alejandra Holguín-Sanabria1,2, Paula Jaimes-de La Hoz1,2, Miguel Perilla-López1,2, Alejandra Pedraza-Carvajal1,2 , Fernando Fierro-Ávila1,2
1 Unidad de Cirugía Pediátrica, Facultad de Medicina, Universidad Nacional de Colombia. Bogotá D. C., Colombia.
2 Fundación HOMI Hospital de La Misericordia. Bogotá D. C., Colombia.
Correspondencia: Sergio David Castañeda-Espinosa. Fundación HOMI Hospital de la Misericordia. Avenida Caracas No. 1-13. Bogotá D. C., Colombia. Teléfono: + 57 1 3811970. Correo electrónico: sdcastanedae@unal.edu.co.
Recibido:24/02/2015 Aceptado: 24/03/2015
Resumen
Antecedentes. La definición actual de apendicitis diferencia la aguda en apéndices no perforados y perforados. Esta clasificación describe los apéndices perforados como aquellos con la presencia de un orificio visible en el apéndice o la presencia de un fecalito libre en la cavidad y ha cambiado el manejo postoperatorio actual.
Objetivo. Determinar si el cambio en la definición macroscópica de la apendicitis aguda tiene alguna influencia en la duración de la estancia hospitalaria y la tasa de complicaciones dado el cambio en el manejo antibiótico postoperatorio.
Materiales y métodos. Se llevó a cabo un rastreo de aquellos pacientes llevados a cirugía con diagnóstico de apendicitis aguda durante el primer semestre del año 2009 y el segundo semestre del año 2011 en la Fundación HOMI. Se excluyeron los pacientes llevados a laparoscopia diagnóstica por estudio del dolor abdominal, apendicectomias incidentales y los pacientes manejados en el protocolo de apendicectomía de Intervalo.
Resultados. Se observó una disminución en el número de días de hospitalización/año y en el número de dosis de antibiótico/año y reducción en el número de complicaciones, lo cual demuestra que la clasificación y el protocolo de manejo actual no se correlacionan con un aumento en el número de complicaciones y se asocia con menores costos.
Conclusión. El cambio en la clasificación macroscópica y el aportar la nueva definición sobre apendicitis perforada ha logrado disminuir la estancia hospitalaria y la cantidad de antibióticos utilizados sin una repercusión significativa en la tasa de complicaciones.
Palabras clave: Antibióticos; Apendicitis; Sépsis abdominal; Complicaciones Posoperatorias; Antibiótico post-operatorio (DeCS).
Castañeda-Espinosa SD, Molina-Ramírez I, Holguín-Sanabria A, Jaimes-de La Hoz P, Perilla-López M, Pedraza-Carvajal A, et al. Cambio en la clasificación macroscópica de la apendicitis. ¿Tiene algún impacto? Estudio retrospectivo en un Hospital Universitario Pediátrico. Rev. Fac. Med. 2015;63(2):243-50. doi: https://doi.org/10.15446/revfacmed.v63n2.49316.
Summary
Background. The current definition differences the acute appendix in nonperforated and perforated. This classification describes the perforated appendicitis as those with the presence of a visible hole in the appendix or the presence of a free fecalito in the cavity and changed the postoperative current management.
Objective. Determine whether the change in the macroscopic definition of acute appendicitis have any influence on the length of hospital stay and complication rates given the change in the post-operative antibiotic treatment.
Materials and Methods. Patients undergoing surgery with a diagnosis of acute appendicitis in the first half of 2009 and the second half of 2011. Patients excluded were those taken to surgery for diagnostic laparoscopy by study of abdominal pain, also incidental appendectomy and patients managed in the protocol of appendectomy interval.
Results. A decrease in the number of hospital days /year and the number of doses of antibiotic/ year and decrease in the number of complications was observed which demonstrates that the classification and current management protocol are not correlated with an increase in number of complications and is associated with lower costs.
Conclusions. The change in the macroscopic classification and provide the new definition of perforated appendicitis has reduced hospital stay and the amount of antibiotics used without a significant impact on the rate of complications.
Keywords: Anti-Bacterial Agents; Appendicitis; Sepsis; Postoperative care; Postoperative antibiotic (MeSH).
Castañeda-Espinosa SD, Molina-Ramírez I, Holguín-Sanabria A, Jaimes-de La Hoz P, Perilla-López M, Pedraza-Carvajal A, et al. [Change in the macroscopic classification of appendicitis. Does it have any impact? Retrospective study in a Pediatric teaching hospital]. Rev. Fac. Med. 2015;63(2):243-50. Spanish. doi: https://doi.org/10.15446/revfacmed.v63n2.49316.
Antecedentes
La Apendicitis Aguda (AA) es la condición quirúrgica más común en niños con un riesgo establecido entre 6.7 y 9 %. La presentación es variable dependiendo de la edad del paciente, la duración de los síntomas y la posición del Apéndice en el abdomen, con un espectro entre el paciente mínimamente sintomático hasta el cuadro de obstrucción intestinal y clínica de choque séptico (1-5).
La definición actual clasifica la Apendicitis Aguda en no perforada y perforada contemplando los perforados como aquellos con un orificio visible en el apéndice o la presencia de un fecalito libre en la cavidad. Esto ha cambiado el manejo postoperatorio. Antes de esta clasificación los apéndices descritos como gangrenosos o necróticos eran tratados como perforados, aún sin evidencia de un orificio visible, lo que implicaba el uso de antibiótico postoperatorio. Aún hoy no existe un acuerdo en la definición sobre este hallazgo, pero se ha demostrado que con el diagnóstico basado en el hallazgo subjetivo tienen mejor pronóstico que aquellos con apéndices perforados y manejados con el mismo esquema de tratamiento; por lo que limitar el uso de antibiótico postoperatorio en los pacientes con apendicitis gangrenosa ha disminuido los costos sin aumentar de forma significativa la morbilidad (3,6,7).
El tratamiento en apendicitis no perforada se basa en una adecuada hidratación y la administración de antibióticos de amplio espectro en el preoperatorio. Una dosis única es efectiva en disminuir la tasa de infección del sitio operatorio (ISO) —incluido la formación de abscesos— sin necesidad del uso de una segunda dosis en el postoperatorio (2,4-8).
El uso de antibióticos endovenosos es el estándar para el manejo durante el periodo de recuperación por un cuadro de apendicitis perforada. El problema se basa en la ausencia de una definición clara sobre cómo clasificar la perforación y, a pesar de la amplia prevalencia, no hay consenso con respecto al diagnóstico y manejo. Asimismo, es difícil encontrar una guía respecto al tratamiento antibiótico, dada la variabilidad que existe en la elección del agente antimicrobiano, la duración de la terapia y la ruta de administración.
Sobre esto, se ha descrito el esquema triconjugado para la cobertura de microorganismos anaerobios, Gram-negativos y Gram-positivos con una duración de hasta 10 días, pero existen protocolos más actuales con el uso de un solo antibiótico o esquemas biconjugados, los cuales han demostrado ser igual de efectivos con disminución en los costos, los días de hospitalización requeridos y la duración de la terapia. También existen reportes de esquemas de tratamiento endovenoso, que se puede completar con un esquema oral según la evolución del paciente. Sin embargo, no hay aún consenso adecuado y el tema de la resistencia bacteriana se ha convertido en otro de los temas de preocupación global (9-20).
El objetivo de este estudio es determinar si el cambio en la definición macroscópica de la apendicitis aguda tiene influencia en la duración de la estancia hospitalaria y la tasa de complicaciones, dado el cambio en el protocolo de manejo antibiótico. Complicaciones posteriores al manejo inicial conllevan la necesidad de nuevos estudios imagenológicos, procedimientos invasivos, mayor tiempo de manejo antibiótico y prolongación de la estancia hospitalaria con reportes de hasta un 58 % en la tasa de complicaciones, cuando la presentación inicial del cuadro es con apendicitis perforada (3,8,15,20-24).
La apendicectomía continúa siendo el procedimiento más realizado con un promedio de 75 procedimientos mensuales. La clasificación usada en el año 2009 dividía los apéndices en: macroscópicamente normales, fibrinopurulentos, gangrenosos, perforado con peritonitis localizada y perforada con peritonitis generalizada. En el año 2010, se realizó el cambio en la denominación "macroscópica" a "macroscópicamente normales", "no perforada" y "perforada con peritonitis localizada o generalizada" según los hallazgos intraoperatorios (3,23).
Este protocolo está diseñado para determinar si el cambio realizado en la clasificación macroscópica ha influido en el pronóstico, la tasa de complicaciones, las reintervenciones y los reingresos. Este trabajo es un estudio descriptivo con cohortes retrospectivos.
Materiales y métodos
Población de pacientes
Se tomaron los pacientes llevados a cirugía con diagnóstico de apendicitis aguda durante el primer semestre del año 2009 y el segundo semestre del año 2011 en la Fundación HOMI, ya que durante estos meses la clasificación macroscópica fue realizada de forma más estricta según los protocolos del servicio. El criterio de inclusión aplica a todos los pacientes llevados a cirugía con diagnóstico de apendicitis aguda. Se excluyeron los pacientes llevados a laparoscopia diagnóstica por estudio del dolor abdominal, apendicectomias incidentales y los pacientes manejados en el protocolo de apendicectomía de intervalo.
Diseño del estudio
Los datos recolectados fueron: edad del paciente, género, tiempo de evolución desde ingreso al servicio de urgencias, resultado de los estudios paraclínicos e imagenológicos, abordaje quirúrgico, hallazgos intraoperatorios, manejo antibiótico y la duración de este, evolución postoperatoria, complicaciones (reingresos, infecciones del sitio operatorio, abscesos postoperatorios) y el tiempo de estancia hospitalaria. El seguimiento de los pacientes se realizó en la consulta externa realizada dos semanas después del procedimiento quirúrgico (6,14,15).
Los hallazgos son determinados por el cirujano durante el intraoperatorio y son descritos según la clasificación utilizada en cada año. El manejo antibiótico se refiere al tipo de esquema utilizado y al número de dosis del antibiótico. Por otra parte, la evolución postoperatoria hace referencia a la necesidad de cuidado en unidades especiales y las complicaciones infecciosas asociadas a la estancia hospitalaria. Las complicaciones se describen como infecciones del sitio operatorio (superficial, profunda, órgano-espacio), la necesidad de reintervención y los cuadros de obstrucción intestinal. La estancia hospitalaria se describe como el número de días completos que requirió el paciente para el manejo postoperatorio hasta el egreso (13).
Intervención
El protocolo de manejo inicia con la administración de antibiótico profiláctico desde el momento del diagnóstico (ampicilina-sulbactam 200mg/kg/día en 4 dosis) y se continúa con el curso del tratamiento según los hallazgos. Los apéndices descritos como no perforados (edematosos, fibrinopurulentos y gangrenosos) reciben este esquema sin necesidad de manejo postoperatorio y con plan de alta al tener tolerancia a la vía oral y control del dolor. Los descritos como perforados requieren estancia mínima de 5 días para continuar el manejo antibiótico. Actualmente en el protocolo no se contempla seguimiento postoperatorio con hemograma ni otro tipo de estudios paraclínico, con un esquema donde todo el antibiótico se administra de forma endovenosa intrahospitalaria. La comparación del protocolo actual se realizó con respecto al año 2009, donde los apéndices descritos como fibrinopurulentos recibían hasta 4 dosis de manejo antibiótico y los descritos como gangrenosos recibían manejo antibiótico durante 48 a 72 horas (4,11).
Metodología estadística
Análisis univariado de las variables. Se utilizó el test de Wald corregido para ver la diferencia entre las medias de las variables y, posterior a esto, se realizó la prueba de hipótesis sobre el coeficiente de correlación de Pearson. Si hay por lo menos 4 pares completos de observación, un intervalo de confianza asintótico se da sobre la base de la transformada Z de Fisher y, por último, se realizó una prueba Exacta de Fisher.
Resultados
Se revisaron 607 pacientes con diagnóstico de apendicitis aguda, 303 pacientes en el grupo de 2009 y 304 pacientes con clasificación de 2011. Las variables demográficas en ambos grupos fueron similares con respecto a la edad y el género (Tabla 1).

Grupo I. Año 2009
El tiempo promedio de evolución al ingreso fue 45.4 horas con un rango entre 28.4 para el grupo de las apéndices edematosas, y hasta 67.82 horas para el grupo de las perforadas con peritonitis localizada. El uso de paraclínicos fue 71.9 % y el de imágenes diagnósticas 20.4 %.
El abordaje por incisión de Rockey-Davis se utilizó en el 93 % de los pacientes: laparoscópico en 4.6 % y laparotomía por línea media en 2.3 % de los casos; además, la mayoría fue en los pacientes descritos con peritonitis generalizada.
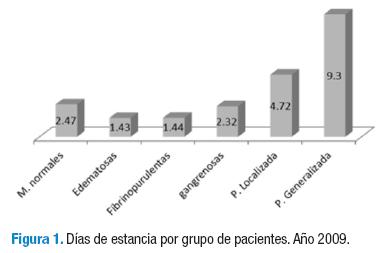
En 2009, la clasificación por apéndices era de 6 grupos según los hallazgos macroscópicos intraoperatorios: 7.6 % corresponden a apéndices macroscópicamente normales, 5.3 % a edematosas, 42.9 % a fibrinopurulentas, 9.2 % a gangrenosas, 26.07 % descritas como perforadas con peritonitis localizada y 8.9 % al grupo de con peritonitis generalizada. El manejo antibiótico en el 94.7 % de los casos fue con ampicilina sulbactam, de ellos, el 1.6 % recibió cambio de esquema a piperacilina tazobactam por los hallazgos intraoperatorios y en 0.99 % de los casos se realizó tratamiento con el esquema de Clindamicina + Amikacina por decisión del cirujano tratante. En 2.6 % de los casos no hay registros en la historia clínica sobre el uso de antibióticos. Las dosis de antibióticos fueron 9.5 dosis por paciente, 1 dosis en el grupo de las apéndices edematosas hasta 34.2 dosis en el grupo de las peritonitis generalizada. Los días de estancia postoperatoria fueron calculados en un promedio de 3.7 días con un rango de 1.4 para las apéndices edematosas, y hasta 9.03 para el grupo con peritonitis generalizada (Figura 1).
Se presentaron complicaciones en 16.8 % de los casos, 43 infecciones del sitio operatorio; 32 superficiales y 11 órgano-espacio, no hay reporte de infecciones del sitio operatorio profundas. En el grupo de apéndices edematosas se presentó una infección superficial, en el grupo de apéndices fibrinopurulentas se encontraron 7 casos de infecciones superficiales y 2 órgano-espacio, en el grupo de apéndices gangrenosas se documentaron 3 infecciones superficiales, en el grupo de perforadas con peritonitis localizadas 14 infecciones superficiales y 3 órgano-espacio y en el grupo de peritonitis generalizada se documentaron 6 infecciones superficiales y 6 órgano-espacio. Existen 8 casos de obstrucción intestinal, 3 en el grupo de peritonitis localizada y 5 en el grupo de peritonitis generalizada. Adicionalmente, hay reporte de 10 pacientes que requirieron reintervención, 6 por cuadros de obstrucción intestinal sin respuesta al manejo médico y 4 para realizar drenajes de colecciones residuales.
Grupo II. 2011
El tiempo promedio de evolución desde ingreso al servicio de urgencias fue de 47.8 horas con un rango entre 31 horas para el grupo de las no perforadas hasta 65 horas para el grupo de perforadas con peritonitis generalizada. El uso de paraclínicos fue 86.51 % y el de imágenes diagnósticas 31.90 %.
El abordaje por incisión de Rockey-Davis se utilizó en el 83.88 % de los pacientes, laparoscópico en 12.5 % y laparotomía por línea media en 3.61 % de los casos. En este grupo todos los abordajes descritos como laparotomía por línea media fueron utilizados en los pacientes con peritonitis generalizada.
En 2011, con el cambio en la clasificación se obtuvieron 4 grupos para el manejo los cuales se dividen en: apéndices macroscópicamente normales que corresponden al 6.9 % de los casos; no perforadas que corresponden al 55.26 % de los casos; 27.3 % descritas como perforadas y 10.52 % al grupo con peritonitis generalizada. El manejo antibiótico en el 90.5 % de los casos fue ampicilina sulbactam, 7.9 % de los pacientes recibió piperacilina tazobactam por los hallazgos intraoperatorios y la necesidad de manejo en unidades especiales por el cambio en el protocolo de sepsis de origen abdominal manejado en nuestra institución. En 1.6 % de los casos se realizó tratamiento con esquema de Clindamicina + Amikacina por decisión del cirujano tratante.
Las dosis de antibióticos fueron 10.2 dosis por paciente, 1.26 dosis en el grupo de las apéndices no perforadas hasta 31.3 dosis en el grupo de las peritonitis generalizada. Los días de estancia postoperatoria fueron calculados en un promedio de 3.5 días con un rango de 1.1 para las apéndices no perforadas hasta 11.04 para el grupo con peritonitis generalizada. Los días de estancia postoperatoria fueron en promedio 5.26 días con un rango de 1.1 para el grupo de las apéndices no perforadas hasta 11.4 para el grupo de peritonitis generalizada (Figura 2).

Se presentaron complicaciones en 12.1 % de los casos, 29 infecciones del sitio operatorio; 22 superficiales y 7 órgano-espacio. No hay reporte de infecciones del sitio operatorio profundas. En el grupo de los apéndices no perforados se presentaron 8 infecciones superficiales y una ISO órgano-espacio, en el grupo de las perforadas 11 superficiales y 2 órgano-espacio. Existen 3 casos de obstrucción intestinal, todas en el grupo de los pacientes con peritonitis generalizada y reporte de 5 pacientes que requirieron reintervención, 3 por cuadros de obstrucción intestinal sin respuesta al manejo médico y 2 para realizar drenajes de colecciones residuales.
Con estos datos se realizó el cálculo de los días de hospitalización/año y las dosis de antibiótico/año para los pacientes del estudio. En total la suma de días/año fue 892 días de hospitalización/año en el 2009, los cuales se dividen en: 57 días/año para macroscopicamente normales, 23 días/año para edematosas, 130 días/año para fibrinopurulentas, 65 días/año para gangrenosas, 373 días/año para perforadas con peritonitis localizada y 244 días/año en el grupo de perforadas con peritonitis generalizada. En 2011 la suma de días de hospitalización/año fue 1068 días/años los cuales se dividen en: 54 días/año para macroscopicamente normales, 192 días/año para no perforadas, 457 días/año para perforadas con peritonitis localizada y 365 días/año en el grupo de perforadas con peritonitis generalizada.
Con respecto a las dosis de antibiótico/año los datos en 2009 son 2901 dosis de antibiótico/año, que se dividen en: 79 dosis/año para macroscopicamente normales, 14 dosis/año para edematosas, 165 dosis/año para fibrinopurulentas, 249 dosis/año para gangrenosas, 1469 dosis/año para perforadas con peritonitis localizada y 925 dosis/año en el grupo de perforadas con peritonitis generalizada. En 2011 se requirieron 2993 dosis de antibiótico/año y se dividen en 21 dosis/año para macroscopicamente normales, 212 dosis/año para no perforadas, 1760 dosis/año para perforadas con peritonitis localizada y 1000 dosis/año en el grupo de perforadas con peritonitis generalizada.
Discusión
En el tratamiento de la apendicitis aguda un mejor régimen, la duración del esquema antibiótico y la forma de administración continúan siendo objeto de controversia; la duración y el tipo de tratamiento son determinados por los hallazgos intraoperatorios según el análisis de la severidad. El parámetro que tiene mayor influencia en el tiempo de hospitalización postoperatoria es la clasificación intraoperatoria como apendicitis perforada, ya que esta perforación tiene mayor riesgo de presentar un absceso postoperatorio (16,17,20).
El propósito del estudio fue evaluar si el cambio en la clasificación macroscópica de la apendicitis y el cambio en el tratamiento de estos pacientes han influenciado el pronóstico y el número de complicaciones.
Existen múltiples estudios acerca de las diferentes opciones de tratamiento que buscan disminuir los costos con la administración de antibióticos y la estancia hospitalaria. Se ha comparado el uso de antibiótico en una sola dosis diaria de cetriaxona y metronidazol, contra el esquema clásico triconjugado, el cual demostró ser más eficiente y costo-efectivo, sin aumentar el número de complicaciones. La base teórica es el uso de antibiótico postoperatorio únicamente en el grupo de las apendicitis perforadas, las cuales son descritas con los mismos criterios utilizados en nuestro estudio. En otro estudio se utilizó un esquema de tratamiento con antibiótico ambulatorio y se logró disminuir el tiempo de estancia hospitalaria, sin aumentar el número de complicaciones, pero dejando en claro que la definición sobre apendicitis aguda perforada es lo que permite diferenciar los pacientes en riesgo de presentar un absceso intraabdominal de los que no; además, esta nueva definición permite que los estudios sean reproducibles y generalizables (2,12).
El estudio buscó determinar si el cambio en la clasificación con la nueva definición tiene influencia en el número de complicaciones. No encontramos en la literatura datos publicados respecto a otros grupos realizando comparaciones similares. A pesar de ser un trabajo retrospectivo, contamos con una amplia base de datos que nos permitió acceder a una cantidad suficiente de pacientes en cada grupo de clasificación.
Para el análisis se realizó la comparación entre el grupo descritos como apéndices edematosas, fibrinopurulentas y gangrenosas en 2009, las cuales se corresponde a las descritas como no perforadas en 2011 (Tabla 2 y 3) . Se observó una disminución significativa en el número de días de hospitalización/año y en el número de dosis de antibiótico/año entre los dos grupos, lo cual justifica el uso de la nueva clasificación y se encontró una disminución en el número de complicaciones que demuestra que la clasificación y el protocolo de manejo actual no se correlacionan con un aumento en el número de complicaciones y se asocia con menores costos, dada la reducción en la estancia hospitalaria y en el uso de antibióticos.


El cambio realizado en el protocolo de manejo de sepsis de origen abdominal, el cual determina el uso de piperacilina tazobactam en lugar de ampicilina sulbactam, para los casos de apendicitis perforada con peritonitis generalizada y necesidad de manejo POP en la Unidad de Cuidados Intensivos, no influenció el análisis final sobre la duración de la estancia hospitalaria y el manejo antibiótico, ya que en los dos grupos de pacientes al igual que lo reportado en la literatura, la mayor tasa de complicaciones se presentó en este grupo y no existen diferencias significativas en la duración de la estancia hospitalaria.
Este estudio demuestra que el cambio en la clasificación macroscópica y el aportar la nueva definición sobre apendicitis perforada ha logrado disminuir la estancia hospitalaria y la cantidad de antibióticos utilizados sin tener una repercusión significativa en la tasa de complicaciones, por lo que la clasificación anterior no tiene utilidad en el manejo postoperatorio de los pacientes pediátricos con diagnóstico de apendicitis aguda.
Conflicto de intereses
Ninguno declarada por los autores.
Financiación
Ninguna declarada por los autores.
Agradecimientos
Al servicio de la Consultoría Estadística, Departamento de Estadística, Universidad Nacional de Colombia.
Referencias
1. Hennelly KE, Bachur R. Appendicitis update. Curr Opin Pediatr [Internet]. 2011 [cited 2015 may 08];23(3):281-5. doi: http://doi.org/dr6wqf.
2. Fraser JD, Aguayo P, Leys CM, Keckler SJ, Newland JG, Sharp SW, et al. A complete course of intravenous antibiotics vs a combination of intravenous and oral antibiotics for perforated appendicitis in children: a prospective, randomized trial. J Pediatr Surg [Internet]. 2010 [cited 2015 may 08];45(6):1198-202. doi: http://doi.org/bgv8rd.
3. St-Peter SD, Sharp SW, Holcomb GW III, Ostlie DJ. An evidence-based definition for perforated appendicitis derived from a prospective randomized trial. J Pediatr Surg [Internet]. 2008 [cited 2015 may 08];43(12):2242-5. doi: http://doi.org/dnnqh4.
4. Lee SL, Islam S, Cassidy LD, Abdullah F, Arca MJ, 2010 American Pediatric Surgical Association Outcomes and Clinical Trials Committee. Antibiotics and appendicitis in the pediatric population: an American Pediatric Surgical Association Outcomes and Clinical Trials Committee Systematic Review. J Pediatr Surg [Internet]. 2010 [cited 2015 may 08];45(11):2181-5. doi: http://doi.org/fgcmvc.
5. Dunn JC. Apendicitis. In: Coran AG editor. Pediatric Surgery. Seventh Edition. Philadelphia: Elsevier [Internet]; 2012 [cited 2015 may 08]. p. 1255-63. doi: http://doi.org/4gx.
6. Emil S, Taylor M, Ndiforchu F, Nguyen N. What are the true advantages of a pediatric appendicitis clinical pathway? Am Surg [Internet]. 2006 [cited 2015 may 08];72(10):885-9. Available from: http://goo.gl/2TmA4y.
7. Emil S, Gaied F, Lo A, Laberge JM, Puligandla P, Shaw K, et al. Gangrenous appendicitis in children: a prospective evaluation of definition, bacteriology, histopathology, and outcomes. J Surg Res [Internet]. 2012 [cited 2015 may 08];177(1):123-6. doi: http://doi.org/4gz.
8. Henry MC, Walker A, Silverman B, Gollin G, Islam S, Sylvester K, et al. Risk factors for the development of abdominal abscess following operation for perforated appendicitis in children. A multicenter case-control study. Arch Surg [Internet]. 2007 [cited 2015 may 08];142(3):236-41. doi: http://doi.org/c3fqkc.
9. Morrow SE, Newman KD. Current management of appendicitis. Semin Pediatr Surg [Internet]. 2007 [cited 2015 may 08];16(1):34-40. doi: http://doi.org/bcbjrt.
10. Chan KW, Lee KH, Mou JW, Cheung ST, Sihoe JD, Tam YH. Evidence-based adjustment of antibiotic in pediatric complicated appendicitis in the era of antibiotic resistance. Pediatr Surg Int [Internet]. 2010 [cited 2015 may 08];26(2):157-60. doi: http://doi.org/bwdwqz.
11. Bliss D, Mckee J, Cho D, Krishnaswami S, Zallen G, Harrison M, et al. Discordance of the pediatric surgeon's intraoperative assessment of pediatric appendicitis with the pathologists report. J Pediatr Surg [Internet]. 2010 [cited 2015 may 08];45(7):1398-403. doi: http://doi.org/d4m8nn.
12. St-Peter SD, Tsao K, Spilde T, Holcomb GW III, Sharp SW, Murphy JP, et al. Single daily dosing ceftriaxone and metronidazole vs standard triple antibiotic regimen for perforated appendicitis in children: a prospective randomized trial. J Pediatr Surg [Internet]. 2008 [cited 2015 may 08];43(6):981-5. doi: http://doi.org/ccx7xh.
13. Schmitt F, Clermidi P, Dorsi M, Cocquerelle V, Ferreira-Gomes C, Becmeur F. Bacterial studies of complicated appendicitis over a 20-year period and their impact on empirical antibiotic treatment. J Pediatr Surg [Internet]. 2012 [cited 2015 may 08];47(11):2055-62. doi: http://doi.org/4g2.
14. Bahar MM, Jangjoo A, Amouzeshi A, Kavianifar K. Wound infection incidence in patients with simple and gangrenous or perforated appendicitis. Arch Iran Med [Internet]. 2010 [cited 2015 may 08];13(1):13-6. Available from: http://goo.gl/iW8Vb7.
15. Kokoska ER, Silen ML, Tracy TF, Dillon PA, Cradock TV, Weber TR. Perforated appendicitis in children: Risk factors for the development of complications. Surgery [Internet]. 1998 [cited 2015 may 08];124(4):619-25. doi: http://doi.org/dv43sp.
16. Solomkin JS, Mazuski JE, Bradley JS, Rodvold KA, Goldstein EJ, Baron EJ, et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis [Internet]. 2010 [cited 2015 may 08];50(2):133-64. doi: http://doi.org/c7g8s4.
17. Rafati MR, Rouini MR, Mojtahedzadeh M, Najafi A, Tavakoli H, Gholami K, et al. Clinical efficacy of continuous infusion of piperacillin compared with intermittent dosing in septic critically ill patients. Int J Antimicrob Agents [Internet]. 2006 [cited 2015 may 08];28(2):122-7. doi: http://doi.org/fj9hbp.
18. Stengel JW, Webb EM, Poder L, Yeh B, Smith-Bindman R, Coakley FV. Acute appendicitis: clinical outcome in patients with an initial false-positive CT diagnosis. Radiology [Internet]. 2010 [cited 2015 may 08];256(1):119-26. doi: http://doi.org/bfk88h.
19. Wang X, Zhang W, Yang X, Shao J, Zhou X, Yuan J. Complicated appendicitis in children: is laparoscopic appendectomy appropriate? A comparative study with the open appendectomy-our experience. J Pediatr Surg [Internet]. 2009 [cited 2015 may 08];44(10):1924-7. doi: http://doi.org/b6h6gb.
20. Bröker ME, van Lieshout EM, van der Elst M, Stassen LP, Schepers T. Discriminating between simple and perforated appendicitis. J Surg Res [Internet]. 2012 [cited 2015 may 08];176(1):79-83. doi: http://doi.org/fgt577.
21. Snelling CMH, Poenaru D, Drover JW. Minimum postoperative antibiotic duration in advanced appendicitis in children: a review. Pediatr Surg Int [Internet]. 2004 [cited 2015 may 08];20(11-12):838-45. doi: http://doi.org/fr8cdt.
22. Lee SL, Shekherdimian S, Chiu VY, Sydorak RM. Perforated appendicitis in children: equal access to care eliminate racial and socioeconomic disparities. J Pediatr Surg [Internet]. 2010 [cited 2015 may 08];45(6):1203-7. doi: http://doi.org/cfb5fz.
Referencias
Hennelly KE, Bachur R. Appendicitis update. Curr Opin Pediatr [Internet]. 2011 [cited 2015 may 08];23(3):281-5. doi: http://doi.org/dr6wqf.
Fraser JD, Aguayo P, Leys CM, Keckler SJ, Newland JG, Sharp SW, et al. A complete course of intravenous antibiotics vs a combination of intravenous and oral antibiotics for perforated appendicitis in children: a prospective, randomized trial. J Pediatr Surg [Internet]. 2010 [cited 2015 may 08];45(6):1198-202. doi: http://doi.org/bgv8rd.
St-Peter SD, Sharp SW, Holcomb GW III, Ostlie DJ. An evidence-based definition for perforated appendicitis derived from a prospective randomized trial. J Pediatr Surg [Internet]. 2008 [cited 2015 may 08];43(12):2242-5. doi: http://doi.org/dnnqh4.
Lee SL, Islam S, Cassidy LD, Abdullah F, Arca MJ, 2010 American Pediatric Surgical Association Outcomes and Clinical Trials Committee. Antibiotics and appendicitis in the pediatric population: an American Pediatric Surgical Association Outcomes and Clinical Trials Committee Systematic Review. J Pediatr Surg [Internet]. 2010 [cited 2015 may 08];45(11):2181-5. doi: http://doi.org/fgcmvc.
Dunn JC. Apendicitis. In: Coran AG editor. Pediatric Surgery. Seventh Edition. Philadelphia: Elsevier [Internet]; 2012 [cited 2015 may 08]. p. 1255-63. doi: http://doi.org/4gx.
Emil S, Taylor M, Ndiforchu F, Nguyen N. What are the true advantages of a pediatric appendicitis clinical pathway? Am Surg [Internet]. 2006 [cited 2015 may 08];72(10):885-9. Available from: http://goo.gl/2TmA4y.
Emil S, Gaied F, Lo A, Laberge JM, Puligandla P, Shaw K, et al. Gangrenous appendicitis in children: a prospective evaluation of definition, bacteriology, histopathology, and outcomes. J Surg Res [Internet]. 2012 [cited 2015 may 08];177(1):123-6. doi: http://doi.org/4gz.
Henry MC, Walker A, Silverman B, Gollin G, Islam S, Sylvester K, et al. Risk factors for the development of abdominal abscess following operation for perforated appendicitis in children. A multicenter case-control study. Arch Surg [Internet]. 2007 [cited 2015 may 08];142(3):236-41. doi: http://doi.org/c3fqkc.
Morrow SE, Newman KD. Current management of appendicitis. Semin Pediatr Surg [Internet]. 2007 [cited 2015 may 08];16(1):34-40. doi: http://doi.org/bcbjrt.
Chan KW, Lee KH, Mou JW, Cheung ST, Sihoe JD, Tam YH. Evidence-based adjustment of antibiotic in pediatric complicated appendicitis in the era of antibiotic resistance. Pediatr Surg Int [Internet]. 2010 [cited 2015 may 08];26(2):157-60. doi: http://doi.org/bwdwqz.
Bliss D, Mckee J, Cho D, Krishnaswami S, Zallen G, Harrison M, et al. Discordance of the pediatric surgeon's intraoperative assessment of pediatric appendicitis with the pathologists report. J Pediatr Surg [Internet]. 2010 [cited 2015 may 08];45(7):1398-403. doi: http://doi.org/d4m8nn.
St-Peter SD, Tsao K, Spilde T, Holcomb GW III, Sharp SW, Murphy JP, et al. Single daily dosing ceftriaxone and metronidazole vs standard triple antibiotic regimen for perforated appendicitis in children: a prospective randomized trial. J Pediatr Surg [Internet]. 2008 [cited 2015 may 08];43(6):981-5. doi: http://doi.org/ccx7xh.
Schmitt F, Clermidi P, Dorsi M, Cocquerelle V, Ferreira-Gomes C, Becmeur F. Bacterial studies of complicated appendicitis over a 20-year period and their impact on empirical antibiotic treatment. J Pediatr Surg [Internet]. 2012 [cited 2015 may 08];47(11):2055-62. doi: http://doi.org/4g2.
Bahar MM, Jangjoo A, Amouzeshi A, Kavianifar K. Wound infection incidence in patients with simple and gangrenous or perforated appendicitis. Arch Iran Med [Internet]. 2010 [cited 2015 may 08];13(1):13-6. Available from: http://goo.gl/iW8Vb7.
Kokoska ER, Silen ML, Tracy TF, Dillon PA, Cradock TV, Weber TR. Perforated appendicitis in children: Risk factors for the development of complications. Surgery [Internet]. 1998 [cited 2015 may 08];124(4):619-25. doi: http://doi.org/dv43sp.
Solomkin JS, Mazuski JE, Bradley JS, Rodvold KA, Goldstein EJ, Baron EJ, et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis [Internet]. 2010 [cited 2015 may 08];50(2):133-64. doi: http://doi.org/c7g8s4.
Rafati MR, Rouini MR, Mojtahedzadeh M, Najafi A, Tavakoli H, Gholami K, et al. Clinical efficacy of continuous infusion of piperacillin compared with intermittent dosing in septic critically ill patients. Int J Antimicrob Agents [Internet]. 2006 [cited 2015 may 08];28(2):122-7. doi: http://doi.org/fj9hbp.
Stengel JW, Webb EM, Poder L, Yeh B, Smith-Bindman R, Coakley FV. Acute appendicitis: clinical outcome in patients with an initial false-positive CT diagnosis. Radiology [Internet]. 2010 [cited 2015 may 08];256(1):119-26. doi: http://doi.org/bfk88h.
Wang X, Zhang W, Yang X, Shao J, Zhou X, Yuan J. Complicated appendicitis in children: is laparoscopic appendectomy appropriate? A comparative study with the open appendectomy-our experience. J Pediatr Surg [Internet]. 2009 [cited 2015 may 08];44(10):1924-7. doi: http://doi.org/b6h6gb.
Bröker ME, van Lieshout EM, van der Elst M, Stassen LP, Schepers T. Discriminating between simple and perforated appendicitis. J Surg Res [Internet]. 2012 [cited 2015 may 08];176(1):79-83. doi: http://doi.org/fgt577.
Snelling CMH, Poenaru D, Drover JW. Minimum postoperative antibiotic duration in advanced appendicitis in children: a review. Pediatr Surg Int [Internet]. 2004 [cited 2015 may 08];20(11-12):838-45. doi: http://doi.org/fr8cdt.
Lee SL, Shekherdimian S, Chiu VY, Sydorak RM. Perforated appendicitis in children: equal access to care eliminate racial and socioeconomic disparities. J Pediatr Surg [Internet]. 2010 [cited 2015 may 08];45(6):1203-7. doi: http://doi.org/cfb5fz.
Cómo citar
APA
ACM
ACS
ABNT
Chicago
Harvard
IEEE
MLA
Turabian
Vancouver
Descargar cita
CrossRef Cited-by
1. Luz Nélida Garzon-González, Laura Tatiana Padilla, Felipe Patiño, María Alejandra Hernández, Juan Valero, Iván Dario Molina, Fernando Fierro Ávila, German Camacho-Moreno. (2023). Association between bacterial resistance profile and the development of intra-abdominal abscesses in pediatric patients with perforated appendicitis: cohort study. Pediatric Surgery International, 40(1) https://doi.org/10.1007/s00383-023-05570-3.
2. Juan Valero, Giancarlo Buitrago, Javier Eslava‐Schmalbach, Carlos J. Rincon. (2020). Prognostic Factors Associated with Clinical and Economic Outcomes of Appendectomies in Children: A Multilevel Analysis in a National Retrospective Cohort Study. World Journal of Surgery, 44(1), p.303. https://doi.org/10.1007/s00268-019-05182-w.
3. Eliana Rodríguez, Juan Valero, Lina Jaramillo, María Teresa Vallejo-Ortega, Luisa Lagos. (2020). Evaluation of concordance among surgeons and pathologists regarding the diagnosis and classification of acute appendicitis in children. Journal of Pediatric Surgery, 55(8), p.1503. https://doi.org/10.1016/j.jpedsurg.2019.09.025.
4. Ana Fernanda Garcés , Fabio Camilo Suarez-Cadena, Fernando Fierro , Iván Darío Molina , Juan Javier Valero-Halaby. (2022). Factores predictores de apendicitis perforada en población pediátrica en un Hospital de referencia en Bogotá D.C., Colombia. Revista de la Facultad de Medicina, 71(2), p.e101309. https://doi.org/10.15446/revfacmed.v71n2.101309.
5. Juan Hernández-Orduña. (2020). Clasificación práctica de la gravedad y manejo médico-quirúrgico de la apendicitis aguda. Cirujano General, 42(4), p.263. https://doi.org/10.35366/101395.
Dimensions
PlumX
Visitas a la página del resumen del artículo
Descargas
Licencia
Derechos de autor 2015 Revista de la Facultad de Medicina

Esta obra está bajo una licencia Creative Commons Reconocimiento 3.0 Unported.
-


















