


Publicado
Phase analysis for the assessment of left ventricular dyssynchrony by Gated Myocardial Perfusion SPECT. Importance of clinical and technical parameters
Análisis de fase para la valoración del sincronismo mecánico del ventrículo izquierdo mediante Gated-SPECT de perfusión miocárdica. Importancia de los parámetros clínicos y técnicos
DOI:
https://doi.org/10.15446/revfacmed.v65n3.59488Palabras clave:
Myocardial Perfusion Imaging, Radionuclide Imaging, Cardiac Resynchronization Therapy (en)Imagen de perfusión miocárdica, Cintigrafía, Terapia de resincronización cardíaca (es)
Descargas
Introduction: Phase analysis (PA) of the left ventricle is a new tool in nuclear cardiology studies used to assess left ventricular mechanical timing based on different clinical applications. However, the use of this tool is relatively unknown.
Objective: To expose the feasibility of the new PA tool in myocardial perfusion (Gated-SPECT) to assess left ventricle mechanical timing, and to verify the differences between values depending on clinical and technical conditions.
Materials and methods: The study included consecutive patients evaluated by Gated-SPECT. The main variables were different depending on clinical and technical conditions. PA was assessed using the PHASE tool of the QPS-QGS program (Cedars-Sinai Medical Center, Los Angeles, USA). The following parameters were obtained: histogram bandwith (HB), standard deviation (SD) and entropy (E). A descriptive and analytical analysis of means and/or medians was performed using parametric or non-parametric tests. Statistical significance was p <0.05. IBM-SPSS V21® was used.
Results: 300 patients were included in this study with a mean age of 65±12.7. No differences were found in relation to the study phase (stress-rest) [HB (p=0.4), SD (p=0.6), E (p=0.8)], stress type [HB (p=0.38), SD (p=0.8), E (p=0.06), E (p=0.06)], dose used [HB (p=0.19), SD (p=0.05), E (p=0.06)], gamma camera [HB (p=0.02), SD (p=0.06), E (p=0.08)], or history of coronary heart disease [HB (p=0.44), SD (p=0.18), E (p=0.17)].
Furthermore, differences in conduction disorders were observed [HB (p=0.001), SD (p=0.02), E (p=0.001)], ejection fraction < or >35% (p=0.001), E (p=0.001)] normal or necrosis study [HB (p=0.001), SD (p=0.001), E (p=0.001)], and gender [HB (p=0.002), SD (p=0.006), E (p=0.005)].
Conclusions: The new PA tool of nuclear medicine is feasible in our context. The type of stress, the administered dose, the study phase or the gamma camera used did not affect the parameters. However, gender, interventricular conduction disorders, necrosis and systolic dysfunction did have an impact on them.
Introducción. El análisis de fase (AF) del ventrículo izquierdo es una herramienta de reciente introducción en los estudios de cardiología nuclear, que permite valorar el sincronismo mecánico de la contracción del ventrículo izquierdo con diferentes aplicaciones clínicas, si bien es poco conocida.
Objetivo. Mostrar la factibilidad de la nueva herramienta AF por perfusión miocárdica (Gated-SPECT) para valorar el sincronismo mecánico del ventrículo izquierdo y verificar diferencias entre sus valores, según situaciones clínicas y condiciones técnicas.
Materiales y métodos. En el estudio participaron pacientes consecutivos con Gated-SPECT. Las variables principales fueron diferentes condiciones clínicas y técnicas. La valoración del AF se realizó mediante la herramienta FASE del programa cardiodedicado (QPS-QGS, Cedars-Sinai Medical Center, Los Angeles, USA). Se obtuvieron los siguientes parámetros: ancho del histograma (AH), desviación estandar de la fase (DE) y entropía (E). Se realizó análisis descriptivo y analítico de medias o medianas a través de test paramétricos o no paramétircos. El límite de significancia estadísitca fue p<0.05. Se utilizó
IBM-SPSS V21®.
Resultados. Con un total de 300 pacientes y una media de edad de 65±12.7, en el análisis del AF no existieron diferencias según la fase del estudio (estrés-reposo) [AH (p=0.4), DE (p=0.6), E (p=0.7)], tipo de estrés [AH (p=0.38), DE (p=0.8), E (p=0.84)], dosis utilizada [AH(p=0.19), DE (p=0.05), E (p=0.06)], gammacámara [AH (p=0.02), DE (p=0.06), E (p=0.08)] ni entre antecedente de enfermedad coronaria [AH (p=0.44), DE (p=0.18), E (p=0.17)].
Hubo diferencias según trastornos de conducción [AH (p=0.001), DE (p=0.02), E (p=0.001)], fracción de eyección < o >35% [AH (p=0.001), DE (p=0.001), E (p=0.001)], estudio normal o con necrosis [AH (p=0.001), DE (p=0.001), E (p=0.001)] y género [AH (p=0.002), DE (p=0.006), E (p=0.005)].
Conclusiones. El uso de la nueva herramienta del AF de medicina nuclear es factible. Sus parámetros no se afectaron por el tipo de estrés producido, dosis administrada o fase del estudio por la gammacámara empleada. Por su parte, sí fueron afectados por género, trastornos de conducción interventricular, necrosis y disfunción sistólica.
original research
DOI: https://doi.org/10.15446/revfacmed.v65n3.59488
Phase analysis for the assessment of left ventricular dyssynchrony by Gated Myocardial Perfusion SPECT.
Importance of clinical and technical parameters
Análisis de fase para la valoración del sincronismo mecánico del ventrículo izquierdo mediante Gated-SPECT de perfusión miocárdica. Importancia de los parámetros clínicos y técnicos
Received: 08/08/2016. Accepted: 01/10/2016.
Víctor Marín-Oyaga1,3 • Claudia Gutiérrez-Villamil1,3 • Karen Dueñas-Criado2 • Sinay Arévalo-Leal1,3
1 Fundación Cardioinfantil - Instituto de Cardiología - Nuclear Medicine and Molecular Imaging Service - Bogotá D.C. - Colombia.
2 Fundación Cardioinfantil - Instituto de Cardiología - Clinical Cardiology and Cardiovascular Surgery Service - Bogotá D.C. - Colombia.
3 Universidad del Rosario - School of Medicine and Health Sciences - Bogotá D.C. - Colombia.
Corresponding author: Víctor Marín-Oyaga. Fundación Cardioinfantil - Instituto de Cardiología. Calle 163a No. 13B-60.
Phone number: +57 1 6672727, ext.: 11301. Bogotá D.C. Colombia. Email: vmarin@cardioinfantil.org.
| Abstract |
Introduction: Phase analysis (PA) of the left ventricle is a new tool in nuclear cardiology studies used to assess left ventricular mechanical timing based on different clinical applications. However, the use of this tool is relatively unknown.
Objective: To expose the feasibility of the new PA tool in myocardial perfusion (Gated-SPECT) to assess left ventricle mechanical timing, and to verify the differences between values depending on clinical and technical conditions.
Materials and methods: The study included consecutive patients evaluated by Gated-SPECT. The main variables were different depending on clinical and technical conditions. PA was assessed using the PHASE tool of the QPS-QGS program (Cedars-Sinai Medical Center, Los Angeles, USA). The following parameters were obtained: histogram bandwith (HB), standard deviation (SD) and entropy (E). A descriptive and analytical analysis of means and/or medians was performed using parametric or non-parametric tests. Statistical significance was p <0.05. IBM-SPSS V21® was used.
Results: 300 patients were included in this study with a mean age of 65±12.7. No differences were found in relation to the study phase (stress-rest) [HB (p=0.4), SD (p=0.6), E (p=0.8)], stress type [HB (p=0.38), SD (p=0.8), E (p=0.06), E (p=0.06)], dose used [HB (p=0.19), SD (p=0.05), E (p=0.06)], gamma camera [HB (p=0.02), SD (p=0.06), E (p=0.08)], or history of coronary heart disease [HB (p=0.44), SD (p=0.18), E (p=0.17)].
Furthermore, differences in conduction disorders were observed [HB (p=0.001), SD (p=0.02), E (p=0.001)], ejection fraction < or >35% (p=0.001), E (p=0.001)] normal or necrosis study [HB (p=0.001), SD (p=0.001), E (p=0.001)], and gender [HB (p=0.002), SD (p=0.006), E (p=0.005)].
Conclusions: The new PA tool of nuclear medicine is feasible in our context. The type of stress, the administered dose, the study phase or the gamma camera used did not affect the parameters. However, gender, interventricular conduction disorders, necrosis and systolic dysfunction did have an impact on them.
Keywords: Myocardial Perfusion Imaging; Radionuclide Imaging; Cardiac Resynchronization Therapy (MeSH).
Marín-Oyaga V, Gutiérrez-Villamil C, Dueñas-Criado K, Arévalo-Leal S. Phase analysis for the assessment of left ventricular dyssynchrony by Gated Myocardial Perfusion SPECT. Importance of clinical and technical parameters. Rev. Fac. Med. 2017;65(3):453-9. English. doi: https://doi.org/10.15446/revfacmed.v65n3.59488.
| Resumen |
Introducción. El análisis de fase (AF) del ventrículo izquierdo es una herramienta de reciente introducción en los estudios de cardiología nuclear, que permite valorar el sincronismo mecánico de la contracción del ventrículo izquierdo con diferentes aplicaciones clínicas, si bien es poco conocida.
Objetivo. Mostrar la factibilidad de la nueva herramienta AF por perfusión miocárdica (Gated-SPECT) para valorar el sincronismo mecánico del ventrículo izquierdo y verificar diferencias entre sus valores, según situaciones clínicas y condiciones técnicas.
Materiales y métodos. En el estudio participaron pacientes consecutivos con Gated-SPECT. Las variables principales fueron diferentes condiciones clínicas y técnicas. La valoración del AF se realizó mediante la herramienta FASE del programa cardiodedicado (QPS-QGS, Cedars-Sinai Medical Center, Los Angeles, USA). Se obtuvieron los siguientes parámetros: ancho del histograma (AH), desviación estandar de la fase (DE) y entropía (E). Se realizó análisis descriptivo y analítico de medias o medianas a través de test paramétricos o no paramétircos. El límite de significancia estadísitca fue p<0.05. Se utilizó
IBM-SPSS V21®.
Resultados. Con un total de 300 pacientes y una media de edad de 65±12.7, en el análisis del AF no existieron diferencias según la fase del estudio (estrés-reposo) [AH (p=0.4), DE (p=0.6), E (p=0.7)], tipo de estrés [AH (p=0.38), DE (p=0.8), E (p=0.84)], dosis utilizada [AH(p=0.19), DE (p=0.05), E (p=0.06)], gammacámara [AH (p=0.02), DE (p=0.06), E (p=0.08)] ni entre antecedente de enfermedad coronaria [AH (p=0.44), DE (p=0.18), E (p=0.17)].
Hubo diferencias según trastornos de conducción [AH (p=0.001), DE (p=0.02), E (p=0.001)], fracción de eyección < o >35% [AH (p=0.001), DE (p=0.001), E (p=0.001)], estudio normal o con necrosis [AH (p=0.001), DE (p=0.001), E (p=0.001)] y género [AH (p=0.002), DE (p=0.006), E (p=0.005)].
Conclusiones. El uso de la nueva herramienta del AF de medicina nuclear es factible. Sus parámetros no se afectaron por el tipo de estrés producido, dosis administrada o fase del estudio por la gammacámara empleada. Por su parte, sí fueron afectados por género, trastornos de conducción interventricular, necrosis y disfunción sistólica.
Palabras clave: Imagen de perfusión miocárdica; Cintigrafía; Terapia de resincronización cardíaca (DeCS).
Marín-Oyaga V, Gutiérrez-Villamil C, Dueñas-Criado K, Arévalo-Leal S. [Análisis de fase para la valoración del sincronismo mecánico del ventrículo izquierdo mediante Gated-SPECT de perfusión miocárdica. Importancia de los parámetros clínicos y técnicos]. Rev. Fac. Med. 2017;65(3):453-9. English. doi: https://doi.org/10.15446/revfacmed.v65n3.59488
Introduction
The prevalence of heart failure is rapidly increasing with major repercussions for patients and the health system. Cardiac resynchronization therapy (CRT) is a new treatment for symptoms associated with heart failure caused by cardiomyopathy and dyssynchrony during the ventricular contraction. Cardiac dyssynchrony is the uncoordinated distribution of electrical activation in the heart pathways, which can be observed in the disordered activation of contractile structures. When the electrical waves are altered or the contractile segments susceptible to stimulation fail, the time of onset of contraction varies with respect to the normal segments (1).
Some patients with cardiomyopathy and heart failure have abnormalities in the electrical system of the heart, such as complete left bundle branch block (LBBB), resulting in an uncoordinated (asynchronous) contraction of the heart muscle. Basically, the goal of CRT is to restore the coordinated action of ventricular pumping back to normal.
However, between 20% and 40% of patients with associated morbidity undergoing this expensive treatment do not show an adequate response (2). The best possible explanation for this phenomenon is that CRT selection criteria —the most relevant include the QRS complex width >120 milliseconds, and the ejection fraction <35% (3,4)— may be insufficient, since electrical synchrony may differ from the mechanical synchrony of the left ventricle. Therefore, it is highly important to carefully select candidates for this type of treatment, and to have the appropriate tools to establish the degree of left ventricular synchronism.
Gated myocardial perfusion by single-photon emission computerized tomography synchronized with electrocardiogram (Gated-SPECT) is widely used in nuclear medicine around the world to diagnose and provide prognosis for ischemic heart disease. It supplies information on global and regional ventricular function, coronary insufficiency and myocardial viability, since many patients with heart failure will undergo a Gated-SPECT as part of their study, and they could benefit from the addition of a new automated technique that allows assessing the left ventricle mechanical synchronism.
Some versions of this tool are already available in the processing programs used by nuclear cardiology studies. The technique is known as phase analysis (PA) by Gated-SPECT and was developed in 2005 by Chen et al. (5,6). It is intended to obtain basic information on myocardial perfusion, function parameters, left ventricle mechanical synchronism, and myocardial viability during the same study —which is useful for detecting non-viable territories which are not suitable for implantation of stimulation devices (7)—. Thus, phase analysis is an automatic, reproducible, simply to implement tool that is already included in the latest versions of the main processing programs available in nuclear cardiology (5,8-10). Gated-SPECT myocardial perfusion does not require extra time for its interpretation and is not a dependent operator (1,11).
To obtain the parameters for phase analysis with Gated-SPECT, complex mathematical calculations are performed on the synchronized study with the electrocardiogram to determine systolic thickening (12-14). The values are usually given in degrees (0º-360º), since this range comprises a period of time between the beginning and the end of each cardiac cycle. These values are obtained for each segment of the left ventricle analyzed and indicate at what point of the cycle the contraction begins (15). In this way, it is possible to measure the degree of synchronism of the ventricular contraction, considering that less synchrony implies greater temporal dispersion of contraction.
The main indication for the use of this technique is the prognostic evaluation of the patients who will undergo CRT, which determines if dyssynchrony detectable by usual methods translates into mechanical synchrony and, consequently, if these patients will receive some real benefit from the treatment. In addition, the role of Gated-SPECT becomes relevant when establishing the feasibility of the optimum placement site for the electrodes (16-20).
Furthermore, this technique has been used in patients with heart failure to predict cardiac events, differentiate ischemic heart disease from non-ischemic heart disease, and to predict cardiac events in patients with chronic diseases (21-25).
Different North American and European groups have carried out extensive studies to determine the normal values of the phase analysis parameters (5,11,26,27). Also, an attempt has been made to assess the factors that may or may not influence the parameters that result from the use of the tool, depending on methods, protocols, radiotracers or clinical conditions, among others (28-31). In spite of this, it is possible to see that there is still evidence that supports the definitive inclusion of the technique in clinical guidelines, management protocols and selection criteria of patients who will undergo a CRT.
It should be noted that despite the rapid knowledge and implementation of the technique in international clinical and research fields, there is a certain lack of knowledge about the technique and its availability in clinical practice and research among the medical specialists involved (nuclear physicians, clinical cardiologists and electrophysiologists) in almost the entire region in this context.
In consequence, the objectives of this study are to continue demonstrating the feasibility of the technique, to increase the knowledge of this tool within the local and regional scientific community, and to identify the influences and differences between the obtained values of the phase analysis with Gated-SPECT according to different clinical and technical conditions, usually in the daily practice of nuclear cardiology.
Materials and methods
A retrospective, analytical, observational and non-experimental study was designed in the nuclear medicine service of the institution where this service is provided. All consecutive patients who underwent a Gated-SPECT study of myocardial perfusion between February and March 2016, who had “raw” purchased studies available, were included in order to carry out the required analysis. Patients with a history of rhythm disorders similar to atrial fibrillation were excluded, since they do not allow achieving a good quality GS-PMI study.
The studies were done using two different gamma cameras. Ambulatory studies were usually performed on a Symbia T6 equipment (SIEMENS®), while an INFINIA HAWKEYE (GENERAL ELECTRIC®) equipment was used for hospitalized patients or emergency patients.
The radiopharmaceutical used was 99mTc-Sestamibi, and the doses administered ranged from 12 mCi (444 MBq) to 30 mCi (1110 MBq) per dose, with a total of 444 MBq (12 mCi) for patients requiring only the post-stress phase. The dose was 888 MBq (24 mCi) for those who required both phases on different days, and 1554 MBq (42 mCi) for those who required two phases on the same day. Patients with outpatient treatment followed a protocol of one or two days (post-stress and post-rest phases on the same day or on a different day) in the post-stress phase (pharmaceutical substance with intravenous dipyridamole or dobutamine or physical exercise) and in the post-rest phase. Inpatients or emergency patients followed a one-day protocol. When the post-stress study was normal, the post-rest phase was not performed due to radiation protection and quality measures.
Both gamma cameras have two heads located in 90° orientation with low energy and high-resolution collimators. Window pulse analyzers at 20% located in 140 KeV photopic were used. The matrix used was 64x64 with maximum zoom of 1.23. Thirty-two images of 20 seconds each were taken per head, for a total of 64 images in step and shot modality. In addition, contour orbit was made in a counterclockwise direction to verify the free execution of the rotation, without touching the patient or the stretcher, with 180° orbits and initial acquisition angle of -45°, with subsequent acquisitions up to 135°.
Tomographic reconstruction was performed using filtered back-projection (Butterworth filter of order 5, and cutoff frequency of 0.5), reorienting the axes of the heart to generate the coronal (short axis), sagittal (long vertical axis) and axial (horizontal long axis) sections. At least one physician with experience in nuclear cardiology carried out the normality assessment of a Gated-SPECT test, presence of ischemia or necrosis, and severity and extent.
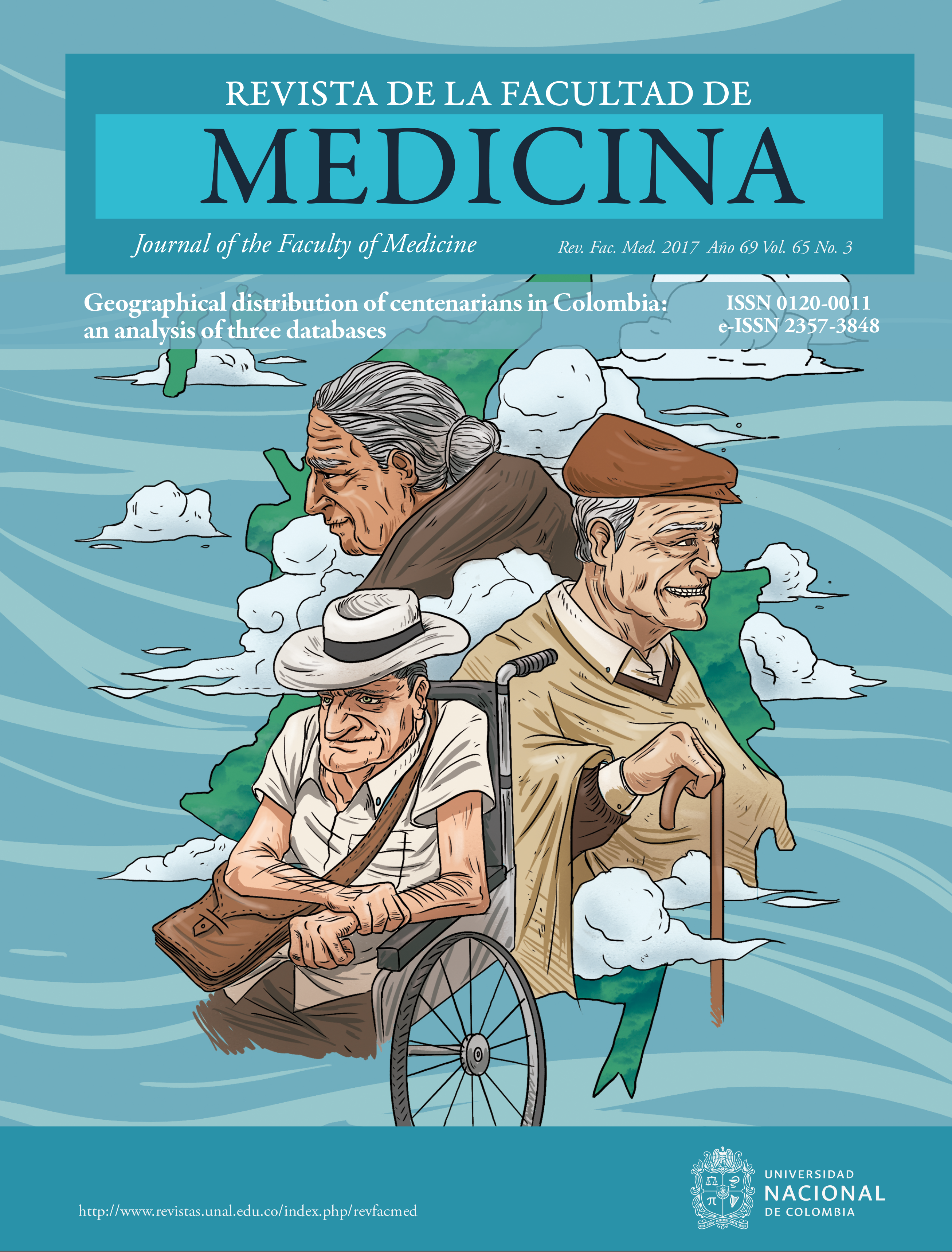
To assess the phase analysis of the studies, the PHASE tool of the QPS-QGS program (Cedars-Sinai Medical Center, Los Angeles, USA) was used. The following parameters were obtained from the phase analysis, as well as the corresponding histogram curves: histogram bandwidth (HB), which includes 95% of the values obtained during the measurement phase; standard deviation of the phase (SD), in reference to the distribution phase; entropy (E), a variability measure expressed as a percentage from 0% to 100%, where 0% corresponds to perfect synchrony, and 100% to the maximum possible dyssynchrony in the ventricular contraction, and average regarding the obtained angles. To date, SD and HB are the parameters considered for clinical assessment (14). The least useful recognized parameter is average, so it was excluded from this study. The final display of the tool showing PA parameters considered as normal and abnormal is shown in Figures 1 and 2.
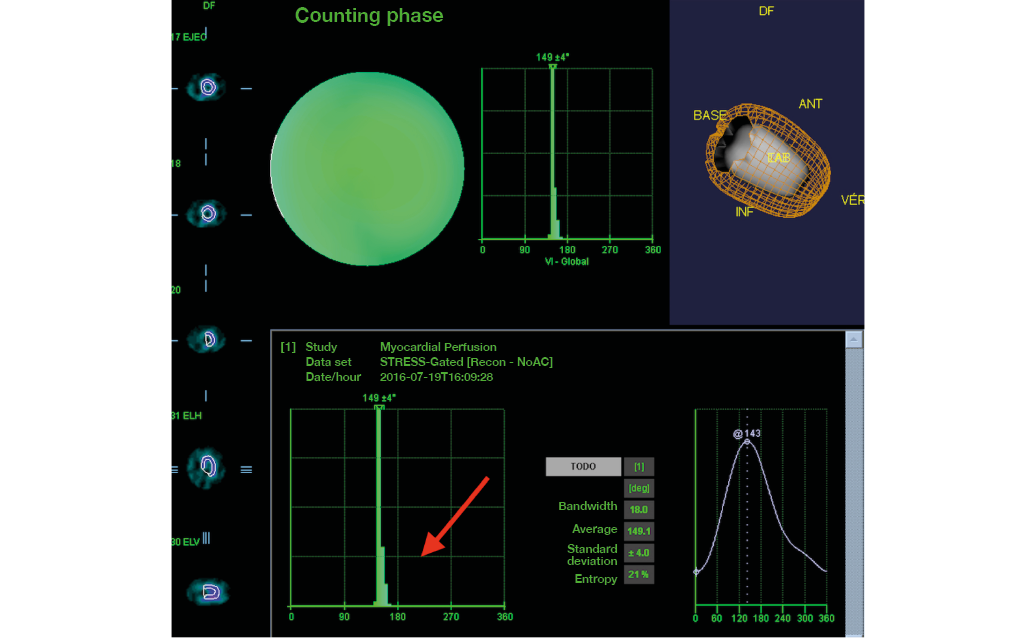
Figure 1. Female patient who underwent a Gated myocardial perfusion SPECT. Histogram representation of phase analysis with narrow bandwidth (arrow) and evidence of left ventricle mechanical synchronism.
Source: Own elaboration based on the data obtained in the study.

Figure 2. Phase analysis for left ventricular mechanical synchronism assessment by myocardial perfusion SPECT. Phase analysis in which wide bandwidth can be observed over the histogram with evidence of mechanical dyssynchrony of the left ventricle with septal predominance (arrows).
Source: Own elaboration based on the data obtained in the study.
The tool automatically yielded the quantitative parameters for the post-stress and post-rest phases. Based on these data, the corresponding analyzes and comparisons were made.
A descriptive analysis was performed using frequencies in the case of qualitative variables. On the other hand, quantitative variables, whether or not they followed a normal distribution (after applying the Kolmogorov-Smirnov normality test), were expressed by means and standard deviation or medians and interquartile range (IR). For the comparison of means or medians of the quantitative variables, parametric or non-parametric tests were used for independent or related samples, depending on the case. The value p <0.05 was taken as the limit to establish statistical significance. The IBM-SPSS V21® package was used for statistical analysis.
The protocol followed all relevant ethical recommendations and was formally reviewed and approved by the Ethics and Research Committees of Fundación Cardioinfantil - Instituto de Cardiología
Results
300 patients (117 women and 183 men), with a mean age of 65±12.7, were included. The most common indication for the study was chronic or acute chest pain (37.7%), followed by a history of coronary disease at follow-up (22.7%) and thoracic pain in patients with a history of known coronary disease (17%). The remaining 22.5% had other indications such as syncope study, recent arrhythmias, control of patients at cardiovascular risk, dyspnea, cardiac failure, myocardial viability assessment, and preoperative assessment. The technique was applied to all patients, since their study was properly synchronized with the electrocardiogram.
Of all patients, 31 (10.3%) had LBBB interventricular conduction disorders or a history of pacemaker implantation. Depending on the type of stress, 194 patients (64.7%) achieved vasodilator stress with intravenous dipyridamole; 94 (31.3%) with physical exercise test; 6 (2%) with dobutamine, and 6 (2%) with rest study, since they were requested to assess myocardial viability.
Of all the studies performed, 169 (56.9%) were interpreted as totally normal; 39 (13%) presented some degree of ischemia; 62 (20.7%) presented necrosis; 8 (3.7%) ischemia and necrosis, and 22 (7.3%) some type of finding other than ischemia or necrosis, but not considered as completely normal.
114 (38%) patients had their exam taken with a General-Electric® gamma camera and 186 (62%) with a Siemens® gamma camera.
An average dose of 1 GBq (27 mCi) per patient was given in one-day (23.3%) and two-day (62.3%) protocols. The stress-only protocol (12.3%) that was performed in hospitalized or emergency patients had normal results, therefore the rest study was not necessary. 8.7% of the patients presented an ejection fraction <35%, while the remaining 91.3% presented an ejection fraction >35%. The results shown and recorded in the tables are those obtained in the resting phase, except for patients who did not have a resting phase, which correspond to the aforementioned 12.3%.
When analyzing entirely technical factors, only normal perfusion studies were considered to avoid bias as much as possible, taking into account secondary parameter alterations in perfusion defects or synchronism of the patients. Thus, when analyzing normal perfusion studies, no differences were found in any of the parameters regardless of the type of stress exerted [HB (p=0.38), SD (p=0.8), E (p=0.84)], and used dose [HB (p=0.19), SD (p=0.05), E (p=0.06)]. Also, no differences between patients with or without a history of known coronary disease were observed [HB (p=0.44), SD (p=0.18), E (p=0.17)]. As for the gamma camera used, a difference in one of the parameters was found, while the other two did not show any [HB (p=0.02), SD (p=0.06), E (p=0.08)].
The analysis of PA parameters in patients undergoing both phases of the study (post-stress and post-rest) showed that there were no significant differences (analysis for related samples) when examining HB (p=0.4), SD (p=0.6) and E (p=0.7) in normal perfusion studies. On the other hand, when all the studies were analyzed, only differences in E values (p=0.01) could be observed, with no differences in HB (p=0.09) or SD (p=0.2).
Significant differences were found between the parameters of patients who had conduction disorders and those who did not: HB (p=0.001), SD (p=0.02), E (p=0.001). In turn, there were differences when comparing patients with ejection fraction greater or lower than 35% in all parameters, regardless of the phase: HB (p=0.001), SD (p=0.001), E (p=0.001).
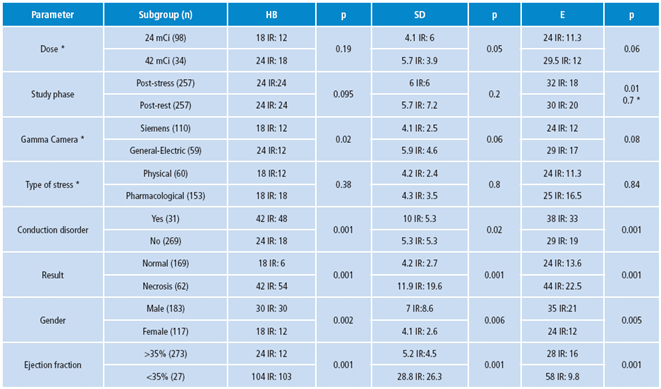
There were significant differences in all parameters when comparing normal perfusion studies with necrosis studies: HB (p=0.001), SD (p=0.001), E (p=0.001). The observation of the parameters in both normal perfusion studies and all studies showed significant differences between men and women in all parameters: HB (p=0.002), SD (p=0.006), E (p=0.005). The numerical values are shown in Table 1.
Table 1. Relevant results of phase analysis parameters.
|
Parameter |
Subgroup (n) |
HB |
p |
SD |
p |
E |
p |
|
Dose * |
24 mCi (98) |
18 IR: 12 |
0.19 |
4.1 IR: 6 |
0.05 |
24 IR: 11.3 |
0.06 |
|
42 mCi (34) |
24 IR: 18 |
5.7 IR: 3.9 |
29.5 IR: 12 |
||||
|
Study phase |
Post-stress (257) |
24 IR:24 |
0.095 |
6 IR:6 |
0.2 |
32 IR: 18 |
0.01 0.7 * |
|
Post-rest (257) |
24 IR: 24 |
5.7 IR: 7.2 |
30 IR: 20 |
||||
|
Gamma Camera * |
Siemens (110) |
18 IR: 12 |
0.02 |
4.1 IR: 2.5 |
0.06 |
24 IR: 12 |
0.08 |
|
General-Electric (59) |
24 IR:12 |
5.9 IR: 4.6 |
29 IR: 17 |
||||
|
Type of stress * |
Physical (60) |
18 IR:12 |
0.38 |
4.2 IR: 2.4 |
0.8 |
24 IR: 11.3 |
0.84 |
|
Pharmacological (153) |
18 IR: 18 |
4.3 IR: 3.5 |
25 IR: 16.5 |
||||
|
Conduction disorder |
Yes (31) |
42 IR: 48 |
0.001 |
10 IR: 5.3 |
0.02 |
38 IR: 33 |
0.001 |
|
No (269) |
24 IR: 18 |
5.3 IR: 5.3 |
29 IR: 19 |
||||
|
Result |
Normal (169) |
18 IR: 6 |
0.001 |
4.2 IR: 2.7 |
0.001 |
24 IR: 13.6 |
0.001 |
|
Necrosis (62) |
42 IR: 54 |
11.9 IR: 19.6 |
44 IR: 22.5 |
||||
|
Gender |
Male (183) |
30 IR: 30 |
0.002 |
7 IR:8.6 |
0.006 |
35 IR:21 |
0.005 |
|
Female (117) |
18 IR: 12 |
4.1 IR: 2.6 |
24 IR:12 |
||||
|
Ejection fraction |
>35% (273) |
24 IR: 12 |
0.001 |
5.2 IR:4.5 |
0.001 |
28 IR: 16 |
0.001 |
|
<35% (27) |
104 IR: 103 |
28.8 IR: 26.3 |
58 IR: 9.8 |
* Patients with normal Gated-SPECT.
IR: inrequartile range; HB: histogram bandwidth; SD: Standard deviation of the phase; E: entropy.
Source: Own elaboration based on data obtained in the study.
Discussion
This research demonstrates the feasibility of the technique known as phase analysis of gated SPECT myocardial perfusion in nuclear medicine services and, therefore, in the current context of the profession. This is an automatic tool that is easy to apply to all Gated-SPECT studies and has gradually increased its usefulness worldwide.
The study did not show differences between parameters in both phases when examining only the normal studies. Only differences in entropy were found in all studies. These results are similar to those found by Zhou et al. (32), who studied 60 patients without finding differences between PA parameters in post-stress and post-rest studies. This is one of the most relevant findings of this study and is of great importance, since many nuclear medicine services conduct Gated-SPECT studies only in the post-rest phase, while other studies (as this one) do not include the post-rest phase if the post-stress phase is normal. The results show that the tool can be used in any of the phases without differences in the results. Furthermore, no dose-dependent differences were found, which is important since not all services, phases and patients use the same doses of radiotracer.
No relevant differences were found in relation to stress type (physical or pharmacological). This is of great importance because the type of stress can be provided in the aforementioned manners without affecting PA parameters based on the type of patient or clinical indication. Additionally, whether or not a patient has a known coronary disease does not seem to be influential, as long as the perfusion study is normal. That one of the analyzed parameters showed differences while the other two did not show any depending on the gamma camera used, which implies that it could be completely confirmed in other studies, although there is a trend towards non-difference.
As expected, significant differences were found between patients with and without conduction disorders when comparing all studies. In consequence, it is possible to effectively differentiate patients without conduction disorders from those with electrical synchronism alterations and left ventricle mechanical synchronism alterations. This finding is similar to other studies, and confirms the usefulness of the technique in this regard (11,14,26). However, the real usefulness of the tool, rather than discriminating between patients with or without conduction disorders, is to determine the cut-off points of the parameters of the phase analysis, which will help to establish if patients would respond or not to the CRT, although, this is not an objective of this study.
Moreover, differences were found among PA parameters regarding gender. When observing all studies or only normal studies, the parameters were higher in men than in women. The most relevant studies published that sought to obtain normal values and cut-off points of normality were carried out by Chen et al. (5) and Romero-Farina et al. (11), which also showed these differences. Thus, normality parameters should be considered for each gender.
Similarly, significant differences were observed between patients with normal myocardial perfusion studies and necrosis, as well as between patients with or without major systolic dysfunction (ejection fraction < or >35%, respectively). These results are consistent with other studies that included patients with necrosis or systolic dysfunction, and showed that the degree of left ventricular mechanical dyssynchrony is directly related to systolic dysfunction and to the extent of perfusion defects (33,34).
Continuing this type of studies is important to familiarize the branches of medicine involved (nuclear medicine and cardiology) with the tool and its clinical utility, to gradually resolve any concerns that may arise from it.
A possible limitation of the study, and a possible source of error, is its retrospective character. With this in mind, the methodology and results obtained make it difficult to perform an adequate multivariate analysis to assess the influence of some variables on others.
Another factor that should be considered is that, when referring normal perfusion studies, patients are not necessarily completely normal from a clinical cardiovascular point of view, but are patients with normal perfusion studies. This occurs because few clinically normal patients who require myocardial perfusion studies are referred to these services. Likewise, as the clinical implementation of the tool increases, the number of clinically normal patients who would benefit from the study decreases.
In addition, this article approaches clinical reality without having normal patients as a direct objective, but considering the patients who, in general, are studied in myocardial perfusion investigations and those who would receive potential benefits from the technique.
Conclusions
The use of the phase analysis tool included in the main programs for the processing of myocardial perfusion studies is feasible in the current professional context and can be used in the corresponding clinical scenario.
The parameters of the phase analysis are not affected and can, therefore, be used without depending on the type of stress (physical or pharmacological), the dose administered, the phase of the study in which the test is performed (post-stress or post-rest), or the gamma camera used.
Nevertheless, these parameters are affected by the variables of the patients themselves, such as gender (which must have normal values), the presence of intracardiac conduction disorders or fixed perfusion defects considered as necrosis, and systolic dysfunction.
Conflict of interest
None stated by the authors.
Funding
The author was financially supported by the Fellow Clinical Research Program of Fundación Cardioinfantil - Instituto de Cardiología. The organization had no direct influence on the design and development of the study.
Acknowledgement
None stated by the authors.
References
1.Yaghoobi N, Malek H. The Age of Reason for Gated SPECT MPI to Deal With Cardiac Dyssynchrony. Res Cardiovasc Med. 2015;4(1):e25851. http://doi.org/b4zg.
2.Nakamura K, Takami M, Shimabukuro M, Maesato A, Chinen I, Ishigaki S, et al. Effective prediction of response to cardiac resynchronization therapy using a novel program of gated myocardial perfusion single photon emission computed tomography. Europace. 2011;13(12):1731-7. http://doi.org/dfxtfb.
3.Brignole M, Auricchio A, Baron-Esquivias G, Bordachar P, Boriani G, Breithardt OA, et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur Heart J. 2013;34(29):2281-329. http://doi.org/f22ff8.
4.Tracy CM, Epstein AE, Darbar D, Dimarco JP, Dunbar SB, Estes MNA III, et al. 2012 ACCF/AHA/HRS focused update of the 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2012;60(14):1297-313. http://doi.org/f2nbt7.
5.Chen J, Garcia EV, Folks RD, Cooke CD, Faber TL, Tauxe EL, et al. Onset of left ventricular mechanical contraction as determined by phase analysis of ECG-gated myocardial perfusion SPECT imaging: development of a diagnostic tool for assessment of cardiac mechanical dyssynchrony. J Nucl Cardiol. 2005;12(6):687-95. http://doi.org/b384d4.
6.Casáns-Tormo I, Jurado-López JA. Diagnóstico de la enfermedad coronaria mediante gated-SPECT de perfusión miocárdica. Revista Española de Cardiología Suplementos. 2008;8(2):15B-24B. http://doi.org/bj5tgb.
7.Ypenburg C, Schalij MJ, Bleeker GB, Steendijk P, Boersma E, Dibbets-Schneider P, et al. Impact of viability and scar tissue on response to cardiac resynchronization therapy in ischaemic heart failure patients. Eur Heart J. 2007;28(1):33-41. http://doi.org/dh3cwj.
8.Matsuo S. Phase analysis using gated myocardial perfusion single-photon emission computed tomography imaging for evaluating cardiac dyssynchrony. Circ J. 2012;76(8):1832-3. http://doi.org/b4zh.
9.Leva L, Brambilla M, Cavallino C, Matheoud R, Occhetta E, Marino P, et al. Reproducibility and variability of global and regional dyssynchrony parameters derived from phase analysis of gated myocardial perfusion SPECT. Q J Nucl Med Mol Imaging. 2012;56(2):209-17.
10.Trimble MA, Velazquez EJ, Adams GL, Honeycutt EF, Pagnanelli RA, Barnhart HX, et al. Repeatability and reproducibility of phase analysis of gated single-photon emission computed tomography myocardial perfusion imaging used to quantify cardiac dyssynchrony. Nucl Med Commun. 2008;29(4):374-81. http://doi.org/cg2dgz.
11.Romero-Farina G, Aguadé-Bruix S, Candell-Riera J, Pizzi MN, García-Dorado D. Cut-off values of myocardial perfusion gated-SPECT phase analysis parameters of normal subjects, and conduction and mechanical cardiac diseases. J Nucl Cardiol. 2015;22(6):1247-58. http://doi.org/f7sz5c.
12.Chen J, Kalogeropoulos AP, Verdes L, Butler J, Garcia EV. Left-ventricular systolic and diastolic dyssynchrony as assessed by multi-harmonic phase analysis of gated SPECT myocardial perfusion imaging in patients with end-stage renal disease and normal LVEF. J Nucl Cardiol. 2011;18(2):299-308. http://doi.org/fmgnn4.
13.Gutiérrez L, Peñafort F, Seretti I, Ortego R. Nuevas herramientas diagnósticas en Insuficiencia Cardiaca: análisis de fase mediante SPECT-Gatillado para evaluación de sincronía miocárdica. Rev Fed Arg Cardiol. 2013;42(2):102-12.
14.Van Kriekinge SD, Nishina H, Ohba M, Berman DS, Germano G. Automatic global and regional phase analysis from gated myocardial perfusion SPECT imaging: application to the characterization of ventricular contraction in patients with left bundle branch block. J Nucl Med. 2008;49(11):1790-7. http://doi.org/bfjd4b.
15.Beretta M, Mut F. Valoración de la sincronía mecánica del ventrículo izquierdo mediante Gated SPECT y análisis de fase. Alasbimn Journal. 2012 [cited 2017 Mar 30]. Available from: http://goo.gl/3dUTZf.
16.Chen J, Garcia EV, Bax JJ, Iskandrian AE, Borges-Neto S, Soman P. SPECT myocardial perfusion imaging for the assessment of left ventricular mechanical dyssynchrony. J Nucl Cardiol. 2011;18(4):685-94. http://doi.org/b4vw84.
17.Boogers MJ, Chen J, Van Bommel RJ, Borleffs CJ, Dibbets-Schneider P, van der Hiel B, et al. Optimal left ventricular lead position assessed with phase analysis on gated myocardial perfusion SPECT. Eur J Nucl Med Mol Imaging. 2011;38(2):230-8. http://doi.org/cjt428.
18.Lin X, Xu H, Zhao X, Chen J. Sites of latest mechanical activation as assessed by SPECT myocardial perfusion imaging in ischemic and dilated cardiomyopathy patients with LBBB. Eur J Nucl Med Mol Imaging. 2014;41(6):1232-9. http://doi.org/b4zj.
19.Chen J, Henneman MM, Trimble MA, Bax JJ, Borges-Neto S, Iskandrian AE, et al. Assessment of left ventricular mechanical dyssynchrony by phase analysis of ECG-gated SPECT myocardial perfusion imaging. J Nucl Cardiol. 2008;15(1):127-36. http://doi.org/bpfjb8.
20.Boogers MM, Chen J, Bax JJ. Myocardial perfusion single photon emission computed tomography for the assessment of mechanical dyssynchrony. Curr Opin Cardiol. 2008;23(5):431-9. http://doi.org/dsx8xk.
21.Peix A, Karell J, Rodríguez L, Cabrera LO, Padrón K, Carrillo R, et al. Gated SPECT myocardial perfusion imaging, intraventricular synchronism, and cardiac events in heart failure. Clin Nucl Med. 2014;36(6):498-504. http://doi.org/b4zk.
22.Zafrir N, Bental T, Strasberg B, Solodky A, Mats I, Gutstein A, et al. Yield of left ventricular dyssynchrony by gated SPECT MPI in patients with heart failure prior to implantable cardioverter-defibrillator or cardiac resynchronization therapy with a defibrillator: Characteristics and prediction of cardiac outcome. J Nucl Cardiol. 2015;24(1):122-9. http://doi.org/f9phkb.
23.Hage FG. Left ventricular mechanical dyssynchrony by phase analysis as a prognostic indicator in heart failure. J Nucl Cardiol. 2014;21(1):67-70. http://doi.org/b4zm.
24.Azizian N, Rastgou F, Ghaedian T, Golabchi A, Bahadorian B, Khanlarzadeh V, et al. LV Dyssynchrony Assessed With Phase Analysis on Gated Myocardial Perfusion SPECT Can Predict Response to CRT in Patients With End-Stage Heart Failure. Res Cardiovasc Med. 2014;3(4):e20720. http://doi.org/b4zn.
25.Uebleis C, Hellweger S, Laubender RP, Becker A, Sohn HY, Lehner S, et al. Left ventricular dyssynchrony assessed by gated SPECT phase analysis is an independent predictor of death in patients with advanced coronary artery disease and reduced left ventricular function not undergoing cardiac resynchronization therapy. Eur J Nucl Med Mol Imaging. 2012;39(10):1561-9. http://doi.org/b4zp.
26.Trimble MA, Borges-Neto S, Honeycutt EF, Shaw LK, Pagnanelli R, Chen J, et al. Evaluation of mechanical dyssynchrony and myocardial perfusion using phase analysis of gated SPECT imaging in patients with left ventricular dysfunction. J Nucl Cardiol. 2008;15(5):663-70. http://doi.org/fhnksf.
27.Henneman MM, Chen J, Ypenburg C, Dibbets P, Bleeker GB, Boersma E, et al. Phase analysis of gated myocardial perfusion single-photon emission computed tomography compared with tissue Doppler imaging for the assessment of left ventricular dyssynchrony. J Am Coll Cardiol. 2007;49(16):1708-14. http://doi.org/bfzcsd.
28.AlJaroudi W, Jaber WA, Grimm RA, Marwick T, Cerqueira MD. Alternative methods for the assessment of mechanical dyssynchrony using phase analysis of gated single photon emission computed tomography myocardial perfusion imaging. Int J Cardiovasc Imaging. 2012;28(6):1385-94. http://doi.org/bphd24.
29.Rastgou F, Shojaeifard M, Amin A, Ghaedian T, Firoozabadi H, Malek H, et al. Assessment of left ventricular mechanical dyssynchrony by phase analysis of gated-SPECT myocardial perfusion imaging and tissue Doppler imaging: comparison between QGS and ECTb software packages. J Nucl Cardiol. 2014;21(6):1062-71. http://doi.org/b4zq.
30.AlJaroudi W, Alraies MC, DiFilippo F, Brunken RC, Cerqueira MD, Jaber WA. Effect of stress testing on left ventricular mechanical synchrony by phase analysis of gated positron emission tomography in patients with normal myocardial perfusion. Eur J Nucl Med Mol Imaging. 2012;39(4):665-72. http://doi.org/fzq39d.
31.Chen CC, Huang WS, Hung GU, Chen WC, Kao CH, Chen J. Left-ventricular dyssynchrony evaluated by Tl-201 gated SPECT myocardial perfusion imaging: a comparison with Tc-99m sestamibi. Nucl Med Commun. 2013;34(3):229-32. http://doi.org/f44vr4.
32.Zhou Y, Li D, Feng J, Yuan D, Patel Z, Cao K, et al. Left Ventricular Dyssynchrony Parameters Measured by Phase Analysis of Post-stress and Resting Gated SPECT Myocardial Perfusion Imaging. World J Nucl Med. 2013;12(1):3-7. http://doi.org/b4zr.
33.Wang J, Wang Y, Zhang X, Zhou R, Niu R, Lu P. [Left ventricular systolic synchrony assessed by phase analysis of gated myocardial perfusion imaging in patients with old myocardial infarction]. Zhonghua Xin Xue Guan Bing Za Zhi. 2015;43(7):599-604. Chinese.
34.Vidigal-Ferreira MJ, Silva R, Cabanelas N, Cunha MJ, Ramos D, Albuquerque A, et al. Left ventricular mechanical dyssynchrony in patients with impaired left ventricular function undergoing gated SPECT myocardial perfusion imaging. Rev Port Cardiol. 2013;32(5):387-94. http://doi.org/f2j5vt.
Iván “Ivanquio” Benavides
“El niño vacío” – 005
Técnica: tinta, color digital
Recibido: 8 de agosto de 2016; Aceptado: 1 de octubre de 2016
Abstract
Introduction:
Phase analysis (PA) of the left ventricle is a new tool in nuclear cardiology studies used to assess left ventricular mechanical timing based on different clinical applications. However, the use of this tool is relatively unknown.
Objective:
To expose the feasibility of the new PA tool in myocardial perfusion (Gated-SPECT) to assess left ventricle mechanical timing, and to verify the differences between values depending on clinical and technical conditions.
Materials and methods:
The study included consecutive patients evaluated by Gated-SPECT. The main variables were different depending on clinical and technical conditions. PA was assessed using the PHASE tool of the QPS-QGS program (Cedars-Sinai Medical Center, Los Angeles, USA). The following parameters were obtained: histogram bandwith (HB), standard deviation (SD) and entropy (E). A descriptive and analytical analysis of means and/or medians was performed using parametric or non-parametric tests. Statistical significance was p <0.05. IBM-SPSS V21® was used.
Results:
300 patients were included in this study with a mean age of 65±12.7. No differences were found in relation to the study phase (stress-rest) [HB (p=0.4), SD (p=0.6), E (p=0.8)], stress type [HB (p=0.38), SD (p=0.8), E (p=0.06), E (p=0.06)], dose used [HB (p=0.19), SD (p=0.05), E (p=0.06)], gamma camera [HB (p=0.02), SD (p=0.06), E (p=0.08)], or history of coronary heart disease [HB (p=0.44), SD (p=0.18), E (p=0.17)].
Furthermore, differences in conduction disorders were observed [HB (p=0.001), SD (p=0.02), E (p=0.001)], ejection fraction < or >35% (p=0.001), E (p=0.001)] normal or necrosis study [HB (p=0.001), SD (p=0.001), E (p=0.001)], and gender [HB (p=0.002), SD (p=0.006), E (p=0.005)].
Conclusions:
The new PA tool of nuclear medicine is feasible in our context. The type of stress, the administered dose, the study phase or the gamma camera used did not affect the parameters. However, gender, interventricular conduction disorders, necrosis and systolic dysfunction did have an impact on them.
Keywords:
Myocardial Perfusion Imaging, Radionuclide Imaging, Cardiac Resynchronization Therapy (MeSH).Resumen
Introducción.
El análisis de fase (AF) del ventrículo izquierdo es una herramienta de reciente introducción en los estudios de cardiología nuclear, que permite valorar el sincronismo mecánico de la contracción del ventrículo izquierdo con diferentes aplicaciones clínicas, si bien es poco conocida.
Objetivo.
Mostrar la factibilidad de la nueva herramienta AF por perfusión miocárdica (Gated-SPECT) para valorar el sincronismo mecánico del ventrículo izquierdo y verificar diferencias entre sus valores, según situaciones clínicas y condiciones técnicas.
Materiales y métodos.
En el estudio participaron pacientes consecutivos con Gated-SPECT. Las variables principales fueron diferentes condiciones clínicas y técnicas. La valoración del AF se realizó mediante la herramienta FASE del programa cardiodedicado (QPS-QGS, Cedars-Sinai Medical Center, Los Angeles, USA). Se obtuvieron los siguientes parámetros: ancho del histograma (AH), desviación estandar de la fase (DE) y entropía (E). Se realizó análisis descriptivo y analítico de medias o medianas a través de test paramétricos o no paramétircos. El límite de significancia estadísitca fue p<0.05. Se utilizó IBM-SPSS V21®.
Resultados.
Con un total de 300 pacientes y una media de edad de 65±12.7, en el análisis del AF no existieron diferencias según la fase del estudio (estrés-reposo) [AH (p=0.4), DE (p=0.6), E (p=0.7)], tipo de estrés [AH (p=0.38), DE (p=0.8), E (p=0.84)], dosis utilizada [AH(p=0.19), DE (p=0.05), E (p=0.06)], gammacámara [AH (p=0.02), DE (p=0.06), E (p=0.08)] ni entre antecedente de enfermedad coronaria [AH (p=0.44), DE (p=0.18), E (p=0.17)].
Hubo diferencias según trastornos de conducción [AH (p=0.001), DE (p=0.02), E (p=0.001)], fracción de eyección < o >35% [AH (p=0.001), DE (p=0.001), E (p=0.001)], estudio normal o con necrosis [AH (p=0.001), DE (p=0.001), E (p=0.001)] y género [AH (p=0.002), DE (p=0.006), E (p=0.005)].
Conclusiones.
El uso de la nueva herramienta del AF de medicina nuclear es factible. Sus parámetros no se afectaron por el tipo de estrés producido, dosis administrada o fase del estudio por la gammacámara empleada. Por su parte, sí fueron afectados por género, trastornos de conducción interventricular, necrosis y disfunción sistólica.
Palabras clave:
Imagen de perfusión miocárdica, Cintigrafía, Terapia de resincronización cardíaca (DeCS).Introduction
The prevalence of heart failure is rapidly increasing with major repercussions for patients and the health system. Cardiac resynchronization therapy (CRT) is a new treatment for symptoms associated with heart failure caused by cardiomyopathy and dyssynchrony during the ventricular contraction. Cardiac dyssynchrony is the uncoordinated distribution of electrical activation in the heart pathways, which can be observed in the disordered activation of contractile structures. When the electrical waves are altered or the contractile segments susceptible to stimulation fail, the time of onset of contraction varies with respect to the normal segments 1.
Some patients with cardiomyopathy and heart failure have abnormalities in the electrical system of the heart, such as complete left bundle branch block (LBBB), resulting in an uncoordinated (asynchronous) contraction of the heart muscle. Basically, the goal of CRT is to restore the coordinated action of ventricular pumping back to normal.
However, between 20% and 40% of patients with associated morbidity undergoing this expensive treatment do not show an adequate response 2. The best possible explanation for this phenomenon is that CRT selection criteria -the most relevant include the QRS complex width >120 milliseconds, and the ejection fraction <35% 3,4- may be insufficient, since electrical synchrony may differ from the mechanical synchrony of the left ventricle. Therefore, it is highly important to carefully select candidates for this type of treatment, and to have the appropriate tools to establish the degree of left ventricular synchronism.
Gated myocardial perfusion by single-photon emission computerized tomography synchronized with electrocardiogram (Gated-SPECT) is widely used in nuclear medicine around the world to diagnose and provide prognosis for ischemic heart disease.
It supplies information on global and regional ventricular function, coronary insufficiency and myocardial viability, since many patients with heart failure will undergo a Gated-SPECT as part of their study, and they could benefit from the addition of a new automated technique that allows assessing the left ventricle mechanical synchronism.
Some versions of this tool are already available in the processing programs used by nuclear cardiology studies. The technique is known as phase analysis (PA) by Gated-SPECT and was developed in 2005 by Chen et al. 5,6. It is intended to obtain basic information on myocardial perfusion, function parameters, left ventricle mechanical synchronism, and myocardial viability during the same study -which is useful for detecting non-viable territories which are not suitable for implantation of stimulation devices 7-. Thus, phase analysis is an automatic, reproducible, simply to implement tool that is already included in the latest versions of the main processing programs available in nuclear cardiology 5,8-10. Gated-SPECT myocardial perfusion does not require extra time for its interpretation and is not a dependent operator 1,11.
To obtain the parameters for phase analysis with Gated-SPECT, complex mathematical calculations are performed on the synchronized study with the electrocardiogram to determine systolic thickening 12-14. The values are usually given in degrees (0°-360°), since this range comprises a period of time between the beginning and the end of each cardiac cycle. These values are obtained for each segment of the left ventricle analyzed and indicate at what point of the cycle the contraction begins 15. In this way, it is possible to measure the degree of synchronism of the ventricular contraction, considering that less synchrony implies greater temporal dispersion of contraction.
The main indication for the use of this technique is the prognostic evaluation of the patients who will undergo CRT, which determines if dyssynchrony detectable by usual methods translates into mechanical synchrony and, consequently, if these patients will receive some real benefit from the treatment. In addition, the role of Gated-SPECT becomes relevant when establishing the feasibility of the optimum placement site for the electrodes 16-20.
Furthermore, this technique has been used in patients with heart failure to predict cardiac events, differentiate ischemic heart disease from non-ischemic heart disease, and to predict cardiac events in patients with chronic diseases 21-25.
Different North American and European groups have carried out extensive studies to determine the normal values of the phase analysis parameters 5,11,26,27. Also, an attempt has been made to assess the factors that may or may not influence the parameters that result from the use of the tool, depending on methods, protocols, radiotracers or clinical conditions, among others 28-31. In spite of this, it is possible to see that there is still evidence that supports the definitive inclusion of the technique in clinical guidelines, management protocols and selection criteria of patients who will undergo a CRT.
It should be noted that despite the rapid knowledge and implementation of the technique in international clinical and research fields, there is a certain lack of knowledge about the technique and its availability in clinical practice and research among the medical specialists involved (nuclear physicians, clinical cardiologists and electrophysiologists) in almost the entire region in this context.
In consequence, the objectives of this study are to continue demonstrating the feasibility of the technique, to increase the knowledge of this tool within the local and regional scientific community, and to identify the influences and differences between the obtained values of the phase analysis with Gated-SPECT according to different clinical and technical conditions, usually in the daily practice of nuclear cardiology.
Materials and methods
A retrospective, analytical, observational and non-experimental study was designed in the nuclear medicine service of the institution where this service is provided. All consecutive patients who underwent a Gated-SPECT study of myocardial perfusion between February and March 2016, who had "raw" purchased studies available, were included in order to carry out the required analysis. Patients with a history of rhythm disorders similar to atrial fibrillation were excluded, since they do not allow achieving a good quality GS-PMI study.
The studies were done using two different gamma cameras. Ambulatory studies were usually performed on a Symbia T6 equipment (SIEMENS®), while an INFINIA HAWKEYE (GENERAL ELECTRIC®) equipment was used for hospitalized patients or emergency patients.
The radiopharmaceutical used was 99mTc-Sestamibi, and the doses administered ranged from 12 mCi (444 MBq) to 30 mCi (1110 MBq) per dose, with a total of 444 MBq (12 mCi) for patients requiring only the post-stress phase. The dose was 888 MBq (24 mCi) for those who required both phases on different days, and 1554 MBq (42 mCi) for those who required two phases on the same day. Patients with outpatient treatment followed a protocol of one or two days (poststress and post-rest phases on the same day or on a different day) in the post-stress phase (pharmaceutical substance with intravenous dipyridamole or dobutamine or physical exercise) and in the post-rest phase. Inpatients or emergency patients followed a one-day protocol. When the post-stress study was normal, the post-rest phase was not performed due to radiation protection and quality measures.
Both gamma cameras have two heads located in 90° orientation with low energy and high-resolution collimators. Window pulse analyzers at 20% located in 140 KeV photopic were used. The matrix used was 64x64 with maximum zoom of1.23. Thirty-two images of 20 seconds each were taken per head, for a total of 64 images in step and shot modality. In addition, contour orbit was made in a counterclockwise direction to verify the free execution of the rotation, without touching the patient or the stretcher, with 180° orbits and initial acquisition angle of -45°, with subsequent acquisitions up to 135°.
Tomographic reconstruction was performed using filtered back-projection (Butterworth filter of order 5, and cutoff frequency of 0.5), reorienting the axes of the heart to generate the coronal (short axis), sagittal (long vertical axis) and axial (horizontal long axis) sections. At least one physician with experience in nuclear cardiology carried out the normality assessment of a Gated-SPECT test, presence of ischemia or necrosis, and severity and extent.
To assess the phase analysis of the studies, the PHASE tool of the QPS-QGS program (Cedars-Sinai Medical Center, Los Angeles, USA) was used. The following parameters were obtained from the phase analysis, as well as the corresponding histogram curves: histogram bandwidth (HB), which includes 95% of the values obtained during the measurement phase; standard deviation of the phase (SD), in reference to the distribution phase; entropy (E), a variability measure expressed as a percentage from 0% to 100%, where 0% corresponds to perfect synchrony, and 100% to the maximum possible dyssynchrony in the ventricular contraction, and average regarding the obtained angles. To date, SD and HB are the parameters considered for clinical assessment 14. The least useful recognized parameter is average, so it was excluded from this study. The final display of the tool showing PA parameters considered as normal and abnormal is shown in Figures 1 and 2.
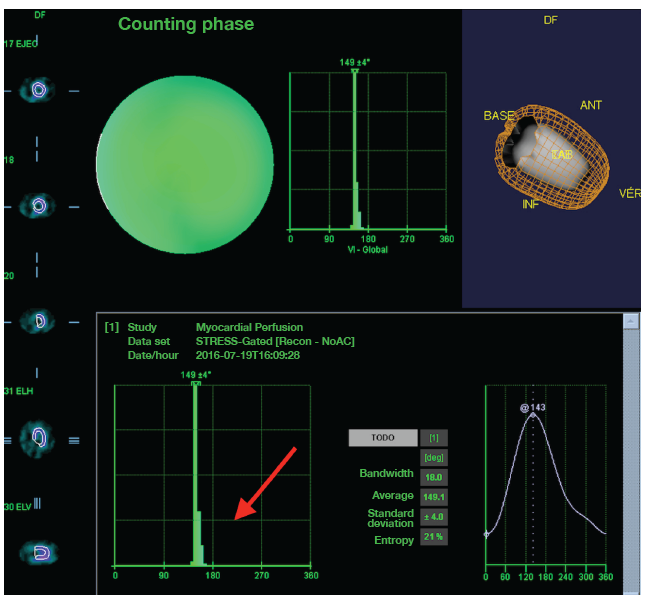
Figure 1: Female patient who underwent a Gated myocardial perfusion SPECT. Histogram representation of phase analysis with narrow bandwidth (arrow) and evidence of left ventricle mechanical synchronism. Source: Own elaboration based on the data obtained in the study.

Figure 2: Phase analysis for left ventricular mechanical synchronism assessment by myocardial perfusion SPECT. Phase analysis in which wide bandwidth can be observed over the histogram with evidence of mechanical dyssynchrony of the left ventricle with septal predominance (arrows). Source: Own elaboration based on the data obtained in the study.
The tool automatically yielded the quantitative parameters for the post-stress and post-rest phases. Based on these data, the corresponding analyzes and comparisons were made.
A descriptive analysis was performed using frequencies in the case of qualitative variables. On the other hand, quantitative variables, whether or not they followed a normal distribution (after applying the Kolmogorov-Smirnov normality test), were expressed by means and standard deviation or medians and interquartile range (IR). For the comparison of means or medians of the quantitative variables, parametric or non-parametric tests were used for independent or related samples, depending on the case. The value p <0.05 was taken as the limit to establish statistical significance. The IBM-SPSS V21® package was used for statistical analysis.
The protocol followed all relevant ethical recommendations and was formally reviewed and approved by the Ethics and Research Committees of Fundación Cardioinfantil - Instituto de Cardiología
Results
300 patients (117 women and 183 men), with a mean age of 65±12.7, were included. The most common indication for the study was chronic or acute chest pain (37.7%), followed by a history of coronary disease at follow-up (22.7%) and thoracic pain in patients with a history of known coronary disease (17%). The remaining 22.5% had other indications such as syncope study, recent arrhythmias, control of patients at cardiovascular risk, dyspnea, cardiac failure, myocardial viability assessment, and preoperative assessment. The technique was applied to all patients, since their study was properly synchronized with the electrocardiogram.
Of all patients, 31 (10.3%) had LBBB interventricular conduction disorders or a history of pacemaker implantation. Depending on the type of stress, 194 patients (64.7%) achieved vasodilator stress with intravenous dipyridamole; 94 (31.3%) with physical exercise test; 6 (2%) with dobutamine, and 6 (2%) with rest study, since they were requested to assess myocardial viability.
Of all the studies performed, 169 (56.9%) were interpreted as totally normal; 39 (13%) presented some degree of ischemia; 62 (20.7%) presented necrosis; 8 (3.7%) ischemia and necrosis, and 22 (7.3%) some type of finding other than ischemia or necrosis, but not considered as completely normal.
114 (38%) patients had their exam taken with a General-Electric® gamma camera and 186 (62%) with a Siemens® gamma camera.
An average dose of 1 GBq (27 mCi) per patient was given in one-day (23.3%) and two-day (62.3%) protocols. The stress-only protocol (12.3%) that was performed in hospitalized or emergency patients had normal results, therefore the rest study was not necessary. 8.7% of the patients presented an ejection fraction <35%, while the remaining 91.3% presented an ejection fraction >35%. The results shown and recorded in the tables are those obtained in the resting phase, except for patients who did not have a resting phase, which correspond to the aforementioned 12.3%.
When analyzing entirely technical factors, only normal perfusion studies were considered to avoid bias as much as possible, taking into account secondary parameter alterations in perfusion defects or synchronism of the patients. Thus, when analyzing normal perfusion studies, no differences were found in any of the parameters regardless of the type of stress exerted [HB (p=0.38), SD (p=0.8), E (p=0.84)], and used dose [HB (p=0.19), SD (p=0.05), E (p=0.06)]. Also, no differences between patients with or without a history of known coronary disease were observed [HB (p=0.44), SD (p=0.18), E (p=0.17)]. As for the gamma camera used, a difference in one of the parameters was found, while the other two did not show any [HB (p=0.02), SD (p=0.06), E (p=0.08)].
The analysis of PA parameters in patients undergoing both phases of the study (post-stress and post-rest) showed that there were no significant differences (analysis for related samples) when examining HB (p=0.4), SD (p=0.6) and E (p=0.7) in normal perfusion studies. On the other hand, when all the studies were analyzed, only differences in E values (p=0.01) could be observed, with no differences in HB (p=0.09) or SD (p=0.2).
Significant differences were found between the parameters of patients who had conduction disorders and those who did not: HB (p=0.001), SD (p=0.02), E (p=0.001). In turn, there were differences when comparing patients with ejection fraction greater or lower than 35% in all parameters, regardless of the phase: HB (p=0.001), SD (p=0.001), E (p=0.001).
There were significant differences in all parameters when comparing normal perfusion studies with necrosis studies: HB (p=0.001), SD (p=0.001), E (p=0.001). The observation of the parameters in both normal perfusion studies and all studies showed significant differences between men and women in all parameters: HB (p=0.002), SD (p=0.006), E (p=0.005). The numerical values are shown in Table 1.
* Patients with normal Gated-SPECT. IR: inrequartile range; HB: histogram bandwidth; SD: Standard deviation of the phase; E: entropy. Source: Own elaboration based on data obtained in the study.Table 1: Relevant results of phase analysis parameters.
Discussion
This research demonstrates the feasibility of the technique known as phase analysis of gated SPECT myocardial perfusion in nuclear medicine services and, therefore, in the current context of the profession. This is an automatic tool that is easy to apply to all Gated-SPECT studies and has gradually increased its usefulness worldwide.
The study did not show differences between parameters in both phases when examining only the normal studies. Only differences in entropy were found in all studies. These results are similar to those found by Zhou et al. 32, who studied 60 patients without finding differences between PA parameters in post-stress and post-rest studies. This is one of the most relevant findings of this study and is of great importance, since many nuclear medicine services conduct Gated-SPECT studies only in the post-rest phase, while other studies (as this one) do not include the post-rest phase if the post-stress phase is normal. The results show that the tool can be used in any of the phases without differences in the results. Furthermore, no dose-dependent differences were found, which is important since not all services, phases and patients use the same doses of radiotracer.
No relevant differences were found in relation to stress type (physical or pharmacological). This is of great importance because the type of stress can be provided in the aforementioned manners without affecting PA parameters based on the type of patient or clinical indication. Additionally, whether or not a patient has a known coronary disease does not seem to be influential, as long as the perfusion study is normal. That one of the analyzed parameters showed differences while the other two did not show any depending on the gamma camera used, which implies that it could be completely confirmed in other studies, although there is a trend towards non-difference.
As expected, significant differences were found between patients with and without conduction disorders when comparing all studies. In consequence, it is possible to effectively differentiate patients without conduction disorders from those with electrical synchronism alterations and left ventricle mechanical synchronism alterations. This finding is similar to other studies, and confirms the usefulness of the technique in this regard 11,14,26. However, the real usefulness of the tool, rather than discriminating between patients with or without conduction disorders, is to determine the cut-off points of the parameters of the phase analysis, which will help to establish if patients would respond or not to the CRT, although, this is not an objective of this study.
Moreover, differences were found among PA parameters regarding gender. When observing all studies or only normal studies, the parameters were higher in men than in women. The most relevant studies published that sought to obtain normal values and cut-off points of normality were carried out by Chen et al. 5 and Romero-Farina et al. 11, which also showed these differences. Thus, normality parameters should be considered for each gender.
Similarly, significant differences were observed between patients with normal myocardial perfusion studies and necrosis, as well as between patients with or without major systolic dysfunction (ejection fraction < or >35%, respectively). These results are consistent with other studies that included patients with necrosis or systolic dysfunction, and showed that the degree of left ventricular mechanical dyssynchrony is directly related to systolic dysfunction and to the extent of perfusion defects 33,34.
Continuing this type of studies is important to familiarize the branches of medicine involved (nuclear medicine and cardiology) with the tool and its clinical utility, to gradually resolve any concerns that may arise from it.
A possible limitation of the study, and a possible source of error, is its retrospective character. With this in mind, the methodology and results obtained make it difficult to perform an adequate multivariate analysis to assess the influence of some variables on others.
Another factor that should be considered is that, when referring normal perfusion studies, patients are not necessarily completely normal from a clinical cardiovascular point of view, but are patients with normal perfusion studies. This occurs because few clinically normal patients who require myocardial perfusion studies are referred to these services. Likewise, as the clinical implementation of the tool increases, the number of clinically normal patients who would benefit from the study decreases.
In addition, this article approaches clinical reality without having normal patients as a direct objective, but considering the patients who, in general, are studied in myocardial perfusion investigations and those who would receive potential benefits from the technique.
Conclusions
The use of the phase analysis tool included in the main programs for the processing of myocardial perfusion studies is feasible in the current professional context and can be used in the corresponding clinical scenario.
The parameters of the phase analysis are not affected and can, therefore, be used without depending on the type of stress (physical or pharmacological), the dose administered, the phase of the study in which the test is performed (post-stress or post-rest), or the gamma camera used.
Nevertheless, these parameters are affected by the variables of the patients themselves, such as gender (which must have normal values), the presence of intracardiac conduction disorders or fixed perfusion defects considered as necrosis, and systolic dysfunction.
Acknowledgement
None stated by the authors.
References
Referencias
Yaghoobi N, Malek H. The Age of Reason for Gated SPECT MPI to Deal With Cardiac Dyssynchrony. Res Cardiovasc Med. 2015;4(1):e25851. http://doi.org/b4zg.
Nakamura K, Takami M, Shimabukuro M, Maesato A, Chinen I, Ishigaki S, et al. Effective prediction of response to cardiac resynchronization therapy using a novel program of gated myocardial perfusion single photon emission computed tomography. Europace. 2011;13(12):1731-7. http://doi.org/dfxtfb.
Brignole M, Auricchio A, Baron-Esquivias G, Bordachar P, Boriani G, Breithardt OA, et al. 2013 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: the Task Force on cardiac pacing and resynchronization therapy of the European Society of Cardiology (ESC). Developed in collaboration with the European Heart Rhythm Association (EHRA). Eur Heart J. 2013;34(29):2281-329. http://doi.org/f22ff8.
Tracy CM, Epstein AE, Darbar D, Dimarco JP, Dunbar SB, Estes MNA III, et al. 2012 ACCF/AHA/HRS focused update of the 2008 guidelines for device-based therapy of cardiac rhythm abnormalities: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2012;60(14):1297-313. http://doi.org/f2nbt7.
Chen J, Garcia EV, Folks RD, Cooke CD, Faber TL, Tauxe EL, et al. Onset of left ventricular mechanical contraction as determined by phase analysis of ECG-gated myocardial perfusion SPECT imaging: development of a diagnostic tool for assessment of cardiac mechanical dyssynchrony. J Nucl Cardiol. 2005;12(6):687-95. http://doi.org/b384d4.
Casáns-Tormo I, Jurado-López JA. Diagnóstico de la enfermedad coronaria mediante gated-SPECT de perfusión miocárdica. Revista Española de Cardiología Suplementos. 2008;8(2):15B-24B. http://doi.org/bj5tgb.
Ypenburg C, Schalij MJ, Bleeker GB, Steendijk P, Boersma E, Dibbets-Schneider P, et al. Impact of viability and scar tissue on response to cardiac resynchronization therapy in ischaemic heart failure patients. Eur Heart J. 2007;28(1):33-41. http://doi.org/dh3cwj.
Matsuo S. Phase analysis using gated myocardial perfusion single-photon emission computed tomography imaging for evaluating cardiac dyssynchrony. Circ J. 2012;76(8):1832-3. http://doi.org/b4zh.
Leva L, Brambilla M, Cavallino C, Matheoud R, Occhetta E, Marino P, et al. Reproducibility and variability of global and regional dyssynchrony parameters derived from phase analysis of gated myocardial perfusion SPECT. Q J Nucl Med Mol Imaging. 2012;56(2):209-17.
Trimble MA, Velazquez EJ, Adams GL, Honeycutt EF, Pagnanelli RA, Barnhart HX, et al. Repeatability and reproducibility of phase analysis of gated single-photon emission computed tomography myocardial perfusion imaging used to quantify cardiac dyssynchrony. Nucl Med Commun. 2008;29(4):374-81. http://doi.org/cg2dgz.
Romero-Farina G, Aguadé-Bruix S, Candell-Riera J, Pizzi MN, García-Dorado D. Cut-off values of myocardial perfusion gated-SPECT phase analysis parameters of normal subjects, and conduction and mechanical cardiac diseases. J Nucl Cardiol. 2015;22(6):1247-58. http://doi.org/f7sz5c.
Chen J, Kalogeropoulos AP, Verdes L, Butler J, Garcia EV. Left-ventricular systolic and diastolic dyssynchrony as assessed by multi-harmonic phase analysis of gated SPECT myocardial perfusion imaging in patients with end-stage renal disease and normal LVEF. J Nucl Cardiol. 2011;18(2):299-308. http://doi.org/fmgnn4.
Gutiérrez L, Peñafort F, Seretti I, Ortego R. Nuevas herramientas diagnósticas en Insuficiencia Cardiaca: análisis de fase mediante SPECT-Gatillado para evaluación de sincronía miocárdica. Rev Fed Arg Cardiol. 2013;42(2):102-12.
Van Kriekinge SD, Nishina H, Ohba M, Berman DS, Germano G. Automatic global and regional phase analysis from gated myocardial perfusion SPECT imaging: application to the characterization of ventricular contraction in patients with left bundle branch block. J Nucl Med. 2008;49(11):1790-7. http://doi.org/bfjd4b.
Beretta M, Mut F. Valoración de la sincronía mecánica del ventrículo izquierdo mediante Gated SPECT y análisis de fase. Alasbimn Journal. 2012 [cited 2017 Mar 30]. Available from: http://goo.gl/3dUTZf.
Chen J, Garcia EV, Bax JJ, Iskandrian AE, Borges-Neto S, Soman P. SPECT myocardial perfusion imaging for the assessment of left ventricular mechanical dyssynchrony. J Nucl Cardiol. 2011;18(4):685-94. http://doi.org/b4vw84.
Boogers MJ, Chen J, Van Bommel RJ, Borleffs CJ, Dibbets-Schneider P, van der Hiel B, et al. Optimal left ventricular lead position assessed with phase analysis on gated myocardial perfusion SPECT. Eur J Nucl Med Mol Imaging. 2011;38(2):230-8. http://doi.org/cjt428.
Lin X, Xu H, Zhao X, Chen J. Sites of latest mechanical activation as assessed by SPECT myocardial perfusion imaging in ischemic and dilated cardiomyopathy patients with LBBB. Eur J Nucl Med Mol Imaging. 2014;41(6):1232-9. http://doi.org/b4zj.
Chen J, Henneman MM, Trimble MA, Bax JJ, Borges-Neto S, Iskandrian AE, et al. Assessment of left ventricular mechanical dyssynchrony by phase analysis of ECG-gated SPECT myocardial perfusion imaging. J Nucl Cardiol. 2008;15(1):127-36. http://doi.org/bpfjb8.
Boogers MM, Chen J, Bax JJ. Myocardial perfusion single photon emission computed tomography for the assessment of mechanical dyssynchrony. Curr Opin Cardiol. 2008;23(5):431-9. http://doi.org/dsx8xk.
Peix A, Karell J, Rodríguez L, Cabrera LO, Padrón K, Carrillo R, et al. Gated SPECT myocardial perfusion imaging, intraventricular synchronism, and cardiac events in heart failure. Clin Nucl Med. 2014;36(6):498-504. http://doi.org/b4zk.
Zafrir N, Bental T, Strasberg B, Solodky A, Mats I, Gutstein A, et al. Yield of left ventricular dyssynchrony by gated SPECT MPI in patients with heart failure prior to implantable cardioverter-defibrillator or cardiac resynchronization therapy with a defibrillator: Characteristics and prediction of cardiac outcome. J Nucl Cardiol. 2015;24(1):122-9. http://doi.org/f9phkb.
Hage FG. Left ventricular mechanical dyssynchrony by phase analysis as a prognostic indicator in heart failure. J Nucl Cardiol. 2014;21(1):67-70. http://doi.org/b4zm.
Azizian N, Rastgou F, Ghaedian T, Golabchi A, Bahadorian B, Khanlarzadeh V, et al. LV Dyssynchrony Assessed With Phase Analysis on Gated Myocardial Perfusion SPECT Can Predict Response to CRT in Patients With End-Stage Heart Failure. Res Cardiovasc Med. 2014;3(4):e20720. http://doi.org/b4zn.
Uebleis C, Hellweger S, Laubender RP, Becker A, Sohn HY, Lehner S, et al. Left ventricular dyssynchrony assessed by gated SPECT phase analysis is an independent predictor of death in patients with advanced coronary artery disease and reduced left ventricular function not undergoing cardiac resynchronization therapy. Eur J Nucl Med Mol Imaging. 2012;39(10):1561-9. http://doi.org/b4zp.
Trimble MA, Borges-Neto S, Honeycutt EF, Shaw LK, Pagnanelli R, Chen J, et al. Evaluation of mechanical dyssynchrony and myocardial perfusion using phase analysis of gated SPECT imaging in patients with left ventricular dysfunction. J Nucl Cardiol. 2008;15(5):663-70. http://doi.org/fhnksf.
Henneman MM, Chen J, Ypenburg C, Dibbets P, Bleeker GB, Boersma E, et al. Phase analysis of gated myocardial perfusion single-photon emission computed tomography compared with tissue Doppler imaging for the assessment of left ventricular dyssynchrony. J Am Coll Cardiol. 2007;49(16):1708-14. http://doi.org/bfzcsd.
AlJaroudi W, Jaber WA, Grimm RA, Marwick T, Cerqueira MD. Alternative methods for the assessment of mechanical dyssynchrony using phase analysis of gated single photon emission computed tomography myocardial perfusion imaging. Int J Cardiovasc Imaging. 2012;28(6):1385-94. http://doi.org/bphd24.
Rastgou F, Shojaeifard M, Amin A, Ghaedian T, Firoozabadi H, Malek H, et al. Assessment of left ventricular mechanical dyssynchrony by phase analysis of gated-SPECT myocardial perfusion imaging and tissue Doppler imaging: comparison between QGS and ECTb software packages. J Nucl Cardiol. 2014;21(6):1062-71. http://doi.org/b4zq.
AlJaroudi W, Alraies MC, DiFilippo F, Brunken RC, Cerqueira MD, Jaber WA. Effect of stress testing on left ventricular mechanical synchrony by phase analysis of gated positron emission tomography in patients with normal myocardial perfusion. Eur J Nucl Med Mol Imaging. 2012;39(4):665-72. http://doi.org/fzq39d.
Chen CC, Huang WS, Hung GU, Chen WC, Kao CH, Chen J. Left-ventricular dyssynchrony evaluated by Tl-201 gated SPECT myocardial perfusion imaging: a comparison with Tc-99m sestamibi. Nucl Med Commun. 2013;34(3):229-32. http://doi.org/f44vr4.
Zhou Y, Li D, Feng J, Yuan D, Patel Z, Cao K, et al. Left Ventricular Dyssynchrony Parameters Measured by Phase Analysis of Post-stress and Resting Gated SPECT Myocardial Perfusion Imaging. World J Nucl Med. 2013;12(1):3-7. http://doi.org/b4zr.
Wang J, Wang Y, Zhang X, Zhou R, Niu R, Lu P. [Left ventricular systolic synchrony assessed by phase analysis of gated myocardial perfusion imaging in patients with old myocardial infarction]. Zhonghua Xin Xue Guan Bing Za Zhi. 2015;43(7):599-604. Chinese.
Vidigal-Ferreira MJ, Silva R, Cabanelas N, Cunha MJ, Ramos D, Albuquerque A, et al. Left ventricular mechanical dyssynchrony in patients with impaired left ventricular function undergoing gated SPECT myocardial perfusion imaging. Rev Port Cardiol. 2013;32(5):387-94. http://doi.org/f2j5vt.
Cómo citar
APA
ACM
ACS
ABNT
Chicago
Harvard
IEEE
MLA
Turabian
Vancouver
Descargar cita
CrossRef Cited-by
1. Maziar Sabouri, Ghasem Hajianfar, Zahra Hosseini, Mehdi Amini, Mobin Mohebi, Tahereh Ghaedian, Shabnam Madadi, Fereydoon Rastgou, Mehrdad Oveisi, Ahmad Bitarafan Rajabi, Isaac Shiri, Habib Zaidi. (2022). Myocardial Perfusion SPECT Imaging Radiomic Features and Machine Learning Algorithms for Cardiac Contractile Pattern Recognition. Journal of Digital Imaging, 36(2), p.497. https://doi.org/10.1007/s10278-022-00705-9.
2. Leonardo Cadavid Blanco, José R. Arriaza-Madrid, Adriana J. Rosales-Morales. (2023). Disincronía miocárdica en pacientes sometidos a estudio de Spect gatillado y análisis de fase. Revista Repertorio de Medicina y Cirugía, 32(2), p.156. https://doi.org/10.31260/RepertMedCir.01217372.1271.
3. Adrian Espejel‐Guzman, Alfonso Gonzalez‐Trejo, Neftali Eduardo Antonio‐Villa, Enrique C. Guerra, Erick Alexanderson‐Rosas, Nilda Espinola‐Zavaleta. (2026). Clinical Utility of Mechanical Echocardiographic Dispersion to Assess Left Ventricular Function and Ischemia or Infarction Detected by Gated 99M‐Tc Sestamibi‐SPECT. Echocardiography, 43(5) https://doi.org/10.1111/echo.70481.
Dimensions
PlumX
Visitas a la página del resumen del artículo
Descargas
Licencia
Derechos de autor 2017 Revista de la Facultad de Medicina

Esta obra está bajo una licencia Creative Commons Reconocimiento 3.0 Unported.
-


















