


Publicado
Competencia para cuidar en el hogar de personas con enfermedad crónica y sus cuidadores en Colombia
Competence for Home Health Care in Colombian People with Chronic Ilness and their Caregivers
DOI:
https://doi.org/10.15446/revfacmed.v63.n4.50322Palabras clave:
enfermedad crónica, cuidadores, alta del paciente, seguridad del paciente (es)Chronic Disease, Caregivers, Patient Discharge, Patient Safety (en)
Antecedentes. La competencia para el cuidado en el hogar es parte de las características fundamentales requeridas en la atención de personas con enfermedad crónica y se describe como la capacidad, habilidad y preparación que tiene el usuario o su cuidador familiar para ejercer la labor de cuidar.
Objetivo. Describir y comparar la competencia para cuidar en el hogar de personas con enfermedad crónica, así como la competencia de sus cuidadores familiares para atenderlas en el hogar.
Materiales y métodos. Estudio cuantitativo, descriptivo, comparativo y de corte transversal desarrollado entre 2012 y 2014 en las cinco regiones geográficas de Colombia. La muestra está compuesta de 2231 personas con enfermedad crónica y cuidadores familiares. Se emplearon los instrumentos Encuesta de caracterización para el cuidado de una diada persona con enfermedad crónica-cuidador familiar y Competencia para cuidar en el hogar GCPC-UN-CPC, versión paciente y cuidador familiar.
Del mismo modo, se utilizó estadística descriptiva para analizar la competencia para cuidar en el hogar y sus dimensiones a partir de los niveles de estratificación alto, medio y bajo; para la comparación se utilizaron pruebas no paramétricas en muestras independientes.
Resultados. Tanto las personas con enfermedad crónica como los cuidadores familiares tienen niveles heterogéneos de competencia para cuidar en el hogar en las diferentes regiones del país. En ambos casos los niveles superiores se encuentran en la Región Amazónica y los más bajos en la Pacífica. Estos niveles de competencia para cuidar en el hogar distan de ser adecuados para garantizar la calidad y seguridad que se requiere.
Conclusión. Los indicadores de cuidado continuo deben tener en cuenta la diada receptor-cuidador familiar y abordar el talento humano, las instituciones y al mismo sistema general de seguridad social en salud para modificar una realidad que, de no ser atendida, resultará agobiante para el país.
Background. The competence for home health care is part of the fundamental features required when taking care of people with chronic disease. It is described as the ability, the skill and the preparation the user or their family caregiver possesses in order to perform the work of caring.
Objective. To describe and compare the competence for home health care in Colombian people with chronic illness and their family caregivers in the different regions of Colombia.
Materials and Methods. Quantitative, descriptive, comparative and cross-sectional study conducted between 2012 and 2014 in the five geographical regions of Colombia. The sample consists of 2231 participants including people with chronic illness and family caregivers. The measurement instruments used were the Survey for the characterization of the caring Dyad patient - family caregiver GCPC-UN-D, and the Home health care competence instrument "GCPC-UN-CPC", both in its patient and family caregiver versions. Descriptive statistics were used to analyze the home health care competence. For comparison of the groups nonparametric tests for independent samples were used.
Results. People with chronic illness and their family caregivers have heterogeneous levels of home health caring competence in the different regions of Colombia. In both cases the higher levels are found in the Amazon region, while the lowest are found in the Pacific region. These levels of home health care competence are far away from the required ones to ensure quality and safety in the care of these patients.
Conclusion. The indicators for the evaluation of home health care competence must address patients and their family caregiver as well as the health human talent, health institutions and the Social Security System in order to understand in a better way and change the current vulnerability in home health care practices in the country.
DOI: https://doi.org/10.15446/revfacmed.v63.n4.50322
INVESTIGACIÓN ORIGINAL
Competencia para cuidar en el hogar de personas con enfermedad crónica y sus cuidadores en Colombia
Competence for Home Health Care in Colombian People with Chronic Ilness and their Caregivers
Gloria Mabel Carrillo-González1, Ruth Vivian Barreto-Osorio2, Ligia Betty Arboleda3, Oscar Alexander Gutiérrez-Lesmes4, Blanca Gregoria Melo5, Vilma Támara Ortiz6
1 Universidad Nacional de Colombia -Sede Bogotá - Facultad de Enfermería - Bogotá, D.C. - Colombia.
2 Universidad de Ciencias Aplicadas y Ambientales (U.D.C.A) - Facultad de Ciencias de la Salud - Programa de Enfermería - Bogotá, D.C. - Colombia.
3 Universidad de Santander (UDES) - Sede Bucaramanga - Facultad de Ciencias de la Salud - Enfermería - Bucaramanga - Colombia.
4 Universidad de los Llanos - Facultad de Ciencias de la Salud Escuela de Salud Pública - Villavicencio - Colombia.
5 Universidad de Cundinamarca - Sede Girardot. Facultad de Ciencias de la Salud- Programa de Enfermería - Girardot - Colombia.
6 Universidad Mariana Enfermera - Facultad de Ciencias de la Salud - Enfermería - San Juan de Pasto - Colombia.
Correspondencia: Gloria Mabel Carrillo-González. Facultad de Enfermería, Universidad Nacional de Colombia. Carrera 30 No. 45-03. Teléfono: +57 1 3165000, extensión: 10340. Bogotá, D.C. Colombia. Correo electrónica: gmcarrillog@unal.edu.co.
Recibido: 29/04/2015 Aceptado: 18/06/2015
Resumen
Antecedentes. La competencia para el cuidado en el hogar es parte de las características fundamentales requeridas en la atención de personas con enfermedad crónica y se describe como la capacidad, habilidad y preparación que tiene el usuario o su cuidador familiar para ejercer la labor de cuidar.
Objetivo. Describir y comparar la competencia para cuidar en el hogar de personas con enfermedad crónica, así como la competencia de sus cuidadores familiares para atenderlas en el hogar.
Materiales y métodos. Estudio cuantitativo, descriptivo, comparativo y de corte transversal desarrollado entre 2012 y 2014 en las cinco regiones geográficas de Colombia. La muestra está compuesta de 2231 personas con enfermedad crónica y cuidadores familiares. Se emplearon los instrumentos Encuesta de caracterización para el cuidado de una diada persona con enfermedad crónica-cuidador familiar y Competencia para cuidar en el hogar GCPC-UN-CPC, versión paciente y cuidador familiar.
Del mismo modo, se utilizó estadística descriptiva para analizar la competencia para cuidar en el hogar y sus dimensiones a partir de los niveles de estratificación alto, medio y bajo; para la comparación se utilizaron pruebas no paramétricas en muestras independientes.
Resultados. Tanto las personas con enfermedad crónica como los cuidadores familiares tienen niveles heterogéneos de competencia para cuidar en el hogar en las diferentes regiones del país. En ambos casos los niveles superiores se encuentran en la Región Amazónica y los más bajos en la Pacífica. Estos niveles de competencia para cuidar en el hogar distan de ser adecuados para garantizar la calidad y seguridad que se requiere.
Conclusión. Los indicadores de cuidado continuo deben tener en cuenta la diada receptor-cuidador familiar y abordar el talento humano, las instituciones y al mismo sistema general de seguridad social en salud para modificar una realidad que, de no ser atendida, resultará agobiante para el país.
Palabras clave: Enfermedad crónica; Cuidadores; Alta del paciente; Seguridad del paciente (DeCS).
Carrillo-González GM, Barreto-Osorio RV, Arboleda LB, Gutiérrez-Lesmes OA, Melo BG, Ortiz VT. Competencia para cuidar en el hogar de personas con enfermedad crónica y sus cuidadores en Colombia. Rev. Fac. Med. 2015;63(4):665-75. Spanish. doi: https://doi.org/10.15446/revfacmed.v63.n4.50322.
Summary
Background. The competence for home health care is part of the fundamental features required when taking care of people with chronic disease. It is described as the ability, the skill and the preparation the user or their family caregiver possesses in order to perform the work of caring.
Objective. To describe and compare the competence for home health care in Colombian people with chronic illness and their family caregivers in the different regions of Colombia.
Materials and Methods. Quantitative, descriptive, comparative and cross-sectional study conducted between 2012 and 2014 in the five geographical regions of Colombia. The sample consists of 2231 participants including people with chronic illness and family caregivers. The measurement instruments used were the Survey for the characterization of the caring Dyad patient - family caregiver GCPC-UN-D, and the Home health care competence instrument "GCPC-UN-CPC", both in its patient and family caregiver versions. Descriptive statistics were used to analyze the home health care competence. For comparison of the groups nonparametric tests for independent samples were used.
Results. People with chronic illness and their family caregivers have heterogeneous levels of home health caring competence in the different regions of Colombia. In both cases the higher levels are found in the Amazon region, while the lowest are found in the Pacific region. These levels of home health care competence are far away from the required ones to ensure quality and safety in the care of these patients.
Conclusion. The indicators for the evaluation of home health care competence must address patients and their family caregiver as well as the health human talent, health institutions and the Social Security System in order to understand in a better way and change the current vulnerability in home health care practices in the country.
Keywords: Chronic Disease; Caregivers; Patient Discharge; Patient Safety (MeSH).
Carrillo-González GM, Barreto-Osorio RV, Arboleda LB, Gutiérrez-Lesmes OA, Melo BG, Ortiz VT. [Competence for Home Health Care in Colombian People with Chronic Ilness and their Caregivers]. Rev. Fac. Med. 2015;63(4):665-75. Spanish. doi: https://doi.org/10.15446/revfacmed.v63.n4.50322.
Introducción
71% de las muertes en Colombia se presentan asociadas con una enfermedad crónica (1); estas dolencias son complejas, se prolongan en el tiempo y, por lo general, demandan apoyos de cuidado (2). Se ha documentado que en América Latina las personas con enfermedad crónica son atendidas especialmente por integrantes de la familia, quienes en muchos casos no tienen la habilidad ni los soportes requeridos para asumir estas responsabilidades de cuidado (3), es por ello que la necesidad de ofertar a los pacientes un cuidado seguro, continuo e integral es prioritaria (4).
Se identifican cuatro categorías que dan cuenta del estado actual de conocimiento (5) en la competencia para cuidar en el hogar y en los planes de alta hospitalaria:
1. Se aceptan la importancia y la pertinencia de desarrollar planes de transición y egreso como elementos fundamentales en el cuidado de los pacientes y la orientación de sus familiares; se refleja falta de claridad en la forma de estructurar dichos planes.
2. Se han desarrollado instrumentos para la valoración y medición de aspectos relacionados con el plan de transición y egreso hospitalario; sin embargo, no han sido construidos ni validados para Latinoamérica.
3. Se reconocen características básicas de los elementos que debe tener un plan de transición hospitalario, especificando que el egreso es un momento de mayor riesgo para el cuidado seguro y continuo de los pacientes y sus familia (6-8). Se resalta la importancia de fortalecer el autocuidado y de tener directrices para orientar la práctica.
4. Se identifica como beneficio del plan de egreso para los pacientes y sus familias el favorecimiento de la calidad en el cuidado de la salud. (9-11)
Teniendo en cuenta estos referentes, el objetivo del estudio fue describir y comparar cuál es el nivel de competencia para cuidar en el hogar de personas con enfermedad crónica, así como la competencia de sus familiares para atenderlas en Colombia.
Método
El estudio se desarrolló entre los años 2012 y 2014 en el marco del Programa para la Disminución de la Carga de la Enfermedad Crónica en Colombia, con participación de integrantes de la Red Latinoamericana de Cuidado al Paciente Crónico; contó con los respectivos avales éticos y mantuvo todos los requisitos exigidos por la Resolución 8430 de 1993 para la investigación en salud en Colombia (12). Adicionalmente, sus autores se comprometieron con la política de protección del medio ambiente y en especial con el uso racional de recursos (13).
Su abordaje es cuantitativo, de tipo descriptivo-comparativo y de corte transversal. Se estudió y comparó la competencia para el cuidado en el hogar en las cinco regiones geográficas de Colombia, acogiendo para ello los esquemas propuestos por el Instituto Geográfico Agustín Codazzi (IGAC) y que fueron ampliamente conceptualizados para la familia colombiana por Gutiérrez de Pineda (14). Su muestra estuvo conformada por 959 personas con enfermedad crónica (EC) y 1272 cuidadores familiares (CF) de enfermos crónicos captados desde programas docente-asistenciales de enfermería como se ilustra en la Tabla 1.

En la descripción de las personas enfermas y sus cuidadores se empleó la Encuesta de caracterización para el cuidado de la diada persona con enfermedad crónica-cuidador familiar, que contiene tres dimensiones: condiciones y perfil socio demográfico de la diada, percepción de carga y apoyo y apropiación de las tecnologías de información y comunicación (TIC); esta fue desarrollada y validada en el contexto de América Latina (15).
Las condiciones y el perfil sociodemográfico incluyen las variables funcionalidad de la diada, género, diagnósticos médicos, edad, escolaridad, procedencia, estado civil, ocupación, estrato socioeconómico, tiempo que lleva con la EC y compromiso religioso.
El componente de percepción de carga y apoyo comprende las variables número de horas de ayuda que se requiere para el cuidado, tiempo como cuidador, número de horas de dedicación al cuidado, percepción de carga del paciente y el cuidador, nivel de bienestar percibido, apoyos y satisfacción respecto a estos.
En la dimensión de apropiación de las tecnologías de información y comunicación (TIC) se incluye autovaloración de la diada en el uso, acceso y apropiación con estas, así como el nivel de apoyo percibido.
Para medir la competencia para cuidar en el hogar se empleó la versión abreviada del instrumento de la Universidad Nacional de Colombia GCPC-UN-CPC en sus versiones paciente y cuidador familiar. Este instrumento considera que la competencia para cuidar en el hogar es la capacidad, habilidad y preparación que tiene la persona con enfermedad crónica o su cuidador familiar para ejercer la labor de cuidar en su sitio de vivienda. La versión empleada consta de 20 ítems que miden —con una escala tipo likert puntuaciones de 1 a 4, donde 4 es el máximo valor posible— seis categorías complementarias entre sí y que se encuentran ordenadas bajo el acróstico CUIDAR así: Conocimiento, Unicidad o condiciones particulares, Instrumental procedimental, Disfrute de condiciones mínimas para el cuidado o nivel de bienestar, Anticipación, y Relación social e interacción. El instrumento cuenta con las pruebas psicométricas necesarias para ser usado en Colombia, incluidas validez aparente, validez de constructo y confiabilidad. Para esta aplicación se obtuvo una consistencia interna dada por un alfa de Cronbach de 0.96 (16).
Los participantes fueron abordados por los investigadores o auxiliares de investigación; la aplicación de los instrumentos se realizó mediante entrevista directa, previa explicación de los objetivos del estudio y acogiendo para cada caso el procedimiento del consentimiento informado.
La información fue acopiada en base de datos de Excel mediante riguroso proceso de control de calidad, posteriormente fue procesada en el programa SPSS versión 19.0 con licencia de la Universidad Nacional de Colombia.
Los análisis incluyeron estadísticas descriptivas utilizando medidas de tendencia central y de dispersión para la totalidad del instrumento y las dimensiones. La competencia para cuidar en el hogar se analizó a partir de los niveles de estratificación alto, medio y bajo. Al evaluar la competencia para cuidar en el hogar, y con fines de comparación entre dimensiones, se realizó una estandarización de las variables en porcentaje. Para la comparación de las regiones y grupos se aplicó la prueba no paramétrica de Kruskal-Wallis y la prueba Chi cuadrado.
Resultados
A continuación se presentan los resultados principales de la caracterización y de la competencia para cuidar en el hogar de las personas con enfermedad crónica (EC) y la de los cuidadores Familiares (CF) por regiones del país.
Personas con enfermedad crónica
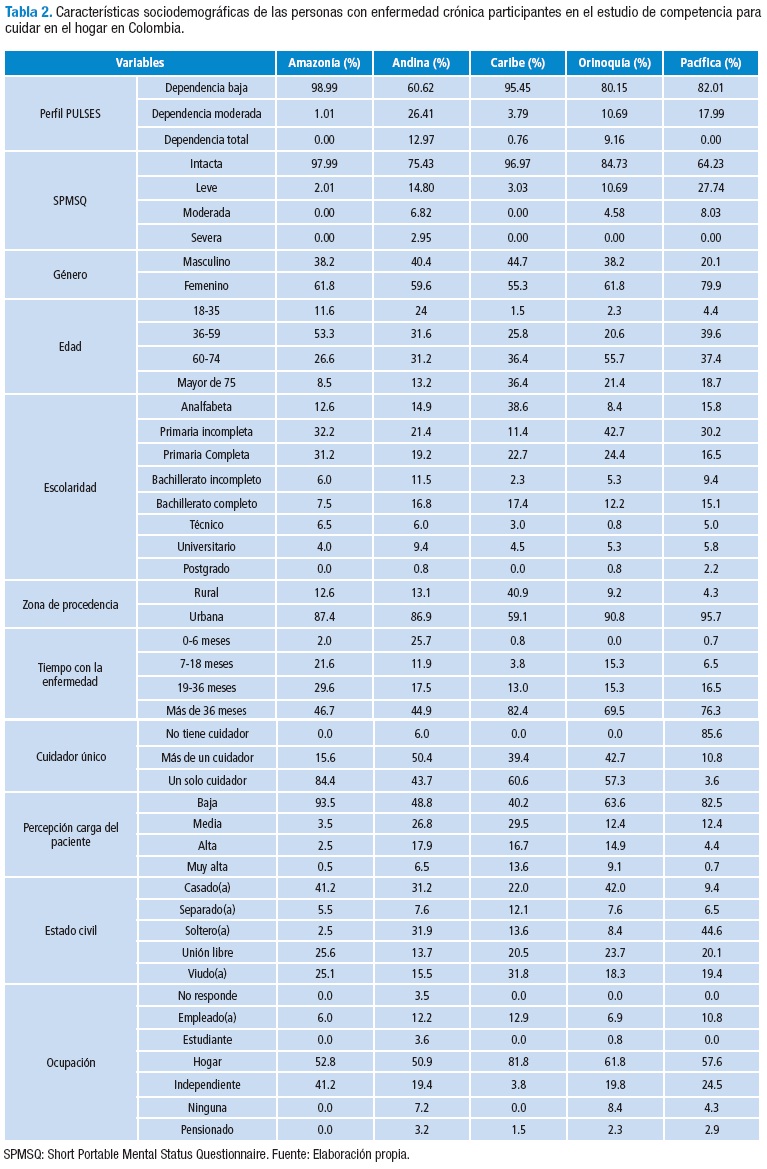
En la Tabla 2 se describen algunos de los aspectos sociodemográficos de las personas con EC de las cinco regiones del país que participaron en la descripción de la competencia para cuidar en el hogar.
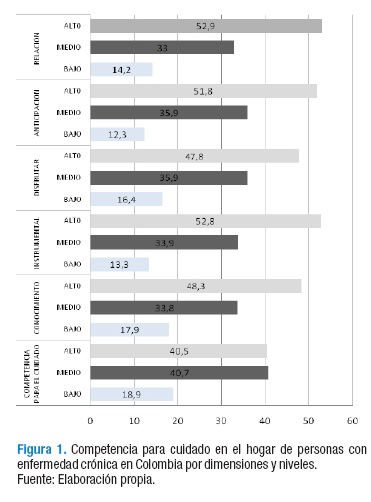
Al evaluar la competencia para cuidar en el hogar, previa estandarización que dio puntajes posibles de 0 a 100, las personas con EC a nivel nacional obtuvieron una media general de 75.62%. Al revisar la competencia para cuidar en el hogar por niveles, se identificó que solo 40.3% de las personas con EC presenta alto nivel de competencia para cuidar en el hogar, 59.7 % reportan un nivel que se puede considerar no óptimo, dado por un 40.8% con nivel medio y un 18.9% con un nivel bajo.
Al revisar las dimensiones, únicamente en el componente de relación y en el de anticipación, cerca de 50% de los participantes reportan niveles altos. Estos hallazgos señalan la necesidad de fortalecer la competencia para cuidar en el hogar de personas con EC en todas sus dimensiones, Figura 1.
Al realizar el análisis por regiones, se identifica que la competencia para cuidar en el hogar en las personas con enfermedad crónica de la Región Pacifica es el más bajo, seguido por la Región Caribe, Andina, Orinoquía y Amazonía respectivamente.
Los valores más altos, en general y por dimensiones, se obtuvieron en la Región Amazonía, hallazgos relacionados probablemente con las características de los enfermos crónicos participantes en el estudio de dicha región: la mayoría con estabilidad de su enfermedad, sin evidentes complicaciones reportadas y con altos niveles de independencia y funcionalidad. Podría también considerarse que ante la falta de recursos de salud, las personas adquieren mayor capacidad de autocuidado, Figura 2.
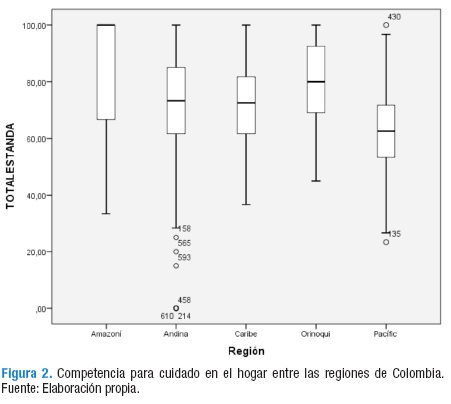
La competencia para cuidar en el hogar en personas con enfermedad crónica presenta los niveles más bajos en la Región Pacífico —hallazgo que es estadísticamente significativo—, seguida por la Región Andina, Caribe y Orinoquía. Por otro lado, es llamativo el alto nivel de competencia para cuidar en el hogar reportado en la Amazonía, correspondiente al 73%. A pesar de esta particularidad, los resultados generales evidencian la importancia de fortalecer la competencia para cuidar en el hogar en personas con EC en todas las regiones de Colombia, Figura 3

Al realizar la comparación de las regiones utilizando la prueba no paramétrica de Kruskal Wallis para muestras independientes, se confirmó que la competencia para cuidar en el hogar de personas con enfermedad crónica, en general y por cada una de sus dimensiones, es diferente en cada una las regiones geográficas del país con un valor p menor a 0.05. (p<0.00). Al análisis con la prueba Chi cuadrado se identificó que la región geográfica donde habitan las personas con EC en Colombia modula o influye en la categorización de la competencia para cuidar en el hogar y en cada una de sus dimensiones. Así mismo es evidente que los niveles de competencia encontrados en todo el país distan mucho de los que son requeridos para garantizar un cuidado de calidad.
Cuidadores familiares de personas con enfermedad crónica
En la Tabla 3 se describen los aspectos generales de la caracterización sociodemográfica de los CF de personas con EC que participaron en el estudio de la competencia para cuidar en el hogar por regiones del país.
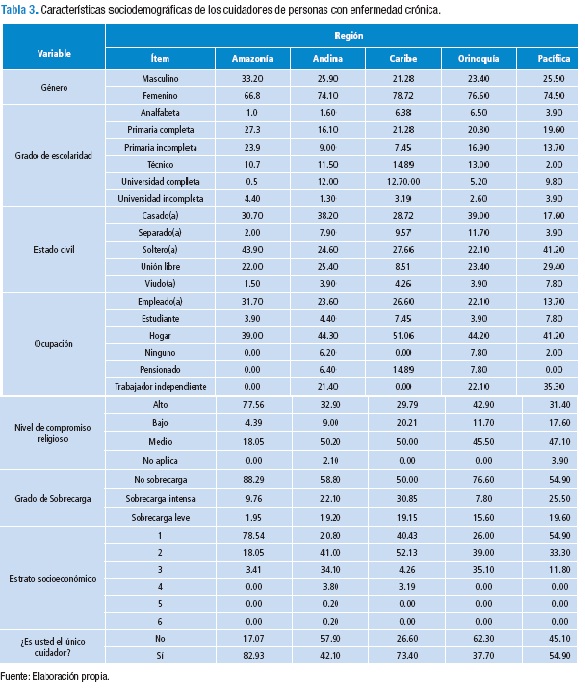
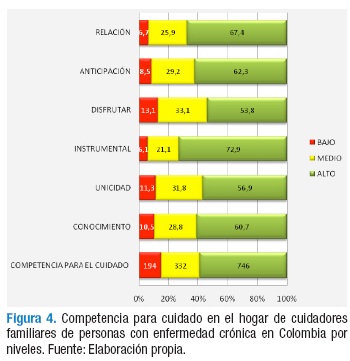
Al evaluar la competencia para cuidar en el hogar, previa estandarización que dio puntajes posibles de 0 a 100, los resultados de los CF de personas con enfermedad crónica participantes del estudio a nivel nacional indican una media en la competencia general de 85.44%. Respecto a la dimensión Conocimiento se encontró un promedio de 82.45%, en Unicidad 84.31%, en Instrumental 88.53%, en Disfrutar 83.16%, en Anticipación 86.43% y Relación e interacción 88.29%.
En la valoración por niveles se identificó que 58.6% de los cuidadores presenta un alto nivel de competencia para cuidar en el hogar, mientras el 41.4% no cuenta con un nivel óptimo. De este segundo grupo el 26.1% reportó un nivel medio y el 15.3% un nivel bajo. Las dimensiones de unicidad —condiciones personales— y disfrute de condiciones mínimas para el cuidado —bienestar— reportan los niveles más bajos, Figura 4.
Al realizar el análisis por regiones se evidencia que la competencia para cuidar en el hogar de los CF en la Región Pacífico es la más baja, seguida por la de los de Caribe, Andina, Orinoquía y Amazonía respectivamente, Figura 5.

Al realizar la comparación entre las cinco regiones de Colombia con la prueba de Kruskal Wallis de muestras independientes, se identifica que la distribución de la competencia para cuidar en el hogar de los cuidadores de personas con enfermedad crónica no es igual en las cinco regiones, (p<0.05); el análisis con la prueba Chi cuadrado indica que la región influye en la categorización de esta competencia.
Finalmente, al comparar la competencia para el cuidado en el hogar de personas con EC y la competencia de los CF para cuidar de estas personas, se identifica que son diferentes en su totalidad y en cada una de las dimensiones (p<0.00). Se reconoce, además, que los cuidadores familiares presentan niveles más altos de competencia que las personas con enfermedad crónica.
Discusión
Parte de lo que establecen los lineamientos mundiales para el cuidado crónico es la importancia de garantizar continuidad, seguridad e integralidad, condiciones que retomó el modelo para la disminución de la carga del cuidado de la EC en Colombia (17).
Las personas con EC y sus CF asumen responsabilidades de cuidado en coparticipación, negociación y con procesos de adaptación permanente frente a la evolución e implicaciones de la EC (18-19).
La enfermedad crónica se caracteriza por estar en incremento y mantenerse en el tiempo; en tal sentido, las relaciones de cuidado deben ser analizadas en diadas CF-receptor del cuidado, las cuales surgen como una opción del desarrollo humano en las que se requieren de dos personas o, en el caso del autocuidado, un diálogo interno con el propio ser, tal como ha sido descrito en población colombiana (20). Una vez inicia la dependencia funcional se van generando acciones mutuas a partir de un contrato que en la mayor parte de los casos es tácito y que llevan a tener mutualidad y reciprocidad que generan y mantienen un vínculo especial (21,22).
En este estudio es evidente que la competencia de cuidar en el hogar es superior en los cuidadores familiares que en los receptores del cuidado, sin embargo es preciso recordar que ser CF afecta a lo largo del tiempo la salud de las personas que ejercen este rol. (23)
Al comparar los hallazgos con la literatura revisada se puede establecer que este estudio, al igual que los anteriores, ratifica la importancia y pertinencia de desarrollar no solamente planes de transición y egreso como elemento fundamental en el cuidado de los pacientes y para la orientación de sus familiares (24-32), sino que se requiere una política de carácter nacional. El aporte del instrumento GCPC-UN-CPC como lineamiento de los mínimos puede servir de orientación para su estructuración.
El instrumento empleado en el presente estudio permite complementar los desarrollos referidos en el estado del arte y, a diferencia de estos, cumple con las características de integralidad, seguridad y continuidad, además de tener sus pruebas psicométricas en español.
Valorar la competencia de cuidar en el hogar aporta a los estudios de conceptualización de los elementos que debe tener un plan de transición y egreso hospitalario (33-38) y apoya el reconocimiento sobre la relevancia de la transición y el egreso como unos de los momentos de mayor riesgo para el cuidado seguro y continuo de los pacientes y sus familias (39-42). En este caso, el estudio ofrece pautas para fortalecer la competencia de cuidar en el hogar y para cualificar la práctica.
Por último, aunque el presente estudio solo pretendió conocer y comparar las competencias de cuidado de las personas con EC y la competencia de los CF para cuidar de estas personas, el potencial que abre puede llegar a ser un aporte significativo para aumentar y documentar los beneficios del plan de egreso para estas personas. (43-45)
Conclusiones
Este trabajo eligió la condición cuidado continuo, establecida por el modelo, para abordar la carga del cuidado de la enfermedad crónica en Colombia.
Los hallazgos reflejan que los pacientes y cuidadores tienen niveles de competencia heterogénea, que esta es diferente de acuerdo con las regiones del país y que dista de manera importante de ser adecuada para asumir el rol de cuidado garantizando calidad y seguridad en el mismo. En tal sentido, los indicadores de cuidado continuo deben tener en cuenta a la persona con EC, su cuidador familiar, la diada receptor-cuidador familiar, pero también debe abordar el talento humano, las instituciones y al mismo sistema general de seguridad social en salud para modificar una realidad que, de no ser atendida, resultará agobiante en el país.
Conflicto de intereses
Ninguno declarado por los autores.
Financiación
Este estudio fue financiado por el programa para disminuir la carga de la enfermedad crónica en Colombia. Convocatoria 537- 2010 Colciencias. Unión Temporal Carga de la Enfermedad Crónica en Colombia.
Agradecimientos
A los integrantes de la Red Latinoamericana de Cuidado al paciente crónico y su familia y de la Unión Temporal Carga de la Enfermedad Crónica en Colombia.
Referencias
1. Organización Mundial de la Salud. Noncommunicable Diseases Country Profiles 2014. Ginebra : OMS; 2014.
2. Barrera-Ortiz L, Galviz-López CR, Moreno-Fergusson ME, Pinto-Afandor N, Pinzón-Rocha ML, Romero-González E, et al. La habilidad de cuidado de los cuidadores familiares de personas con enfermedad crónica. Investigación y educación en Enfermería. 2006;23(1):36-46.
3. Barrera-Ortiz L, Blanco-de Camargo L, Figueroa-Ingrid P, Pinto-Afanador N, Sánchez-Herrera B. Habilidad de cuidado de los cuidadores familiares de personas con enfermedad crónica. Mirada internacional. Aquichan. 2006;6(1):22-33.
4. Sánchez B. Cuidado seguro: la nueva tendencia en el cuidado de la salud. Actual. Enferm. 2011;14(2):27-32.
5. Sánchez B, Carrillo GM, Barrera L. El plan de transición y egreso hospitalario y su efecto en el cuidado de la salud: una revisión integrada. Rev. U.D.C.A. Act. & Div. Cient. 2014;17(1):13-23.
6. Tellett L, Pyle L, Coombs M. End of life in intensive care: is transfer home an alternative? Intensive Crit. Care Nurs. 2012;28(4):234-241. http://doi.org/8x7.
7. Oliver D. Medical input, rehabilitation and discharge planning for patients with hip fracture: Why traditional models are not fit for purpose and how things are changing. Current Anaesthesia & Critical Care. 2005;16(1):11-22. http://doi.org/crhjs4.
8. Vargas-Bermúdez Z., Fernández-Coto R. Programa de alta hospitalaria programada para preparar el egreso del paciente y familia. Enfermería Actual de Costa Rica. 2011;21:1-20. http://doi.org/8x8.
9. Thraena I, Bairb B, Mullinc S, Weir CR. Characterizing "information transfer" by using a Joint Cognitive Systems model to improve continuity of care in the aged. Int. J. Med. Inform. 2012;81(7):435-41. http://doi.org/fxzvrz.
10. Koelling TM, Johnson ML, Cody RJ, Aaronson KD. Discharge education improves clinical outcomes in patients with chronic heart failure. Circulation. 2005; 111(2):179-185. http://doi.org/fkr7qf.
11. Thrutchley D, DeLong D, Rymer M. Stroke home health care: The transition to independence. J. Stroke Cerebrovasc. Dis. 1997;6(6):465. http://doi.org/dc6wxt.
12. República de Colombia. Ministerio de Salud. Resolución 8430 de 1993 (octubre 4): Por la cual se establecen las normas científicas, técnicas y administrativas para la investigación en salud. Bogotá, D.C.; Octubre 4 de 1993 [cited 2013 Mar 23]. Available from: http://goo.gl/rt5xgm.
13. República de Colombia. Universidad Nacional de Colombia, Consejo Superior Universitario. Acuerdo 016 de 2011 (octubre 18): Por el cual se establece la Política Ambiental de la Universidad Nacional de Colombia. Bogotá, D.C.: Sistema de Información Normativa, Jurisprudencial y de Conceptos "Régimen Legal"; octubre 18 de 2011 [cited 2013 Mar 23]. Available from: http://goo.gl/3XVkWv.
14. Gutiérrez- de Pineda V. Familia y cultura en Colombia; tipologías, funciones y dinámica de la familia: Manifestaciones múltiples a través del mosaico cultural y sus estructuras sociales. Bogotá, D.C.: Instituto Colombiano de Cultura, Subdirección de Comunicaciones Culturales; 1975.
15. Carrillo-González GM, Chaparro L, Sánchez B. Encuesta de caracterización del cuidado de la diada cuidador familiar-persona con enfermedad crónica. Revista Ciencia y Cuidado. 2014;11(2):31-45.
16. Carrillo GM, Sánchez-Herrera B, Arias-Rojas EM. Validation of an instrument to assess the homecare competency of the family caregiver of a person with chronic disease. Invest. Educ. Enferm. 2015; 33(3): 449-455. http://doi.org/87m.
17. Arias M, Sánchez B. Las cinco características necesarias para ofrecer cuidado institucional en situaciones de enfermedad crónica. Experiencias de formación e investigación para el cuidado de enfermería. Bogotá, D.C.: Universidad Nacional de Colombia; 2013.
18. Shyu YL. The needs of family caregiver of frail elders during the transition from hospital to home: a Taiwanese sample. J. Adv. Nurs. 2000;32(3):619-25. http://doi.org/cvhgpm.
19. Shyu YL. Role tuning between caregiver and care receiver during discharge transition: An illustration of role function mode in Roy's Adaptation Theory. Nurs. Sci. Q. 2000;13(4):323-31. http://doi.org/fmkbzt.
20. Chaparro-Díaz L. El vínculo especial de cuidado: construcción de una teoría fundamentada. Avances en Enfermería. 2010;28(2):23-33.
21. Lazar A, Demiris G, Thompson HJ. Involving family members in the implementation and evaluation of technologies for dementia: a dyad case study. J. Gerontol. Nurs. 2015;41(4):21-6. http://doi.org/8zd.
22. Chaparro-Díaz L. Cómo se constituye el "vínculo especial" de cuidado entre la persona con enfermedad crónica y el cuidador familiar. Aquichan. 2011.11(1):7-22. http://doi.org/wk3.
23. López-Gil MJ, Orueta-Sánchez R, Gómez-Caro S, Sánchez-Oropesa A, Carmona-de la Morena J, Alonso-Moreno FJ. El rol de Cuidador de personas dependientes y sus repercusiones sobre su Calidad de Vida y su Salud. Rev. Clin. Med. Fam. 2009.2(7):332-9.
24. Lin F, Chaboyer W, Wallis M. A literature review of organizational, individual and teamwork factors contributing to the ICU discharge process. Aust. Crit. Care. 2009;22 (1):29-43. http://doi.org/bdd6kj.
25. Chen J, Ross JS, Carlson MD, Lin Z, Normand SL, Bernhein SM, et al. Skilled nursing facility referral and hospital readmission rates after heart failure or myocardial infarction. Am. J. Med. 2012;125(1):100-9. http://doi.org/fzxqfp.
26. Foust JB. Discharge planning as part of daily nursing practice. Appl. Nurs. Res. 2007;20(2):72-7. http://doi.org/dvbhf2.
27. Han CY, Barnard A, Chapman H. Discharge planning in the emergency department: a comprehensive approach. J. Emerg. Nurs. 2009;35 (6):525-7. http://doi.org/fm4bq5.
28. Collier EJ. Harrington C. Discharge planning, nursing home placement and the Internet. Nurs Outlook. 2005;53(2):95-103. http://doi.org/fpsvz6.
29. Pichitpornchaia W, Street A, Boontong T. Discharge planning and transitional care: issues in Thai nursing. Int. J. Nurs. Stud. 1999;36(5):355-62. http://doi.org/fmvh83.
30. Hanratty B, Holmes L, Lowson E, Grande G, Addington-hall J, Payne S, et al. Older adults' experiences of transitions between care settings at the end of life in england: a qualitative interview study. J. Pain Symptom Manage. 2012;44(1):74-83. http://doi.org/8zf.
31. Krohn DA. Discharge Instructions in the Outpatient Setting: Nursing Considerations. J Radiology Nursing. 2008;27(1):29-33. http://doi.org/8zg.
32. Adib-Hajbaghey M, Maghaminejad F, Abbasi A. The role of continuous care in reducing readmission for patients with heart failure. J. Caring Sci. 2013 Nov 30 2(4): 255-67. http://doi.org/87n.
33. Annells M, Koch T, Brown M. Client relevant care and quality of life: the trial of a Client Generated Index (CGI) tool for community nursing. Int. J. Nurs. Stud. 2001;38(1):9-16. http://doi.org/cx449q.
34. Kenner C, Boykova M. Transition to Home: Family Perspectives on Care in Russia. Newborn Infant Nurs. Rev. 2007;7(1):20-24. http://doi.org/cj2h3q.
35. Senarath U, Gunawardena NS. Development of an Instrument to Measure Patient Perception of the Quality of Nursing Care and Related Hospital Services at the National Hospital of Sri Lanka. Asian Nurs. Res. 2011;5(2):71-80. http://doi.org/d6vw3v.
36. Bobay KL, Jerofke TA, Weiss ME, Yakusheva O. Age-Related Differences in Perception of Quality of Discharge Teaching and Readiness for Hospital Discharge. Geriatr. Nurs. 2010.31(3):178-87. http://doi.org/bz32q4.
37. McMurray A, Johnson P, Wallis M, Patterson E, Griffiths S. General surgical patients' perspectives of the adequacy and appropriateness of discharge planning to facilitate health decision-making at home. J. Clin. Nurs. 2007;16(9):1602-9. http://doi.org/d9ccfz.
38. Hadjistavropoulos HD, Garratt S, Janzen JA, Bourgault-fagnou MD, Spice K. Development and evaluation of a Continuity of Care Checklist for improving orthopaedic patient discharge from hospital. Journal of Orthopaedic Nursing. 2009;13(4):183-93. http://doi.org/cqt6pq.
39. Hauser JM. Lost in Transition: The Ethics of the Palliative Care Handoff. J. Pain Symptom Manage. 2009;37(5):930-3. http://doi.org/b4pcj6.
40. Crocker JB, Crocker JT, Greenwald JL. Telephone Follow-up as a Primary Care Intervention for Postdischarge Outcomes Improvement: A Systematic Review. Am. J. Med. 2012;125(9):915-21. http://doi.org/8zj.
41. Jacob E. Making the Transition from Hospital to Home: caring for the Newly diagnosed child with cancer. Home Care Prov. 1999;4(2):67-73. http://doi.org/d6cp3m.
42. Baker EB, Wellman NS. Nutrition Concerns in Discharge Planning for Older Adults: A Need for Multidisciplinary Collaboration. J. Am. Diet. Assoc. 2005;105 (4):603-7. http://doi.org/bxh9zm.
43. Bull MJ, Hansen HE, Gross CR. A Professional-Patient Partnership Model of Discharge Planning with elders hospitalized with heart failure. Appl. Nurs. Res. 2000;13(1):19-28. http://doi.org/chhj9f.
44. Ben-Morderchai B, Herman A, Kerzman H, Irony A. Structured discharge education improves early outcome in orthopedic patients. Int. J. Orthop. Trauma Nurs. 2010;14(2):66-74. http://doi.org/d2b5rc.
45. Hiskett G. Clinical and economic consequences of discharge from hospital with on-going TNP therapy: a pilot study. J. Tissue Viability. 2010;19(1):16-21. http://doi.org/dtshg4.
Referencias
Organización Mundial de la Salud. Noncommunicable Diseases Country Profiles 2014. Ginebra : OMS; 2014.
Barrera-Ortiz L, Galviz-López CR, Moreno-Fergusson ME, Pinto-Afandor N, Pinzón-Rocha ML, Romero-González E, et al. La habilidad de cuidado de los cuidadores familiares de personas con enfermedad crónica. Investigación y educación en Enfermería. 2006;23(1):36-46.
Barrera-Ortiz L, Blanco-de Camargo L, Figueroa-Ingrid P, Pinto-Afanador N, Sánchez-Herrera B. Habilidad de cuidado de los cuidadores familiares de personas con enfermedad crónica. Mirada internacional. Aquichan. 2006;6(1):22-33.
Sánchez B. Cuidado seguro: la nueva tendencia en el cuidado de la salud. Actual. Enferm. 2011;14(2):27-32.
Sánchez B, Carrillo GM, Barrera L. El plan de transición y egreso hospitalario y su efecto en el cuidado de la salud: una revisión integrada. Rev. U.D.C.A. Act. & Div. Cient. 2014;17(1):13-23.
Tellett L, Pyle L, Coombs M. End of life in intensive care: is transfer home an alternative? Intensive Crit. Care Nurs. 2012;28(4):234-241. http://doi.org/8x7.
Oliver D. Medical input, rehabilitation and discharge planning for patients with hip fracture: Why traditional models are not fit for purpose and how things are changing. Current Anaesthesia & Critical Care. 2005;16(1):11-22. http://doi.org/crhjs4.
Vargas-Bermúdez Z., Fernández-Coto R. Programa de alta hospitalaria programada para preparar el egreso del paciente y familia. Enfermería Actual de Costa Rica. 2011;21:1-20. http://doi.org/8x8.
Thraena I, Bairb B, Mullinc S, Weir CR. Characterizing "information transfer" by using a Joint Cognitive Systems model to improve continuity of care in the aged. Int. J. Med. Inform. 2012;81(7):435-41. http://doi.org/fxzvrz.
Koelling TM, Johnson ML, Cody RJ, Aaronson KD. Discharge education improves clinical outcomes in patients with chronic heart failure. Circulation. 2005; 111(2):179-185. http://doi.org/fkr7qf.
Thrutchley D, DeLong D, Rymer M. Stroke home health care: The transition to independence. J. Stroke Cerebrovasc. Dis. 1997;6(6):465. http://doi.org/dc6wxt.
República de Colombia. Ministerio de Salud. Resolución 8430 de 1993 (octubre 4): Por la cual se establecen las normas científicas, técnicas y administrativas para la investigación en salud. Bogotá, D.C.; Octubre 4 de 1993 [cited 2013 Mar 23]. Available from: http://goo.gl/rt5xgm.
República de Colombia. Universidad Nacional de Colombia, Consejo Superior Universitario. Acuerdo 016 de 2011 (octubre 18): Por el cual se establece la Política Ambiental de la Universidad Nacional de Colombia. Bogotá, D.C.: Sistema de Información Normativa, Jurisprudencial y de Conceptos "Régimen Legal"; octubre 18 de 2011 [cited 2013 Mar 23]. Available from: http://goo.gl/3XVkWv.
Gutiérrez- de Pineda V. Familia y cultura en Colombia; tipologías, funciones y dinámica de la familia: Manifestaciones múltiples a través del mosaico cultural y sus estructuras sociales. Bogotá, D.C.: Instituto Colombiano de Cultura, Subdirección de Comunicaciones Culturales; 1975.
Carrillo-González GM, Chaparro L, Sánchez B. Encuesta de caracterización del cuidado de la diada cuidador familiar-persona con enfermedad crónica. Revista Ciencia y Cuidado. 2014;11(2):31-45.
Carrillo GM, Sánchez-Herrera B, Arias-Rojas EM. Validation of an instrument to assess the homecare competency of the family caregiver of a person with chronic disease. Invest. Educ. Enferm. 2015; 33(3): 449-455. http://doi.org/87m.
Arias M, Sánchez B. Las cinco características necesarias para ofrecer cuidado institucional en situaciones de enfermedad crónica. Experiencias de formación e investigación para el cuidado de enfermería. Bogotá, D.C.: Universidad Nacional de Colombia; 2013.
Shyu YL. The needs of family caregiver of frail elders during the transition from hospital to home: a Taiwanese sample. J. Adv. Nurs. 2000;32(3):619-25. http://doi.org/cvhgpm.
Shyu YL. Role tuning between caregiver and care receiver during discharge transition: An illustration of role function mode in Roy's Adaptation Theory. Nurs. Sci. Q. 2000;13(4):323-31. http://doi.org/fmkbzt.
Chaparro-Díaz L. El vínculo especial de cuidado: construcción de una teoría fundamentada. Avances en Enfermería. 2010;28(2):23-33.
Lazar A, Demiris G, Thompson HJ. Involving family members in the implementation and evaluation of technologies for dementia: a dyad case study. J. Gerontol. Nurs. 2015;41(4):21-6. http://doi.org/8zd.
Chaparro-Díaz L. Cómo se constituye el "vínculo especial" de cuidado entre la persona con enfermedad crónica y el cuidador familiar. Aquichan. 2011.11(1):7-22. http://doi.org/wk3.
López-Gil MJ, Orueta-Sánchez R, Gómez-Caro S, Sánchez-Oropesa A, Carmona-de la Morena J, Alonso-Moreno FJ. El rol de Cuidador de personas dependientes y sus repercusiones sobre su Calidad de Vida y su Salud. Rev. Clin. Med. Fam. 2009.2(7):332-9.
Lin F, Chaboyer W, Wallis M. A literature review of organizational, individual and teamwork factors contributing to the ICU discharge process. Aust. Crit. Care. 2009;22 (1):29-43. http://doi.org/bdd6kj.
Chen J, Ross JS, Carlson MD, Lin Z, Normand SL, Bernhein SM, et al. Skilled nursing facility referral and hospital readmission rates after heart failure or myocardial infarction. Am. J. Med. 2012;125(1):100-9. http://doi.org/fzxqfp.
Foust JB. Discharge planning as part of daily nursing practice. Appl. Nurs. Res. 2007;20(2):72-7. http://doi.org/dvbhf2.
Han CY, Barnard A, Chapman H. Discharge planning in the emergency department: a comprehensive approach. J. Emerg. Nurs. 2009;35 (6):525-7. http://doi.org/fm4bq5.
Collier EJ. Harrington C. Discharge planning, nursing home placement and the Internet. Nurs Outlook. 2005;53(2):95-103. http://doi.org/fpsvz6.
Pichitpornchaia W, Street A, Boontong T. Discharge planning and transitional care: issues in Thai nursing. Int. J. Nurs. Stud. 1999;36(5):355-62. http://doi.org/fmvh83.
Hanratty B, Holmes L, Lowson E, Grande G, Addington-hall J, Payne S, et al. Older adults' experiences of transitions between care settings at the end of life in england: a qualitative interview study. J. Pain Symptom Manage. 2012;44(1):74-83. http://doi.org/8zf.
Krohn DA. Discharge Instructions in the Outpatient Setting: Nursing Considerations. J Radiology Nursing. 2008;27(1):29-33. http://doi.org/8zg.
Adib-Hajbaghey M, Maghaminejad F, Abbasi A. The role of continuous care in reducing readmission for patients with heart failure. J. Caring Sci. 2013 Nov 30 2(4): 255-67. http://doi.org/87n.
Annells M, Koch T, Brown M. Client relevant care and quality of life: the trial of a Client Generated Index (CGI) tool for community nursing. Int. J. Nurs. Stud. 2001;38(1):9-16. http://doi.org/cx449q.
Kenner C, Boykova M. Transition to Home: Family Perspectives on Care in Russia. Newborn Infant Nurs. Rev. 2007;7(1):20-24. http://doi.org/cj2h3q.
Senarath U, Gunawardena NS. Development of an Instrument to Measure Patient Perception of the Quality of Nursing Care and Related Hospital Services at the National Hospital of Sri Lanka. Asian Nurs. Res. 2011;5(2):71-80. http://doi.org/d6vw3v.
Bobay KL, Jerofke TA, Weiss ME, Yakusheva O. Age-Related Differences in Perception of Quality of Discharge Teaching and Readiness for Hospital Discharge. Geriatr. Nurs. 2010.31(3):178-87. http://doi.org/bz32q4.
McMurray A, Johnson P, Wallis M, Patterson E, Griffiths S. General surgical patients' perspectives of the adequacy and appropriateness of discharge planning to facilitate health decision-making at home. J. Clin. Nurs. 2007;16(9):1602-9. http://doi.org/d9ccfz.
Hadjistavropoulos HD, Garratt S, Janzen JA, Bourgault-fagnou MD, Spice K. Development and evaluation of a Continuity of Care Checklist for improving orthopaedic patient discharge from hospital. Journal of Orthopaedic Nursing. 2009;13(4):183-93. http://doi.org/cqt6pq.
Hauser JM. Lost in Transition: The Ethics of the Palliative Care Handoff. J. Pain Symptom Manage. 2009;37(5):930-3. http://doi.org/b4pcj6.
Crocker JB, Crocker JT, Greenwald JL. Telephone Follow-up as a Primary Care Intervention for Postdischarge Outcomes Improvement: A Systematic Review. Am. J. Med. 2012;125(9):915-21. http://doi.org/8zj.
Jacob E. Making the Transition from Hospital to Home: caring for the Newly diagnosed child with cancer. Home Care Prov. 1999;4(2):67-73. http://doi.org/d6cp3m.
Baker EB, Wellman NS. Nutrition Concerns in Discharge Planning for Older Adults: A Need for Multidisciplinary Collaboration. J. Am. Diet. Assoc. 2005;105 (4):603-7. http://doi.org/bxh9zm.
Bull MJ, Hansen HE, Gross CR. A Professional-Patient Partnership Model of Discharge Planning with elders hospitalized with heart failure. Appl. Nurs. Res. 2000;13(1):19-28. http://doi.org/chhj9f.
Ben-Morderchai B, Herman A, Kerzman H, Irony A. Structured discharge education improves early outcome in orthopedic patients. Int. J. Orthop. Trauma Nurs. 2010;14(2):66-74. http://doi.org/d2b5rc.
Hiskett G. Clinical and economic consequences of discharge from hospital with on-going TNP therapy: a pilot study. J. Tissue Viability. 2010;19(1):16-21. http://doi.org/dtshg4.
Cómo citar
APA
ACM
ACS
ABNT
Chicago
Harvard
IEEE
MLA
Turabian
Vancouver
Descargar cita
CrossRef Cited-by
1. Sonia Carreño Moreno, Mauricio Arias Rojas. (2016). Competencia para cuidar en el hogar y sobrecarga en el cuidador del niño con cáncer. Gaceta Mexicana de Oncología, 15(6), p.336. https://doi.org/10.1016/j.gamo.2016.09.009.
2. Maria Stella Campos de Aldana, Erika Yurley Durán Niño, Silvia Liliana Ruiz-Roa, Astrid Nathalia Páez Esteban. (2023). Plan de egreso: herramienta del cuidado - diada con enfermedad crónica. Revista Cuidarte, 14(1) https://doi.org/10.15649/cuidarte.2754.
3. Daniela Díaz Agudelo, Olga Janneth Gómez Ramírez. (2019). Effect of the «Caring for caregivers®» program in family caregivers of people with rheumatoid arthritis. Revista Colombiana de Reumatología (English Edition), 26(3), p.177. https://doi.org/10.1016/j.rcreue.2019.07.001.
4. Yolima Judith Llorente Pérez, Jorge Luis Herrera Herrera, Edinson Oyola López, Ivonne Rosario Romero Guzmán, Xiomara España Franco Zuluaga. (2026). Self-Efficacy and Caregiving Competence in Family Caregivers of Patients Undergoing Renal Replacement Therapy: A Correlational Study. Nursing Reports, 16(2), p.73. https://doi.org/10.3390/nursrep16020073.
5. Claudia Patricia Cantillo-Medina, Brigitte Vanessa Castro-Morea, Yury Hasbleydi Mosquera. (2021). Estudio de la competencia para el autocuidado de las personas en tratamiento renal sustitutivo con diálisis. Enfermería Nefrológica, 24(4), p.398. https://doi.org/10.37551/S2254-28842021034.
6. Natalia Esquivel Garzón, Dora Inés Parra. (2025). Association between family caregiver competence and dependency in patients discharged from the Intensive Care Unit. Enfermería Intensiva (English ed.), 36(2), p.500540. https://doi.org/10.1016/j.enfie.2025.500540.
7. Elkin Herney Peñaranda-Pabón, Yury Alexandra Rico-Medina, Yoli Andreina Rozo-Hurtado, Olga Marina Vega-Angarita. (2018). Family caregivers: Competence in the care of the chronically ill. Revista Ciencia y Cuidado, 15(1), p.7. https://doi.org/10.22463/17949831.1227.
8. Luis Felipe Ruiz Valencia, Alisson Michelle Gordillo Sierra, Clara Rocío Galvis López. (2019). Factores condicionantes básicos en cuidadores informales de pacientes crónicos en el domicilio. Revista Cuidarte, 10(3) https://doi.org/10.15649/cuidarte.v10i3.608.
9. Lorena Alejandra Bernal-Baron, Olga Janneth Gómez-Ramírez. (2020). Competencia para el cuidado y acceso a la salud rural. Revista Ciencia y Cuidado, 17(3), p.46. https://doi.org/10.22463/17949831.2210.
10. Julia Elena Del Ángel-García, Rodrigo César León Hernández, Gregorio Méndez Santos, Isabel Peñarrieta de Córdoba, Florabel Flores-Barrios. (2020). Relación entre sobrecarga y competencias del cuidar en cuidadores informales de personas con enfermedades crónicas. MedUNAB, 23(2), p.233. https://doi.org/10.29375/01237047.3878.
11. Claudia Patricia Cantillo-Medina, Alix Yaneth Perdomo-Romero, Claudia Andrea Ramírez-Perdomo. (2021). Habilidad del cuidado, sobrecarga percibida y calidad de vida del cuidador de personas en diálisis. Enfermería Nefrológica, 24(2), p.184. https://doi.org/10.37551/S2254-28842021017.
12. Sonia patricia Carreño-Moreno, Lorena Chaparro-Díaz , Nelly Cáliz Romero , Nathaly Rivera Romero. (2022). Validez de la escala de soledad UCLA en cuidadores de pacientes crónicos en Colombia. Investigación en Enfermería: Imagen y Desarrollo, https://doi.org/10.11144/Javeriana.ie24.vesu.
13. Sonia Patricia Carreño Moreno, Maira Alejandra Fonsca Salguero, Juan Carlos Rojas Vargas, Paola Andrea Cubillos Moreno, Lina Juliana Moreno Ozuna. (2019). Concepto de sobrecarga del cuidador del niño con cáncer: revisión integrativa.. Revista Ciencia y Cuidado, 16(2), p.120. https://doi.org/10.22463/17949831.1605.
14. Dianne Sofia Gonzalez Escobar, Olga Marina Vega Angarita. (2021). Competencia para cuidar y Soporte social en cuidadores de Norte de Santander: Perspectiva comparativa. Revista Cuidarte, https://doi.org/10.15649/cuidarte.1329.
15. Lisieux E. De Borba Telles, Franklin Escobar Córdoba. (2015). Revista de la Facultad de Medicina y Ciência Latinoamericana. Revista de la Facultad de Medicina, 63(4), p.561. https://doi.org/10.15446/revfacmed.v63n4.54223.
16. Natalia Esquivel Garzón, Dora Inés Parra. (2025). Asociación entre competencia del cuidador familiar y dependencia en pacientes que egresan de Unidad de Cuidado Intensivo. Enfermería Intensiva, 36(2), p.500540. https://doi.org/10.1016/j.enfi.2025.500540.
17. Jenny Carolina Rojas Barbosa, Monica Paola Quemba Mesa. (2020). Díadas de cuidado y competencia para cuidar al alta hospitalaria en un hospital de Bogotá. Revista Investigación en Salud Universidad de Boyacá, 7(1), p.71. https://doi.org/10.24267/23897325.417.
18. Gloria Carrillo, Mónica Mesa, Olga Janeth Gómez, Oscar Numpaque, María Laguna. (2019). Educational intervention (CUIDAR) in cancer patients treated with surgery: A quasi-experimental study. Patient Education and Counseling, 102(8), p.1475. https://doi.org/10.1016/j.pec.2019.03.002.
19. Amparo Montalvo Prieto, Hanier Fajardo Rocha. (2019). Competencias del cuidador familiar para cuidar a su familiar que recibe quimioterapia.. Revista Ciencia y Cuidado, 16(2), p.95. https://doi.org/10.22463/17949831.1612.
20. Laura Milena Sánchez, Gloria Mabel Car. (1970). Competencia para el cuidado en el hogar diada persona con cáncer en quimioterapia. Cuidador familiar. Psicooncología, 14(1), p.137. https://doi.org/10.5209/PSIC.55817.
21. Daniela Díaz Agudelo, Olga Janneth Gómez Ramírez. (2019). Efecto del programa «Cuidando a los cuidadores®» en cuidadores familiares de personas con artritis reumatoide. Revista Colombiana de Reumatología, 26(3), p.177. https://doi.org/10.1016/j.rcreu.2019.07.003.
Dimensions
PlumX
Visitas a la página del resumen del artículo
Descargas
Licencia
Derechos de autor 2015 Revista de la Facultad de Medicina

Esta obra está bajo una licencia Creative Commons Reconocimiento 3.0 Unported.
-


















