


Publicado
Nutritional condition and IGF-1 and IGFBP-2 serum concentrations in students aged 7 to 9 attending two educational institutions
Estado nutricional y niveles séricos de IGF-1 e IGFBP-2 en escolares de 7 a 9 años en dos instituciones educativas
DOI:
https://doi.org/10.15446/revfacmed.v64n3.54454Palabras clave:
Insulin-Like Growth Factor I, School, Children, Nutritional Status, Insulin-Like Growth Factor Binding Protein 2, Adiposity (en)Factor I del crecimiento similar a la insulina, Niños, Estado nutricional, Proteína 2 de unión a factor de crecimiento similar a la Insulina, Adiposidad (es)
Descargas
Introduction: Nutritional vulnerability is more evident during childhood, since malnutrition has an impact on academic performance and is linked to different diseases during this period. Likewise, an increase in the incidence and prevalence of obesity in children has been observed, therefore, researches that assess nutritional conditions of children attending schools may have high-impact results in terms of public health.
Objective: To relate children’s nutritional condition by using anthropometry, with serum concentrations of insulin-like growth factor 1 (IGF-1) and its binding protein 2 (IGFBP-2).
Materials and methods: A cross-sectional observational and comparative study was performed in children aged 7 to 9 attending two schools, one from the public sector and the other from the private sector. An anthropometric assessment was performed in 157 children, while IGF-1 and IGFBP (enzyme immunoassay) serum concentrations were measured in 81 children. Pearson’s coefficient, analysis of variance (ANOVA), Dunnet’s test and Games Howell’s test, with a 95% confidence interval and a p<0.05 statistical significance, were considered for performing the statistical analysis.
Results: Overweight and obesity were found in 46 subjects; the prevalence of obesity was higher in boys, while overweight prevalence was higher in girls. A direct relation between IGF-1 and height (p<0,05) was observed, while an inverse relation between IGFBP-2 and BMI (p<0,001) was found.
Conclusions: IGF-1 serum concentrations were higher in students attending the public school.
Introducción. Una de las etapas con mayor vulnerabilidad del estado nutricional es la infancia, pues en este periodo la desnutrición interfiere con el desempeño escolar y se asocia a enfermedades; asimismo, se ha observado aumento de la incidencia y prevalencia de obesidad en niños, por lo que investigaciones de evaluación nutricional en población escolar pueden tener alto impacto en salud pública.
Objetivo. Relacionar el estado nutricional —antropometría— con niveles séricos del factor de crecimiento similares a la insulina 1 (IGF-1) y su proteína enlazante 2 (IGFBP-2).
Materiales y métodos. Estudio observacional de corte transversal comparativo entre estudiantes de 7 a 9 años de dos colegios, uno público y otro privado, mediante el cual se realizó valoración antropométrica de 157 niños y medición de niveles séricos de IGF-1 e IGFBP-2 (enzimoinmunoanálisis) en 81 niños. Para el análisis estadístico se tuvo en cuenta coeficiente de Pearson, análisis de varianza (ANOVA), test de Dunnet y Games Howell, intervalo de confianza del 95% y significancia estadística de p<0.05.
Resultados. Se registró sobrepeso y obesidad en 46 sujetos; la obesidad fue más prevalente en niños mientras que el sobrepeso en niñas. Se encontró relación directa entre IGF-1 y talla (p<0.05) y relación inversa entre IGFBP-2 e IMC (p<0.001).
Conclusiones. Las concentraciones séricas de IGF-1 fueron mayores en la institución pública.
original research
DOI: https://doi.org/10.15446/revfacmed.v64n3.54454
Nutritional condition and IGF-1 and IGFBP-2 serum concentrations in students aged 7 to 9 attending two educational institutions
Estado nutricional y niveles séricos de IGF-1 e IGFBP-2 en escolares
de 7 a 9 años en dos instituciones educativas
Received: 30/11/2015. Accepted: 17/03/2016.
Jenifer Tatiana Figueroa1 • Sorany Vera1 • Luz Helena Aranzález1 • Ismena Mockus1
1 Universidad Nacional de Colombia - Bogotá Campus - School of Medicine - Lipids and Diabetes Division - Bogotá, D.C. - Colombia.
Corresponding author: Jenifer Tatiana Figueroa. Department of Physiological Sciences, School of Medicine, Universidad Nacional de Colombia. Carrera 30 No. 45-03, building 471, office 418. Phone number: +57 1 3165000, ext.: 15054; mobile phone: +57 3133733488. Bogotá, D.C. Colombia. Email: jtfigueroah@unal.edu.co.
| Abstract |
Introduction: Nutritional vulnerability is more evident during childhood, since malnutrition has an impact on academic performance and is linked to different diseases during this period. Likewise, an increase in the incidence and prevalence of obesity in children has been observed, therefore, researches that assess nutritional conditions of children attending schools may have high-impact results in terms of public health.
Objective: To relate children’s nutritional condition by using anthropometry, with serum concentrations of insulin-like growth factor 1 (IGF-1) and its binding protein 2 (IGFBP-2).
Materials and methods: A cross-sectional observational and comparative study was performed in children aged 7 to 9 attending two schools, one from the public sector and the other from the private sector. An anthropometric assessment was performed in 157 children, while IGF-1 and IGFBP (enzyme immunoassay) serum concentrations were measured in 81 children. Pearson’s coefficient, analysis of variance (ANOVA), Dunnet’s test and Games Howell’s test, with a 95% confidence interval and a p<0.05 statistical significance, were considered for performing the statistical analysis.
Results: Overweight and obesity were found in 46 subjects; the prevalence of obesity was higher in boys, while overweight prevalence was higher in girls. A direct relation between IGF-1 and height (p<0,05) was observed, while an inverse relation between IGFBP-2 and BMI (p<0,001) was found.
Conclusions: IGF-1 serum concentrations were higher in students attending the public school.
Keywords: Insulin-Like Growth Factor I; School; Children; Nutritional Status; Insulin-Like Growth Factor Binding Protein 2; Adiposity (MeSH).
Figueroa JT, Vera S, Aranzález LH, Mockus I. Nutritional condition and IGF-1 and IGFBP-2 serum concentrations in students aged 7 to 9 attending two educational institutions. Rev. Fac. Med. 2016;64(3):439-45. English. doi: https://doi.org/10.15446/revfacmed.v64n3.54454.
| Resumen |
Introducción. Una de las etapas con mayor vulnerabilidad del estado nutricional es la infancia, pues en este periodo la desnutrición interfiere con el desempeño escolar y se asocia a enfermedades; asimismo, se ha observado aumento de la incidencia y prevalencia de obesidad en niños, por lo que investigaciones de evaluación nutricional en población escolar pueden tener alto impacto en salud pública.
Objetivo. Relacionar el estado nutricional —antropometría— con niveles séricos del factor de crecimiento similares a la insulina 1 (IGF-1) y su proteína enlazante 2 (IGFBP-2).
Materiales y métodos. Estudio observacional de corte transversal comparativo entre estudiantes de 7 a 9 años de dos colegios, uno público y otro privado, mediante el cual se realizó valoración antropométrica de 157 niños y medición de niveles séricos de IGF-1 e IGFBP-2 (enzimoinmunoanálisis) en 81 niños. Para el análisis estadístico se tuvo en cuenta coeficiente de Pearson, análisis de varianza (ANOVA), test de Dunnet y Games Howell, intervalo de confianza del 95% y significancia estadística de p<0.05.
Resultados. Se registró sobrepeso y obesidad en 46 sujetos; la obesidad fue más prevalente en niños mientras que el sobrepeso en niñas. Se encontró relación directa entre IGF-1 y talla (p<0.05) y relación inversa entre IGFBP-2 e IMC (p<0.001).
Conclusiones. Las concentraciones séricas de IGF-1 fueron mayores en la institución pública.
Palabras clave: Factor I del crecimiento similar a la insulina; Niños; Estado nutricional; Proteína 2 de unión a factor de crecimiento similar a la Insulina; Adiposidad (DeCS).
Figueroa JT, Vera S, Aranzález LH, Mockus I. [Estado nutricional y niveles séricos de IGF-1 e IGFBP-2 en escolares de 7 a 9 años en dos instituciones educativas]. Rev. Fac. Med. 2016;64(3):439-45. English. doi:
https://doi.org/10.15446/revfacmed.v64n3.54454.
Introduction
Nutrition is key for growth and human development and may be affected by economic, cultural, social, and physiological factors, among others (1,2). Nutritional vulnerability is more evident during childhood, since the onset of malnutrition during this period is associated with capacity and learning constraints and interferes with an adequate school performance. The effects of malnutrition on health and education have effects on economic and human capital costs that must be assumed by the society (2). Similarly, malnutrition by excess has become a public health problem in recent years.
In Colombia, a high prevalence of malnutrition caused by both deficiency (acute and chronic) and excess (obesity and overweight) is evident. According to the results of the National Survey on Nutrition and Food 2010 (ENSIN, by its acronym in Spanish) (3), a prevalence of low height for age of 12.6% and low weight for height of 1.1% was obtained, as well as a prevalence of overweight of 13.7% and obesity of 5.2% in the group of children aged 5 to 9. These findings can affect growth and development in this stage of life, determining the incidence of new diseases and affecting economic development.
Type 1 insulin-like growth factor (IGF-1) is a polypeptide anabolic hormone secreted in multiple tissues, whose serum concentrations come mainly from the liver (4,5); its synthesis is regulated by the growth hormone (GH) (5) and by other factors, including nutrition, which plays an important role (6,7). IGF-1 has multiple functions related to metabolic and growth processes and is responsible for certain actions of GH (5). It has also been observed that IGF-1 exerts insulin-like activities and that concentrations of this hormone are regulated by the interaction with its binding proteins (IGFBPs), for which six types have been described (4,7): IGFBP-1, IGFBP-2 and IGFBP-3 are predominant in blood (5).
Recent studies suggest that IGFBP2 is involved in alterations associated with obesity (8-10). As this is the main IGFBP expressed during childhood and is also the most produced by adipocytes, its determination is of great interest to study the relation between nutrition, growth and metabolism.
In this sense, this paper projects the evaluation of the relations between anthropometric variables, and energy and nutrient intake with IGF-1 and IGFBP-2 serum concentrations in children from two educational institutions, one public and another private.
Materials and methods
A cross-sectional comparative observational study was conducted in students aged 7 to 9 from one private and one public school, where anthropometric and food consumption variables were compared with IGF-1 and IGFBP-2 serum levels.
This study was conducted in two schools that receive mainly children from families of socioeconomic strata 1 and 2:
1. Llano Oriental School, a public school located in the locality of Bosa in Bogotá, D.C., which receives 1184 students distributed in morning and afternoon school hours; during the morning, preschool and elementary school children are attended and during the afternoon middle and high school students. Students receive daily school snacks provided by the Department of Education of the District, which are consumed in the classroom at the beginning of their break.
2. Liceo Integral Los Alisos, a private school located in the municipality of Soacha, Cundinamarca, which provides elementary, middle and high school education to 418 students in one school day. Children have a break during which they can consume food in the playground.
The selection criteria were: age between 7 and 9, no pubertal development initiation, enrollment in the selected educational institutions, informed consent reviewed and signed by parents or legal guardians and the children, no drug consumption in the last month and absence of diseases such as diabetes, hypoglycemia and growth hormone deficiency that could affect the results.
For anthropometric data, the World Health Organization (WHO), which describes the standardized technique for measuring height, weight and waist circumference was considered. A Tanita electronic scale was used to measure weight —the subjects were measured in light clothes and barefoot— and for measuring height, a stadiometer (SECA) was used. Based on these data, the body mass index (BMI) kg/m2 was calculated. The waist circumference (WC) was measured in the horizontal plane, at the midpoint between the last right rib and the iliac crest using an inelastic tape fiber glass. These data were taken by two nutritionists and a nursing assistant.
During the initial phase, the universe consisted of all students from 7 to 9 years old enrolled in the two educational institutions during the second half of 2014, which accounted for 372 children —142 subjects from Liceo Integral Los Alisos and 230 from Llano Oriental School—; only 185 of these children met the selection criteria. Seven children did not provide a blood sample nor attended anthropometric assessments. This way, a total of 178 children were studied, but due to the time elapsed since the signing of consent and data collection, 21 children turned 10 years and were not included in the statistical analysis. Thus, the target population was composed of 157 subjects (70 boys and 87 girls).
The information obtained in the nutritional assessment of children was interpreted using the growth curves established by the WHO for children and adolescents (11). According to the indicators weight/height, height/age and WC/age, five subgroups were formed: 1) low size and risk of low size; 2) eutrophic; 3) appropriate weight with high WC; 4) overweight and 5) obesity. WC in children was classified according to percentiles of the Center for Disease Control and Prevention and the National Center for Health Statistics (12).
The anthropometric study was conducted on a sample of 157 subjects, whereas hormonal measurements were performed on a subsample of 81 children. In order to keep statistical balance, a subsample size was established taking into account the 18 children with obesity for the analysis of IGF-1 and IGFBP-2. All children were Tanner stage 1 without clinical manifestation of sexual development.
Blood samples were collected from the antecubital vein after 12 hours of fasting, centrifuged at 3500rpm for five minutes and the obtained serum was stored at -80°C. IGF-1 and IGBP-2 serum levels were determined by double junction enzyme-linked immunosorbent assay (ELISA) using KAP1581 kits for IGF-1 and KAPME05 for IGFBP-2 and according to the manufacturer’s protocols. This process was performed with DS2/DSX automated equipment.
In addition, a written survey about the nutritional background, with a frequency table of food consumption —for which parents provided information on dietary intake of students for specific food groups, especially proteins— and family history was conducted.
Data were stored in Microsoft Excel program and SPSS version 18.0 was used for statistical analysis. The first part consisted of a descriptive analysis of weight, height, BMI, WC, IGF-1 and IGFBP-2, and several statistics tools were used as measures of central tendency (mean, average), form (histograms), position (percentiles, and box diagrams), and dispersion (varianza, central deviation), which allowed an overview of the relation between variables.
At a later stage, the relation between variables was determined in order to assess the possible association between nutritional status, IGF-1 and IGFBP-2. Inferences and hypotheses evaluations were conducted through the Pearson coefficient, Chi square, analysis of variance (ANOVA), Kruskal Wallis, and Dunnet and Games-Howell. For comparison of groups and association between nutritional status, IGF-1 and IGFBP-2, a technical analysis of variance (ANOVA) was used when data was (parametrically) normal and homogeneous; after observing significant results, an analysis of multiple comparisons with different means using Dunnet method was performed to recognize the relevant differences.
The Games-Howell test was used for pairwise comparison and for evaluating IGF-1 serum levels based on food consumption. Scatter plots of the IGF-1 values were performed for each of the food groups. The relationship between variables was identified to test the hypothesis of equality of means between each class; associations were calculated with p<0.05 as statistically significant with confidence interval of 95%. The numerical variables were expressed as mean, standard deviation and percentages.
This research was approved by the Ethics Committee of the Faculty of Medicine from Universidad Nacional de Colombia, it considered all ethical aspects under Resolution 8430 of 1993 by the Ministry of Health of Colombia and was classified as minimum risk for health participants; the information provided to children met the requirements of article 15 of the aforementioned resolution. In addition, each participant provided informed consent signed by parents or legal guardians.
Results
Table 1 shows the statistical information of the anthropometric variables weight, height, WC and BMI of the study population (n=157).
Table 1. Anthropometric variables of the study subjects.
|
Statistical |
Weight (Kg) |
Height (cm) |
WC (cm) |
BMI Weight (kg)/height (m)2 |
|
Average |
29.8 |
128.6 |
62.4 |
17.9 |
|
Standard deviation |
6.8 |
6.9 |
8.4 |
2.8 |
|
Minimum |
19.5 |
111.8 |
48.8 |
13.2 |
|
25th percentile |
24.6 |
123.3 |
56.2 |
15.9 |
|
75th percentile |
33.3 |
134.7 |
67.0 |
19.6 |
|
Maximum |
50.6 |
144.0 |
85.7 |
27.1 |
WC: waist circumference; BMI: body mass index. Source: Own elaboration based on the data obtained in the study.
The analysis of the nutritional status of the participants was based on body mass index (BMI/age) and was classified into eutrophic, overweight, obesity, thinness and thinness risk (Figure 1). Children were classified according to height/age into appropriate, risk of low height and low height (Figure 2), finding the coexistence of malnutrition by excess and deficit. Thinness was evidenced only in girls of the private institution and there was a delay in height in girls from both institutions, as well as a significant percentage of overweight boys and girls in both institutions, predominantly obese boys and overweight girls (Figure 1).
Those with the highest WC average (65.1±3.6cm and 73.4±8.1cm, respectively) were ranked in the overweight and obesity nutritional groups. Children with high WC and proper weight presented WC 63.3±3.5, whereas the eutrophic and low height risk group showed WC 56.0±1.4cm and 54.7±3.8cm, respectively. An analysis of the results of IGF-1 and IGFBP-2 serum levels measured in the subgroup of 81 children are presented below.

Figure 1. Nutritional status according to BMI/age. Source: Own elaboration based on the data obtained in the study.
The relationship between IGF-1 and nutritional status can be seen in Figure 3, where a strong association between IGF-1, BMI and CC is evident; however, a relation between IGF-1 and height is suggested. Also the inverse relation between IGFBP-2 serum levels and BMI is identified.
Figure 4 displays the box plots that show the position of the data, where the lowest levels of IGF-1 are found in children with height delay. Dunnet test confirms the significant difference between the groups delay in height and proper height.
Higher levels of IGF-1 were mainly seen in overweight children from Llano Oriental School (Figure 5). To clarify the possible relation between obesity and IGF-1, serum levels of IGF-1 in obese subjects were compared with eutrophic children (controls) and a significant difference (p=0.035) was observed, indicating that the adiposity level is related to IGF-1 serum levels.

Figure 2. Nutritional status according to height/age. Source: Own elaboration based on the data obtained in the study.
Table 2. Statistical summary of IGF-1 and IGFBP-2 concentrations.
|
(ng/ml) |
(ng/ml) |
|
|
Average |
300.93 |
230.19 |
|
Standard deviation |
150.23 |
83.70 |
|
Count |
81 |
81 |
|
Minimum |
65.42 |
21.92 |
|
Maximum |
734.62 |
442.09 |
|
25th percentile |
195.74 |
170.75 |
|
Median |
245.26 |
221.74 |
|
75th percentile |
385.61 |
288.04 |
Source: Own elaboration based on the data obtained in the study.

Figure 3. Scattering matrix between anthropometric and hormonal variables. IGF-1: type 1 insulin-like growth factor; IGFBP-2 binding protein of type 2 IGF-1; BMI: body mass index; WC: waist circumference. Source: Own elaboration based on the data obtained in the study.

Figure 4. Box plots of IGF-1 serum levels according to height/age. Source: Own elaboration based on the data obtained in the study.

Figure 5. Box plot for circulating levels of IGF-1 according to weight/height and CC/age per institution. IGF-1: type 1 insulin-like growth factor; WC: waist circumference. Source: Own elaboration based on the data obtained in the study.
Figure 6 compares the relative frequency histograms of IGF-1 for both educational institutions; there is a positive asymmetry observed in both cases. While lower concentrations of IGF-1 are present in the students of Liceo Integral Los Alisos, the highest values of this variable were found in Llano Oriental School.
Different p values are shown in Table 3 to compare the mean, median and distribution groups —classified according to BMI/age and height/age—.

Figure 6. Frequency histograms of IGF-1 per educational institutions.IGF-1: type 1 insulin-like growth factor.Source: Own elaboration based on the data obtained in the study.
Table 3. Comparison of height and IGF-1, IGFBP-2 and BMI p value.
|
Category |
ANOVA p value |
Median p value |
P value (Kruskal-distribution) |
|
IGF-1/height |
0.097 |
0* |
0.024* |
|
IGFBP-2/BMI |
0* |
0.234 |
0.129 |
ANOVA: variance analysis; IGF-1: type 1 insulin-like growth factor; IGFBP-2 type 2 binding protein of IGF-1. * Significance level p<0.05.
Source: Own elaboration based on the data obtained in the study.
Figure 7 shows a diagram of boxes indicating the position of IGFBP-2 serum levels in relation with BMI classification; also, it is observed that children with lower IGBP-2 values are those with obese and overweight. The greatest statistical significance is observed in the obese group after using Dunnet test.
To study the relation between intake of macronutrients —proteins, lipids and carbohydrates— and IGF-1 serum levels, a descriptive analysis was performed between the means of this hormone and the count of the most frequent categories of consumption of food groups.
In this research, only one possible link to the source of protein food was found in children who consumed milk and dairy products daily and those who ate eggs 2 to 3 times a week, who showed the highest IGF-1 values. Within other food groups, it became clear that occasional use of additions of fat was associated with lower levels of IGF-1.
It is important to note that the high weekly consumption of fast foods, soda, fat additions and processed food, accompanied by a low consumption of vegetables and fruits, indicates inadequate eating habits in this group of children and could explain the high levels of overweight and obesity found.

Figure 7. Box plot IGFBP-2 and BMI. IGFBP-2: type 2 binding protein of IGF-1. Source: Own elaboration based on the data obtained in the study.
Discussion
Malnutrition due to both excess and deficit was found: in 0.6% of children thinness was observed and in 3.2% delay in height, which is inferior to the data reported by the ENSIN 2010 (3) —thinness 2.1% and delay in height 10%—. Low height risk and low height were observed only in girls, and the only case of thinness was found in a girl from Liceo Integral Los Alisos.
This study shows a higher prevalence of overweight (19.1%) and obesity (10.2%) compared to national data reported by ENSIN 2010 (13.4% and 4.1%, respectively) (3).When analyzing the results by sex, obesity is more prevalent in boys, while overweight is more common in girls. These findings can be compared with those reported in previous Colombian studies conducted in Bogotá (13) and Medellín (14), where similar data were presented and the coexistence of malnutrition, overweight and obesity was evident. In Latin America, other studies have also reported similar results in school children from Ecuador (15) and Perú (16).
Malnutrition during childhood caused by deficit can affect intellectual and cognitive ability by reducing school performance and learning life skills. Therefore, this condition impairs human and professional development and affects the progress of the community and the country (2,17). Also, excess weight has important consequences since it is associated with metabolic disorders (dyslipidemias, insulin resistance, diabetes, hypertension, among others) (18) that may occur at an early age; in addition, an obese child may suffer social discrimination, low self-esteem and depression (19). Similarly, overweight during childhood and adolescence has been associated with higher probabilities of eating disorders such as anorexia and bulimia (18).
When analyzing the nutritional status and IGF-1, a proportional relation between circulating levels of this hormone with height was observed. Low IGF-1 levels were also found in children with delay in height, which agrees with previous studies (20-22). These results are explained by the interaction of the GH-IGF-1 hormonal axis.
It has been shown that malnutrition is associated with a state of GH resistance (23), which would explain the low functionality of this hormone to regulate the synthesis and availability of IGF-1 in subjects with chronic malnutrition or stunting. In turn, a positive relation between IGF-1 levels and BMI was found, relation that has not been observed in all studies when recording normal (24), low (25,26) and high values (26,27). These differences may occur since this growth factor is affected by sex, age, degree of obesity and genetic factors, which generates conflicting results. It is important to note that most studies have been conducted in adults and there is little research with school population linking obesity with circulating levels of IGF-1.
It is necessary to clarify the relation between IGF-1 and diet. This study did not find a clear influence of the intake of protein sources, but a relation (although small) between a consumption of dairy and eggs with IGF-1 concentrations was found. Previous studies in rats show that the decrease in energy intake and marked protein deprivation decrease levels of IGF-I (28,29). Most human studies have been conducted in adults (30-32), so data are still scarce in school children. A multiethnic study of populations living in the US found no association between IGF-1 and protein consumption (33), like other studies in adults (34).
When comparing the levels of IGF-1 per educational institution, it was found that they were higher in the public institution, which may be attributed to increased access and availability of food and nutrients, since these subjects received school snacks from the district daily, as opposed to the private school children, who eat what their parents send from home or buy packaged foods with high sugar content in the school store. It is noteworthy that the highest prevalence of obesity was observed in Llano Oriental School.
In this research an inversely proportional relation between IGFBP-2 and nutritional status was also found: the lowest values of this binding protein were found in children diagnosed with obesity, which is consistent with several previous studies (8,10,35). IGFBP-2 is the major IGFBP secreted by white preadipocytes during adipogenesis (8,9). The correlation found between decreased circulating IGFBP-2 and BMI could be related to a profile of unfavorable secretion of adipocytes of the binding protein and, simultaneously, with increased leptin and decreased adiponectin (34). Leptin has significant effects on maintaining normal weight and glucose metabolism and has been proven to increase hepatic transcription of IGFBP-2 when administered by peripheral or central route in mice with lipodystrophy (36-38). Regarding obesity, a possible leptin resistance has been reported, which could explain the low serum levels of IGBP-2 observed in this study (37,38); however, the mechanisms by which leptin regulates the production of IGFBP-2 have not been fully elucidated.
On the other hand, the analysis of food consumption showed inadequate eating habits in both, boys and girls, consisting of low consumption of fruits and vegetables, which violates the recommendations of five daily servings by the WHO. In addition, a high intake of high caloric density foods such as soft drinks, fast foods, fat additions and packaged food was found, highlighting the importance of working in food and nutrition education with families, students, school stores and staff.
In this study a high prevalence of overweight and obesity in the two educational institutions, whose socioeconomic strata is low, was observed, which is why greater attention should be paid to the promotion of healthy lifestyles, including changing eating habits, self-care practices and promotion of physical activity in the school population to reduce the risk of developing chronic conditions such as cardiovascular disease, diabetes and cancer that could permanently influence their quality of life.
Conclusions
In the educational institutions studied in this work, a coexistence of malnutrition caused by deficit and excess weight was observed, as well as low prevalence of thinness and risk of thinness and high prevalence of overweight and obesity. Obesity was more prevalent in boys and overweight in girls, while poor eating habits given by low consumption of fruits and vegetables and high intake of caloric foods were evident.
A direct relation between IGF-1 and height and between IGF-1 levels and BMI was found. Since an inverse relation between IGFBP-2 and BMI was observed, this may suggest that IGFBP-2 is a predictor of adiposity in children; however, it was no possible to establish a direct relation of IGF-1 with protein consumption, except for dairy and egg.
This work can be a baseline that evidence more fully the current situation of the school population by relating not only anthropometric variables but also including hormone variables.
This paper is the result of the thesis for the Master’s degree in Physiology of one of the authors, entitled “The relation between nutritional status, serum levels of insulin-like factor growth (IGF-1) growth and its type 2 binding protein (IGFBP -2) in school children from two educational institutions in Bogotá and Soacha (2014)” (39).
Conflict of interests
None stated by the authors.
Funding
This research was funded by the Master’s program in Physiology and the Universidad Nacional DIB-Hermes-21971 call.
Acknowledgements
To both educational institutions, Llano Oriental School and Liceo Integral Los Alisos, and their staff, which arranged the facilities, personnel and time. To the Master’s program in Physiology and to the Laboratory of Lipids and Diabetes.
References
1.Latham MC. Nutrición Humana en el Mundo en Desarrollo. Roma: Organización para la Agricultura y la Alimentación; 2002 [cited 2016 Aug 26]. Available from: http://goo.gl/vHabFr.
2.Mcdonald B, Haddad L, Gross R, McLachlan M. Nutrición: Los argumentos a Favor. In: Comité permanente de nutrición del sistema de las Naciones Unidas, editor. Nutrición: La base para el desarrollo. Ginebra: Organización de las Naciones unidas; 2002 [cited 2016 Aug 25]. Available from: http://goo.gl/CgcuWf.
3.Fonseca-Centeno Z, Heredia-Vargas AP, Ocampo-Téllez R, Forero-Torres Y, Sarmiento-Dueñas OL, Álvarez-Uribe MC, et al. Encuesta Nacional de la Situación Nutricional en Colombia 2010 - ENSIN. Bogotá, D.C.: Instituto Colombiano de Bienestar Familiar; 2011.
4.Bonefeld K, Møller S. Insulin-like growth factor-I and the liver. Liver Int. 2011;31(7):911-9. http://doi.org/cdspbw.
5.Puche JE, Castilla-Córtazar I. Human conditions of insulin-like factor-I (IGF-1) deficiency. J. Transl. Med. 2012;10:224-53. http://doi.org/bp24.
6.Fontana L, Weiss EP, Villareal DT, Klein S, Holloszy JO. Long-term effects of calorie or protein restriction on serum IGF-1 and IGFBP-3 concentration in humans. Aging Cell. 2008;7(5):681-7. http://doi.org/cm44hc.
7.Holly J, Perks C. The Role of Insulin-Like Growth Factor Binding Proteins. Neuroendocrinology. 2006;83(3-4):154-60. http://doi.org/frw3nt.
8.Ko JM, Park HK, Yang S, Kim EY, Chung SC, Hwang IT. Association between insulin-like growth factor binding protein-2 levels and cardiovascular risk factors in Korean children. Endocr. J. 2012;59(4):335-43. http://doi.org/fzfztp.
9.Wheatcroft SB, Kearney MT, Shah AM, Ezzat VA, Miell JR, Modo M, et al. IGF-Binding Protein-2 Protects Against the Development of Obesity and Insulin Resistance. Diabetes. 2007;56(2):285-94.
http://doi.org/b936mv.
10.Heald AH, Kaushal K, Siddals KW, Rudenski AS, Anderson SG, Gibson JM. Insulin-like growth factor binding protein-2 (IGFBP-2) is a marker for the metabolic syndrome. Exp. Clin. Endocrinol. Diabetes. 2006;114(7):371-6. http://doi.org/cxkdxv.
11. Ministerio de la Protección Social, Instituto Nacional de Salud, Instituto Colombiano de Bienestar Familiar. Instructivo para la Implementación de los Patrones de Crecimiento de la OMS en Colombia para niños, niñas y adolescentes de 0 a 18 años. Bogotá, D.C.: Instituto Nacional de Salud; 2010.
12.McDowell MA, Fryar CD, Ogden CL. Anthropometric Reference Data for Children and Adults: United States 1988-1994. Washington, D.C.: National Center for Health Stadistics. Vital and Health Statistics 11 (249); 2009 [cited 2016 Aug 19]. Available from: http://goo.gl/elph8S.
13. Fajardo-Bonilla E, Ángel-Arango LA. Prevalencia de sobrepeso y obesidad, consumo de alimentos y patrón de actividad física en una población de niños escolares de la Ciudad de Bogotá. Rev Med. 2012;20(1):101-16.
14.Uscátegui-Peñuela RM, Álvarez-Uribe MC, Laguado-Salinas I, Soler-Terranova W, Martínez-Maluedas L, Arias-Arteaga R, et al. Factores de riesgo cardiovascular en niños de 6 a 18 años de Medellín (Colombia). An. Pediatr. 2003;58(5):411-7. http://doi.org/ck5b4w.
15.Yepez R, Carrasco F, Baldeón ME. Prevalencia de sobrepeso y obesidad en estudiantes adolescentes ecuatorianos del área urbana. Arch. Latinoam. Nutr. 2008;58(2):139-43.
16.Bustamante A, Seabra AF, Garganta RM, Maia JA. Efectos de la actividad física y del nivel socioeconómico en el sobrepeso y obesidad de escolares, Lima Este 2005. Rev. Perú. Med. Exp. Salud Pública. 2007;24(2):121-8.
17.Wisbaum W. La desnutrición infantil. Causas, consecuencias y estrategias para su prevención y tratamiento. Madrid: Unicef; 2011 [cited 2016 Aug 29] Available from: http://goo.gl/WeytGM.
18.Reyna L. Consecuencias de la obesidad en el niño y el adolescente: un problema que requiere atención. Rev. Peru Med. Exp. Salud Pública. 2012;29(3):357-60. http://doi.org/bp25.
19. Lobstein T, Baur L, Uauy R. Obesity in children and young people: a crisis in public health. Obes. Rev. 2004;5(Suppl 1):4-85. http://doi.org/ff3b4n.
20. Soliman AT, Elawwa A, Khella A, Saeed S, Yassin H. Linear growth in relation to the circulating concentration of insulin-like growth factor-I in young children with acyanotic congenital heart disease with left to right shunts before versus after surgical intervention. Indian J. Endocrinol. Metab. 2012;16(5):791-5. http://doi.org/bp26.
21.Wang J, Zhou J, Bondy CA. IGF-1 promotes longitudinal bone growth by insulin-like actions augmenting chondrocyte hypertrophy. FASEB J. 1999;13(14):1985-90.
22.Ranke MB, Schweizer R, Elmlinger MW, Weber K, Binder G, Schwarze CP, Wollmann HA. Significance of basal IGF-I, IGFBP-3 and IGFBP-2 measurements in the diagnostics of short stature in children. Horm. Res. 2000;54(2):60-8. http://doi.org/fhtmp4.
23.Turan S, Bereket A, Furman A, Omar A, Berber M, Ozen A, et al. The effect of economic status on height, insulin-like growth factor (IGF)-I and IGF binding protein-3 concentrations in healthy Turkish children. Eur. J. Clin. Nutr. 2007;61(6):752-8. http://doi.org/c7pkbq.
24.Nam SY, Lee EJ, Kim KR, Cha BS, Song YD, Lim SK, et al. Effect of obesity on total and free insulin-like growth factor (IGF)-1, and their relationship to IGF-binding protein (BP)-1, IGFBP-2, IGFBP-3, insulin, and growth hormone. Int. J. Obes. Relat. Metab. Disord. 1997;21(5):355-9. http://doi.org/dj67c4.
25. Mårin P, Kvist H, Lindstedt G, Sjöström L, Björntorp P. Low concentrations of insulin-like growth factor-I in abdominal obesity. Int. J. Obes. Relat. Metab. Disord. 1993;17(2):83-9.
26.Kong AP, Choi KC, Wong GW, Ko GT, Ho CS, Chan MH, et al. Serum concentrations of insulin-like growth factor-I, insulin-like growth factor binding protein-3 and cardiovascular risk factors in adolescents. Ann. Clin. Biochem. 2011;48(3):263-9. http://doi.org/dcrvb3.
27.Lewitt MS, Dent MS, Hall K. The Insulin-Like Growth Factor System in Obesity, Insulin Resistance and Type 2 Diabetes Mellitus. J. Clin. Med. 2014;3(4):1561-74. http://doi.org/bp33.
28.Sánchez-Gómez M, Malmlöf K, Mejía W, Bermúdez A, Ochoa MT, Carrasco-Rodríguez S, et al. Insulin-like growth factor-I, but not growth hormone, is dependent on a high protein intake to increase nitrogen balance in the rat. Br. J. Nutr. 1999;81(2):145-52.
29.Norat T, Dossus L, Rinaldi S, Overvad K, Grønbaek H, Tjønneland A, et al. Diet, serum insulin-like growth factor-I and IGF-binding protein-3 in European women. Eur. J. Clin. Nutr. 2007;61(1):91-8. http://doi.org/bkwwbk.
30.VandeHaar MJ, Moats-Staats BM, Davenport ML, Walker JL, Ketelslegers JM, Sharma BK, et al. Reduced serum concentrations of insulin-like growth factor-I (IGF-I) in protein-restricted growing rats is accompanied by reduced IGF-I mRNA levels in liver and skeletal muscle. J. Endocrinol. 1991;130(2):305-12. http://doi.org/db2hnj.
31. Hoppe C, Mølgaard C, Juul A, Michaelsen KF. High intakes of skimmed milk, but not meat, increase serum IGF-I and IGFBP-3 in eight-year-old boys. Eur. J. Clin. Nutr. 2004;58(9):1211-6. http://doi.org/cw99wq.
32.Smith WJ, Underwood LE, Clemmons DR. Effects of caloric or protein restriction on insulin-like growth factor-I (IGF-I) and IGF-binding proteins in children and adults. J. Clin. Endocrinol. Metab. 1995;80(2):443-9. http://doi.org/bp34.
33.DeLellis K, Rinaldi S, Kaaks RJ, Kolonel LN, Henderson B, LeMarchand L. Dietary and lifestyle correlates of plasma insulin-like growth factor-I (IGF-I) and IGF binding protein-3 (IGFBP-3): the multiethnic cohort. Cancer Epidemiol. Biomarkers Prev. 2005;13(9):1444-51.
34.Baibas N, Bamia C, Vassilopoulou E, Sdrolias J, Trichopoulou A, Trichopoulos D. Dietary and lifestyle factors in relation to plasma insulin-like growth factor I in a general population simple. Eur. J. Cancer Prev. 2003;12(3):229-34. http://doi.org/bm8r52.
35. Claudio M, Benjamin F, Riccardo B, Massimiliano C, Francesco B, Luciano C. Adipocytes IGFBP-2 expression in prepubertal obese children. Obesity (Silver Spring). 2010;18(10):2055-7. http://doi.org/fgj58p.
36.Levi J, Huynh FK, Denroche HC, Neumann UH, Glavas MM, Covey SD, Kieffer TJ. Hepatic leptin signalling and subdiaphragmatic vagal efferents are not required for leptin-induced increases of plasma IGF binding protein-2 (IGFBP-2) in ob/ob mice. Diabetologia. 2012;55(3):752-62. http://doi.org/fzvp88.
37.Rosado EL, Monteiro JB, Chaia V, Lago MF. Efecto de la leptina en el tratamiento de la obesidad e influencia de la dieta en la secreción y acción de la hormona. Nutr. Hosp. 2006;21(6):686-93.
38.Hedbacker K, Birsoy K, Wysocki RW, Asilmaz E, Ahima RS, Farooqi IS, et al. Antidiabetic effects of IGFBP2, a leptin-regulated gene. Cell. Metab. 2010;11(1):11-22. http://doi.org/cmwg9j.
39.Figueroa JT. Relación entre estado nutricional, niveles séricos del factor de crecimiento similar a la insulina (IGF-1) y su proteína enlazante tipo 2 (IGFBP-2) en escolares de dos instituciones educativas de Bogotá y Soacha (2014). [Tesis Maestría]. Bogotá, D.C.: Facultad de Medicina, Universidad Nacional de Colombia; 2015.
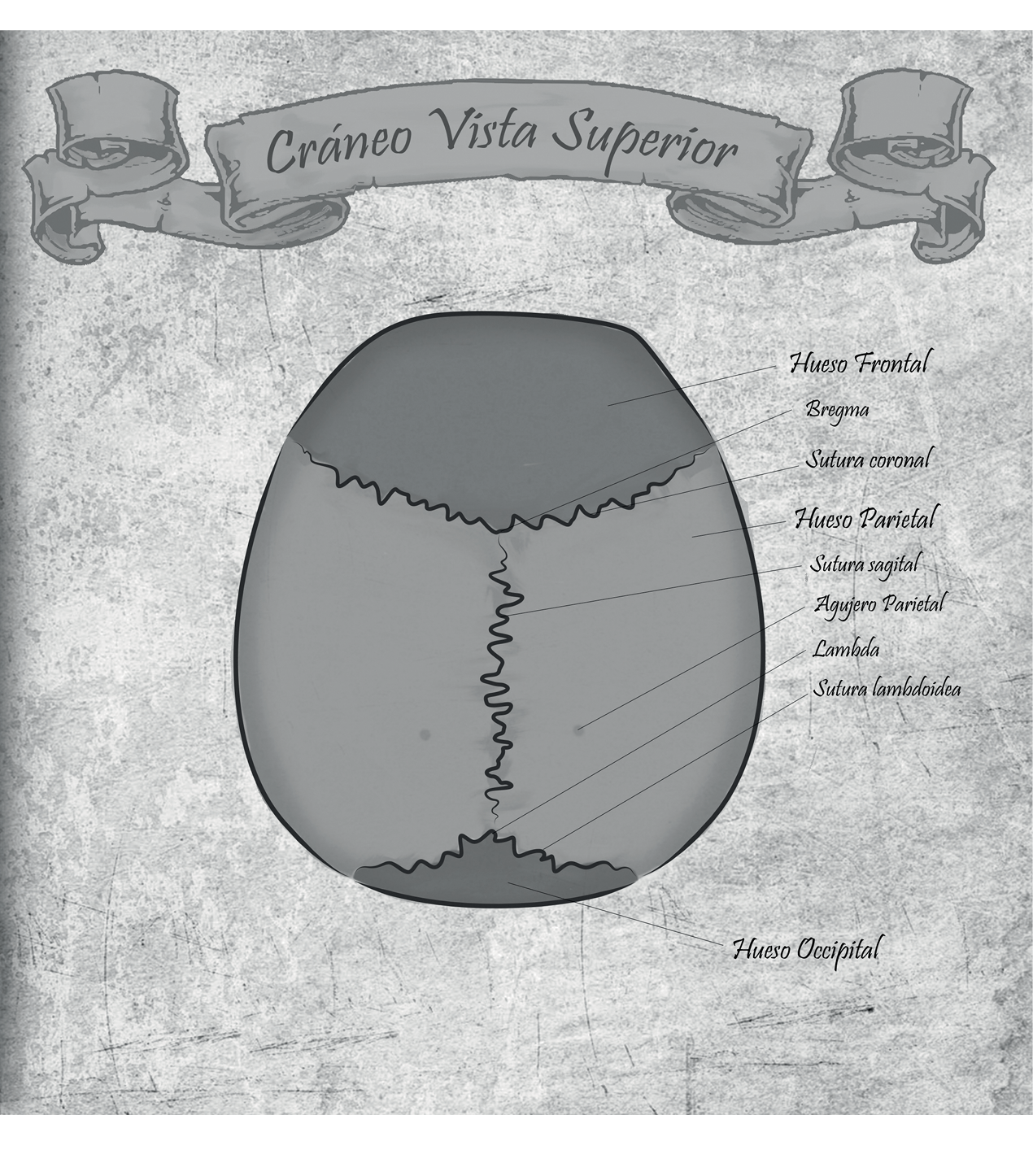
César Alexander Eslava Franco
“Mapas anatómicos”
Universidad Nacional de Colombia
Referencias
Latham MC. Nutrición Humana en el Mundo en Desarrollo. Roma: Organización para la Agricultura y la Alimentación; 2002 [cited 2016 Aug 26]. Available from: http://goo. gl/vHabFr.
Mcdonald B, Haddad L, Gross R, McLachlan M. Nutrición: Los argumentos a Favor. In: Comité permanente de nutrición del sistema de las Naciones Unidas, editor. Nutrición: La base para el desarrollo. Ginebra: Organización de las Naciones unidas; 2002 [cited 2016 Aug 25]. Available from: http://goo. gl/CgcuWf.
Fonseca-Centeno Z, Heredia-Vargas AP, Ocampo-Téllez R, Forero-Torres Y, Sarmiento-Dueñas OL, Álvarez-Uribe MC, et al. Encuesta Nacional de la Situación Nutricional en Colombia 2010 - ENSIN. Bogotá, D. C. : Instituto Colombiano de Bienestar Familiar; 2011.
Bonefeld K, Møller S. Insulin-like growth factor-I and the liver. Liver Int. 2011;31(7):911-9. http://doi. org/cdspbw.
Puche JE, Castilla-Córtazar I. Human conditions of insulin-like factor-I (IGF-1) deficiency. J. Transl. Med. 2012;10:224-53. http://doi. org/bp24.
Fontana L, Weiss EP, Villareal DT, Klein S, Holloszy JO. Long-term effects of calorie or protein restriction on serum IGF-1 and IGFBP-3 concentration in humans. Aging Cell. 2008;7(5):681-7. http://doi. org/cm44hc.
Holly J, Perks C. The Role of Insulin-Like Growth Factor Binding Proteins. Neuroendocrinology. 2006;83(3-4):154-60. http://doi. org/frw3nt.
Ko JM, Park HK, Yang S, Kim EY, Chung SC, Hwang IT. Association between insulin-like growth factor binding protein-2 levels and cardiovascular risk factors in Korean children. Endocr. J. 2012;59(4):335-43. http://doi. org/fzfztp.
Wheatcroft SB, Kearney MT, Shah AM, Ezzat VA, Miell JR, Modo M, et al. IGF-Binding Protein-2 Protects Against the Development of Obesity and Insulin Resistance. Diabetes. 2007;56(2):285-94.
http://doi. org/b936mv.
Heald AH, Kaushal K, Siddals KW, Rudenski AS, Anderson SG, Gibson JM. Insulin-like growth factor binding protein-2 (IGFBP-2) is a marker for the metabolic syndrome. Exp. Clin. Endocrinol. Diabetes. 2006;114(7):371-6. http://doi. org/cxkdxv.
Ministerio de la Protección Social, Instituto Nacional de Salud, Instituto Colombiano de Bienestar Familiar. Instructivo para la Implementación de los Patrones de Crecimiento de la OMS en Colombia para niños, niñas y adolescentes de 0 a 18 años. Bogotá, D. C. : Instituto Nacional de Salud; 2010.
McDowell MA, Fryar CD, Ogden CL. Anthropometric Reference Data for Children and Adults: United States 1988-1994. Washington, D. C. : National Center for Health Stadistics. Vital and Health Statistics 11 (249); 2009 [cited 2016 Aug 19]. Available from: http://goo. gl/elph8S.
Fajardo-Bonilla E, Ángel-Arango LA. Prevalencia de sobrepeso y obesidad, consumo de alimentos y patrón de actividad física en una población de niños escolares de la Ciudad de Bogotá. Rev Med. 2012;20(1):101-16.
Uscátegui-Peñuela RM, Álvarez-Uribe MC, Laguado-Salinas I, Soler-Terranova W, Martínez-Maluedas L, Arias-Arteaga R, et al. Factores de riesgo cardiovascular en niños de 6 a 18 años de Medellín (Colombia). An. Pediatr. 2003;58(5):411-7. http://doi. org/ck5b4w.
Yepez R, Carrasco F, Baldeón ME. Prevalencia de sobrepeso y obesidad en estudiantes adolescentes ecuatorianos del área urbana. Arch. Latinoam. Nutr. 2008;58(2):139-43.
Bustamante A, Seabra AF, Garganta RM, Maia JA. Efectos de la actividad física y del nivel socioeconómico en el sobrepeso y obesidad de escolares, Lima Este 2005. Rev. Perú. Med. Exp. Salud Pública. 2007;24(2):121-8.
Wisbaum W. La desnutrición infantil. Causas, consecuencias y estrategias para su prevención y tratamiento. Madrid: Unicef; 2011 [cited 2016 Aug 29] Available from: http://goo. gl/WeytGM.
Reyna L. Consecuencias de la obesidad en el niño y el adolescente: un problema que requiere atención. Rev. Peru Med. Exp. Salud Pública. 2012;29(3):357-60. http://doi. org/bp25.
Lobstein T, Baur L, Uauy R. Obesity in children and young people: a crisis in public health. Obes. Rev. 2004;5(Suppl 1):4-85. http://doi. org/ff3b4n.
Soliman AT, Elawwa A, Khella A, Saeed S, Yassin H. Linear growth in relation to the circulating concentration of insulin-like growth factor-I in young children with acyanotic congenital heart disease with left to right shunts before versus after surgical intervention. Indian J. Endocrinol. Metab. 2012;16(5):791-5. http://doi. org/bp26.
Wang J, Zhou J, Bondy CA. IGF-1 promotes longitudinal bone growth by insulin-like actions augmenting chondrocyte hypertrophy. FASEB J. 1999;13(14):1985-90.
Ranke MB, Schweizer R, Elmlinger MW, Weber K, Binder G, Schwarze CP, Wollmann HA. Significance of basal IGF-I, IGFBP-3 and IGFBP-2 measurements in the diagnostics of short stature in children. Horm. Res. 2000;54(2):60-8. http://doi. org/fhtmp4.
Turan S, Bereket A, Furman A, Omar A, Berber M, Ozen A, et al. The effect of economic status on height, insulin-like growth factor (IGF)-I and IGF binding protein-3 concentrations in healthy Turkish children. Eur. J. Clin. Nutr. 2007;61(6):752-8. http://doi. org/c7pkbq.
Nam SY, Lee EJ, Kim KR, Cha BS, Song YD, Lim SK, et al. Effect of obesity on total and free insulin-like growth factor (IGF)-1, and their relationship to IGF-binding protein (BP)-1, IGFBP-2, IGFBP-3, insulin, and growth hormone. Int. J. Obes. Relat. Metab. Disord. 1997;21(5):355-9. http://doi. org/dj67c4.
Mårin P, Kvist H, Lindstedt G, Sjöström L, Björntorp P. Low concentrations of insulin-like growth factor-I in abdominal obesity. Int. J. Obes. Relat. Metab. Disord. 1993;17(2):83-9.
Kong AP, Choi KC, Wong GW, Ko GT, Ho CS, Chan MH, et al. Serum concentrations of insulin-like growth factor-I, insulin-like growth factor binding protein-3 and cardiovascular risk factors in adolescents. Ann. Clin. Biochem. 2011;48(3):263-9. http://doi. org/dcrvb3.
Lewitt MS, Dent MS, Hall K. The Insulin-Like Growth Factor System in Obesity, Insulin Resistance and Type 2 Diabetes Mellitus. J. Clin. Med. 2014;3(4):1561-74. http://doi. org/bp33.
Sánchez-Gómez M, Malmlöf K, Mejía W, Bermúdez A, Ochoa MT, Carrasco-Rodríguez S, et al. Insulin-like growth factor-I, but not growth hormone, is dependent on a high protein intake to increase nitrogen balance in the rat. Br. J. Nutr. 1999;81(2):145-52.
Norat T, Dossus L, Rinaldi S, Overvad K, Grønbaek H, Tjønneland A, et al. Diet, serum insulin-like growth factor-I and IGF-binding protein-3 in European women. Eur. J. Clin. Nutr. 2007;61(1):91-8. http://doi. org/bkwwbk.
VandeHaar MJ, Moats-Staats BM, Davenport ML, Walker JL, Ketelslegers JM, Sharma BK, et al. Reduced serum concentrations of insulin-like growth factor-I (IGF-I) in protein-restricted growing rats is accompanied by reduced IGF-I mRNA levels in liver and skeletal muscle. J. Endocrinol. 1991;130(2):305-12. http://doi. org/db2hnj.
Hoppe C, Mølgaard C, Juul A, Michaelsen KF. High intakes of skimmed milk, but not meat, increase serum IGF-I and IGFBP-3 in eight-year-old boys. Eur. J. Clin. Nutr. 2004;58(9):1211-6. http://doi. org/cw99wq.
Smith WJ, Underwood LE, Clemmons DR. Effects of caloric or protein restriction on insulin-like growth factor-I (IGF-I) and IGF-binding proteins in children and adults. J. Clin. Endocrinol. Metab. 1995;80(2):443-9. http://doi. org/bp34.
DeLellis K, Rinaldi S, Kaaks RJ, Kolonel LN, Henderson B, LeMarchand L. Dietary and lifestyle correlates of plasma insulin-like growth factor-I (IGF-I) and IGF binding protein-3 (IGFBP-3): the multiethnic cohort. Cancer Epidemiol. Biomarkers Prev. 2005;13(9):1444-51.
Baibas N, Bamia C, Vassilopoulou E, Sdrolias J, Trichopoulou A, Trichopoulos D. Dietary and lifestyle factors in relation to plasma insulin-like growth factor I in a general population simple. Eur. J. Cancer Prev. 2003;12(3):229-34. http://doi. org/bm8r52.
Claudio M, Benjamin F, Riccardo B, Massimiliano C, Francesco B, Luciano C. Adipocytes IGFBP-2 expression in prepubertal obese children. Obesity (Silver Spring). 2010;18(10):2055-7. http://doi. org/fgj58p.
Levi J, Huynh FK, Denroche HC, Neumann UH, Glavas MM, Covey SD, Kieffer TJ. Hepatic leptin signalling and subdiaphragmatic vagal efferents are not required for leptin-induced increases of plasma IGF binding protein-2 (IGFBP-2) in ob/ob mice. Diabetologia. 2012;55(3):752-62. http://doi. org/fzvp88.
Rosado EL, Monteiro JB, Chaia V, Lago MF. Efecto de la leptina en el tratamiento de la obesidad e influencia de la dieta en la secreción y acción de la hormona. Nutr. Hosp. 2006;21(6):686-93.
Hedbacker K, Birsoy K, Wysocki RW, Asilmaz E, Ahima RS, Farooqi IS, et al. Antidiabetic effects of IGFBP2, a leptin-regulated gene. Cell. Metab. 2010;11(1):11-22. http://doi. org/cmwg9j.
Figueroa JT. Relación entre estado nutricional, niveles séricos del factor de crecimiento similar a la insulina (IGF-1) y su proteína enlazante tipo 2 (IGFBP-2) en escolares de dos instituciones educativas de Bogotá y Soacha (2014). [Tesis Maestría]. Bogotá, D. C. : Facultad de Medicina, Universidad Nacional de Colombia; 2015.
Cómo citar
APA
ACM
ACS
ABNT
Chicago
Harvard
IEEE
MLA
Turabian
Vancouver
Descargar cita
CrossRef Cited-by
1. Sorany Vera, Tatiana Figueroa, Luz Helena Aranzález, Ismena Mockus. (2020). Marcadores de riesgo cardiovascular en niños menores de 10 años y su relación con niveles séricos de IGF-1, IGFBP-1, IGFBP-2 e IGFBP-3. Revista de la Facultad de Medicina, 68(1) https://doi.org/10.15446/revfacmed.v68n1.69979.
Dimensions
PlumX
Visitas a la página del resumen del artículo
Descargas
Licencia
Derechos de autor 2017 Revista de la Facultad de Medicina

Esta obra está bajo una licencia Creative Commons Reconocimiento 3.0 Unported.
-


















