



Publicado
Traumatic abdominal wall hernia from handlebar injury, laparoscopic repair - Report of two cases
Hernia traumática de la pared abdominal por lesión del manubrio, reparación laparoscópica - Informe de dos casos
Palabras clave:
Handlebar injury, blunt abdominal wall hernia, laparoscopic repair of abdominal hernia. (en)Lesión de manubrio, hernia de pared abdominal, reparación laparoscópica de la hernia abdominal. (es)
Descargas
Although rare, traumatic abdominal wall hernia associated with handlebar injury is a well-described entity in the pediatric population with about 40 cases and only one laparoscopic repair reported in children. We present two cases of male patients, 9 and 13 years old, who were assessed in our emergency room for blunt abdominal trauma associated with handlebar injury. The patients showed signs of handlebar trauma in the abdominal wall: one presented with a painful mass, and the other with intermittent pain in the area of trauma with no palpable mass. Neither of the patients were hemodynamically unstable or showed any peritoneal signs.
Ultrasound and CT scans were performed in both patients to identify abdominal wall hernias containing bowel content in the absence of other injuries. Laparoscopic repair was performed uneventfully in both patients with interrupted non-absorbable multifilament suture with 2 and 3 ports respectively.
Oral intake was initiated one day after surgery and both patients were discharged the following day. In the follow-up visit, the patients were asymptomatic and no signs of abdominal wall hernias were found.
Laparoscopic repair of blunt traumatic abdominal wall hernias is safe and technically possible in children and should be considered as the standard initial approach in the stable patient.
Aunque rara, la hernia traumática de la pared abdominal asociada a una lesión en el manubrio es una entidad bien descrita en la población pediátrica, con aproximadamente 40 casos y solo se informó una reparación laparoscópica en niños. Presentamos dos casos de pacientes varones, de 9 y 13 años de edad, que fueron evaluados en nuestra sala de emergencias por un traumatismo abdominal cerrado asociado con una lesión en el manubrio. Los pacientes mostraron signos de traumatismo del manubrio en la pared abdominal: uno presentó una masa dolorosa y el otro con dolor intermitente en el área de trauma sin masa palpable. Ninguno de los pacientes presentaba inestabilidad hemodinámica ni signos peritoneales.
Se realizaron ecografías y tomografías computarizadas en ambos pacientes para identificar las hernias de la pared abdominal que contenían contenido intestinal en ausencia de otras lesiones. La reparación laparoscópica se realizó sin incidentes en ambos pacientes con sutura discontinua no reabsorbible interrumpida con 2 y 3 puertos respectivamente.
La ingesta oral se inició un día después de la cirugía y ambos pacientes fueron dados de alta al día siguiente. En la visita de seguimiento, los pacientes estaban asintomáticos y no se encontraron signos de hernias de la pared abdominal.
La reparación laparoscópica de las hernias de pared abdominal traumáticas romas es segura y técnicamente posible en los niños y debe considerarse como el abordaje inicial estándar en el paciente estable.
TRAUMATIC ABDOMINAL WALL HERNIA FROM HANDLEBAR INJURY, LAPAROSCOPIC REPAIR REPORT OF TWO CASES
Santiago Correa-Salazar,
Juan Javier Valero-Halaby,
Jorge Ricardo Beltran-Chitiva,
Fenando Fierro-Avila.
Pediatric Surgery Department.
Fundación Hospital de la Misericordia,
Universidad Nacional de Colombia.
Correspondence to:
Santiago Correa, Bogota D.C., Colombia.
Email : tiagosan25@hotmail.com
ABSTRACT
Although rare, traumatic abdominal wall hernia associated with handlebar injury is a well-described entity in the pediatric population with about 40 cases and only one laparoscopic repair reported in children. We present two cases of male patients, 9 and 13 years old, who were assessed in our emergency room for blunt abdominal trauma associated with handlebar injury. The patients showed signs of handlebar trauma in the abdominal wall: one presented with a painful mass, and the other with intermittent pain in the area of trauma with no palpable mass. Neither of the patients were hemodynamically unstable or showed any peritoneal signs. Ultrasound and CT scans were performed in both patients to identify abdominal wall hernias containing bowel content in the absence of other injuries. Laparoscopic repair was performed uneventfully in both patients with interrupted non-absorbable multifilament suture with 2 and 3 ports respectively. Oral intake was initiated one day after surgery and both patients were discharged the following day. In the follow-up visit, the patients were asymptomatic and no signs of abdominal wall hernias were found.
Laparoscopic repair of blunt traumatic abdominal wall hernias is safe and technically possible in children and should be considered as the standard initial approach in the stable patient.
Keywords: Handlebar injury, blunt abdominal wall hernia, laparoscopic repair of abdominal hernia.
INTRODUCTION
Although handlebar injuries are well known in children, abdominal wall hernias secondary to this mechanism are rare. There are few reported cases of this kind, with about only 40 reported cases identified in the reviewed literature (2). Traditionally, management has consisted in repairing the defect through an incision above the hernia or by laparotomy, though other authors propose a conservative approach in the asymptomatic patient (3,4), and there is only one report of laparoscopic repair (1). We present two cases of abdominal wall hernias repaired successfully by laparotomy.
CASE 1
A 13-year-old boy was referred to our institution three days after suffering a handlebar injury in the right iliac fossa. He presented with history of abdominal pain, nausea and vomiting. On examination he was hemodynamically stable, though a handlebar sign was present in the right iliac fossa (fig 1) with tenderness. No palpable mass was found.

Fig 1. Handlebar sign.
An abdominal ultrasound was performed in the referring institution with an image that suggested a traumatic abdominal wall hernia. A CT scan was performed, without evidence of lesion in the solid viscera and the traumatic hernia was confirmed with bowel protruding trough the defect (fig 2).

Fig 2. CT scan, with an abdominal wall defect and small bowel trhough it.
The patient was taken to the operating room. The laparoscopic approach was performed with one 10 mm port at the umbilicus and two 5 mm ports in the right flank and left iliac fossa, respectively. A 2 cm defect above the internal right inguinal ring was found (fig 3), compromising the peritoneum and transverse and oblique muscles.
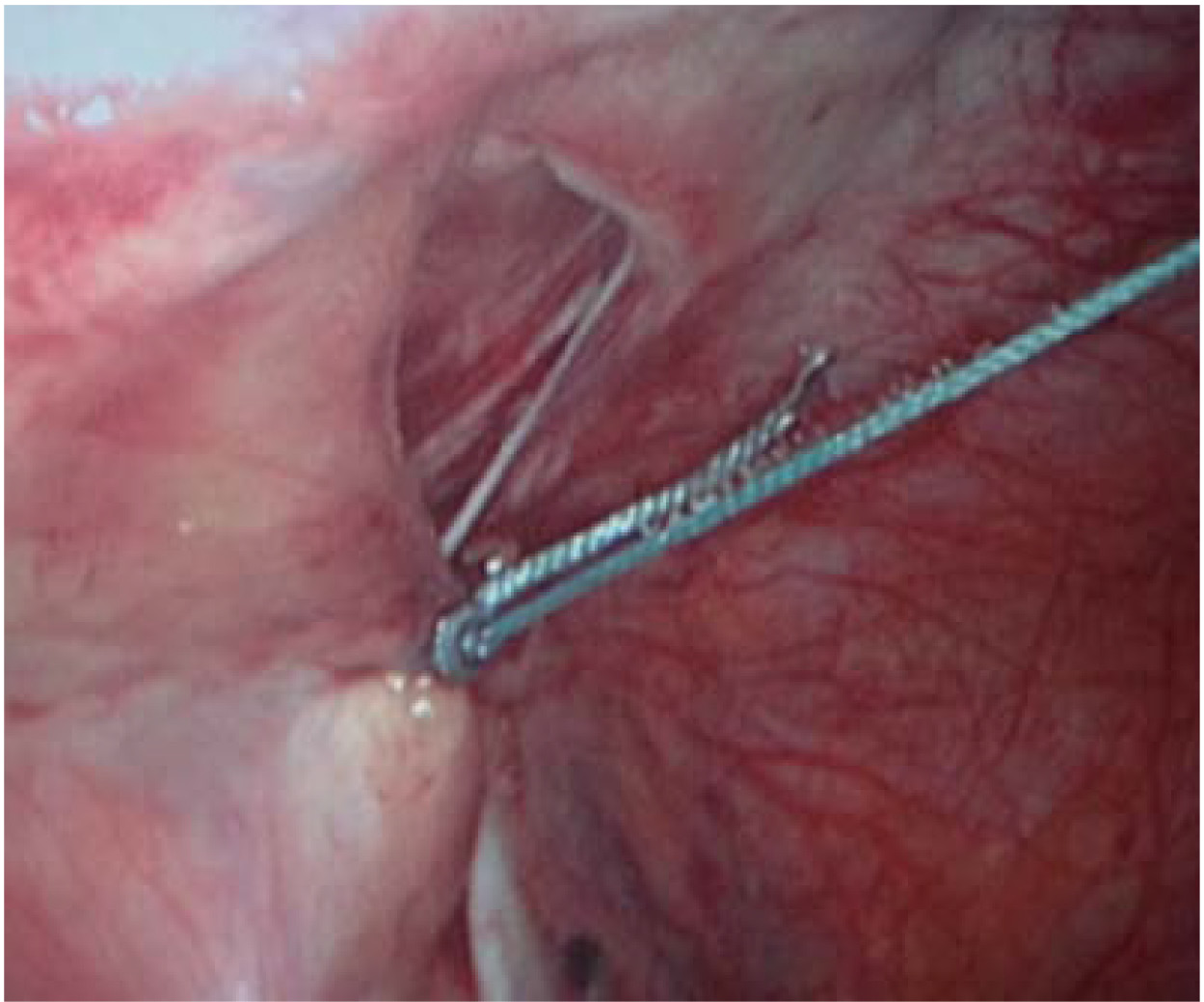
Fig 3. Traumatic abdominal wall defect above the internal inguinal ring.
The defect contained a segment of ileum, which was reduced, and no signs of ischemia or lesion in its mesentery were found. The defect was closed (fig 4) with interrupted non-absorbable multifilament sutures using the extracorporeal knot tying technique. Oral intake was initiated the next day, and the patient was discharged the following day. In the first follow-up visit, the patient was doing well, without palpable masses or abdominal pain. After two years, the patient remains asymptomatic regarding the abdominal wall hernia with no recurrence.
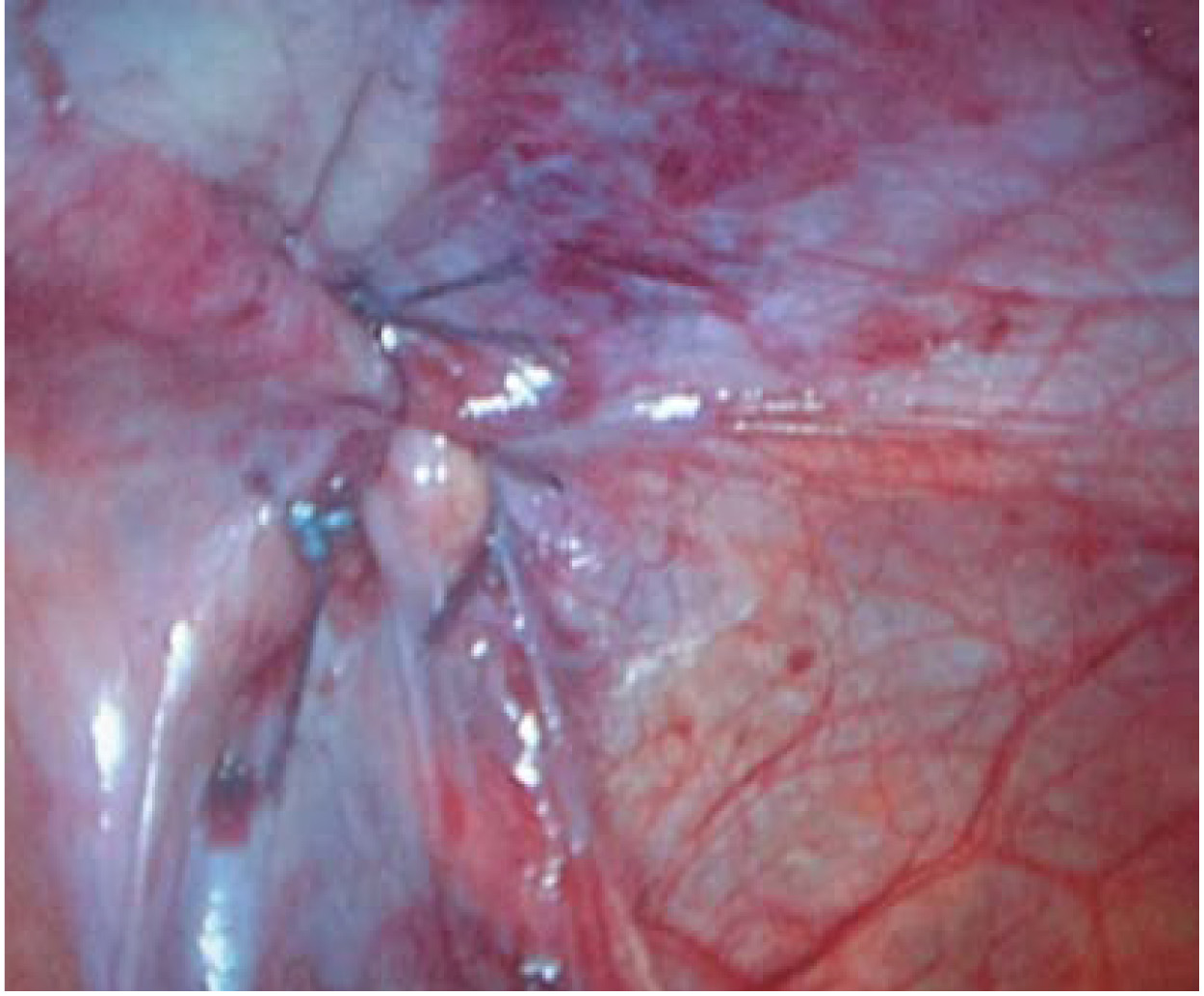
Fig 4. Closed defect.
CASE 2
A 9-year-old boy presented to our institution 12 hours after suffering a handlebar injury in the upper-left abdomen. After the injury, he noticed a painful abdominal mass at this level, and subsequently, vomiting. On examination, the patient was hemodynamically stable, with the handlebar sign (Fig 5) at the level of the upper-left abdomen, with a tender palpable mass.

Fig 5. Handlebar sign.
An ultrasound was performed, and an abdominal wall hernia was identified and confirmed by a CT scan evaluation (Fig 6) in which no other lesions were found. The abdominal wall hernia was filled by a small bowel segment.

Fig 6. CT scan demostrates the presence of an abdominal wall hernia with bowel content.
Based on these findings, the patient was taken to the operating room for laparoscopic repair. Two 5 mm ports were used, one through the umbilicus and one in the right iliac fossa, after the pneumoperitoneum was insufflated. Only the omentum (Fig 7) was identified inside the hernia, and was reduced.

Fig 7. Abdominal wall hernia with omentum.
The defect was about 4 to 5 cm long compromising the peritoneum and transverse and oblique muscles. It was corrected with interrupted non-absorbable sutures. The needle was passed through 2 mm skin incisions above the hernia and recovered with an endoscopic needle holder. Then, the edges of the hernia were taken and the needle was recovered again trough the skin incision. The suture was tied until the defect was corrected completely. Oral intake was initiated and tolerated the next day and the patient was discharged the following day. In the follow-up visit, the patient was doing well, without signs of hernia recurrence.
DISCUSSION
Abdominal wall hernias represent about 1% of lesions related to blunt trauma (1). Although rare, traumatic abdominal wall hernia associated with handlebar injury is a well-described entity (1) in the pediatric population with about 40 cases reported in the reviewed literature (2). Most cases of pediatric handlebar injuries occur between the ages of 9 and 14 (8). Abdominal wall hernias can be detected soon after handlebar injury or a few days after as it is not always evident in the physical examination, such as it was in our first case and other reported cases (5). Additionally, a lack of knowledge of this pathology might result in missed and underreported cases in the asymptomatic patient (4).
As described above, a high index of suspicion is needed to perform the diagnosis (7), and complementary imaging using abdominal ultrasound and CT scan might also be necessary. In one of our children, clinical findings were insufficient to perform the diagnosis and complementary images were needed. CT scans will also help in the evaluation of additional injuries (5).
Usually in children, these kinds of hernias are secondary to a low energy trauma, as in bicycle handlebar injuries (5), and it is secondary to a sudden application of blunt force that is insufficient to penetrate the skin but strong enough to disrupt the muscle and fascia (6). In the reviewed literature no major related injuries were reported and were correlated with the findings in our cases (6).
Open layer repair has been used traditionally either through an incision above the hernia or by laparotomy (2,5). Laparoscopy has been used for diagnostic purposes (2,6) and there is one report of laparoscopic repair using an Endo Close TM system (Covidien, Mansfield, MA) (1). We present two different techniques that can be used in the management of this disease that are reproducible with adequate results. Other authors have postulated the possibility of a conservative approach for the asymptomatic patients, as they identify spontaneous resolution with time (3,4). Nevertheless, we don’t have enough experience with this approach to be able to recommend it. Early primary repair is also reported to limit ongoing morbidity related to pain, limitation of function, and hospital stay (7).
Laparoscopic repair of blunt traumatic abdominal wall hernias is safe and technically possible in children, and should be considered as the standard initial approach in the stable patient.
REFERENCES
1. Rowell EE, Chin AC. Laparoscopic repair of traumatic abdominal wall hernia from handlebar injury. J Pediatr Surg. 2011;46(5):e9-12. doi: http://doi.org/bm69qh.
2. Rathore A, Simpson BJ, Diefenbach KA. Traumatic abdominal wall hernias: an emerging trend in handlebar injuries. J Pediatr Surg. 2012;47(7):1410-3. doi: http://doi.org/2d8.
3. Litton K, Izzidien AY, Hussien O, Vali A. Conservative management of a traumatic abdominal wall hernia after a bicycle handlebar injury (case report and literature review). J Pediatr Surg. 2008;43(4):e31-2. doi: http://doi.org/d5gh4z.
4. Upasani A, Bouhadiba N. Paediatric abdominal wall hernia following handlebar injury: should we diagnose more and operate less? BMJ Case Rep; 2013.
5. Van Bemmel AJ, van Marle AG, Schlejen PM, Schmitz RF. Handlebar hernia: a case report and literature review on traumatic abdominal wall hernia in children. Hernia. 2011;15(4):439-42. doi: http://doi.org/bdrgc7.
6. Iinuma Y, Yamazaki Y, Hirose Y, Kinoshita H, Kumagai K, Tanaka T, et al. A case of traumatic abdominal wall hernia that could not be identified until exploratory laparoscopy was performed. Pediatr Surg Int. 2005;21(1):54-7. doi: http://doi.org/csm5d8.
7. Yan J, Wood J, Bevan C, Cheng W, Wilson G. Traumatic abdominal wall hernia – a case report and literature review. J Pediatr Surg. 2011;46(8):1642-5. doi: http://doi.org/bgsnzv.
8. Nataraja RM, Palmer CS, Arul GS, Bevan C, Crameri J. The full spectrum of handlebar injuries in children: A decade of experience. Injury. 2014;45(4):684-9. doi: http://doi.org/2d9.
Referencias
Rowell EE, Chin AC. Laparoscopic repair of traumatic abdominal wall hernia from handlebar injury. J Pediatr Surg. 2011;46(5):e9-12. doi: http://doi.org/bm69qh.
Rathore A, Simpson BJ, Diefenbach KA. Traumatic abdominal wall hernias: an emerging trend in handlebar injuries. J Pediatr Surg. 2012;47(7):1410-3. doi: http://doi.org/2d8.
Litton K, Izzidien AY, Hussien O, Vali A. Conservative management of a traumatic abdominal wall hernia after a bicycle handlebar injury (case report and literature review). J Pediatr Surg. 2008;43(4):e31-2. doi: http://doi.org/d5gh4z.
Upasani A, Bouhadiba N. Paediatric abdominal wall hernia following handlebar injury: should we diagnose more and operate less? BMJ Case Rep; 2013.
Van Bemmel AJ, van Marle AG, Schlejen PM, Schmitz RF. Handlebar hernia: a case report and literature review on traumatic abdominal wall hernia in children. Hernia. 2011;15(4):439-42. doi: http://doi.org/bdrgc7.
Iinuma Y, Yamazaki Y, Hirose Y, Kinoshita H, Kumagai K, Tanaka T, et al. A case of traumatic abdominal wall hernia that could not be identified until exploratory laparoscopy was performed. Pediatr Surg Int. 2005;21(1):54-7. doi: http://doi.org/csm5d8.
Yan J, Wood J, Bevan C, Cheng W, Wilson G. Traumatic abdominal wall hernia – a case report and literature review. J Pediatr Surg. 2011;46(8):1642-5. doi: http://doi.org/bgsnzv.
Nataraja RM, Palmer CS, Arul GS, Bevan C, Crameri J. The full spectrum of handlebar injuries in children: A decade of experience. Injury. 2014;45(4):684-9. doi: http://doi.org/2d9.
Cómo citar
APA
ACM
ACS
ABNT
Chicago
Harvard
IEEE
MLA
Turabian
Vancouver
Descargar cita
Visitas a la página del resumen del artículo
Descargas
Licencia
Derechos de autor 2015 Case reports

Esta obra está bajo una licencia internacional Creative Commons Atribución-NoComercial-SinDerivadas 4.0.
Los autores al someter sus manuscritos conservarán sus derechos de autor. La revista tiene el derecho del uso, reproducción, transmisión, distribución y publicación en cualquier forma o medio.
El Formulario de Divulgación Uniforme para posibles Conflictos de Interés y los oficios de cesión de derechos y de responsabilidad deben ser entregados junto con el original.
Aquellos autores/as que tengan publicaciones con esta revista, aceptan los términos siguientes:
Los autores/as conservarán sus derechos de autor y garantizarán a la revista el derecho de primera publicación de su obra, el cual estará simultáneamente sujeto a la Licencia de reconocimiento de Creative Commons 4.0 que permite a terceros compartir la obra siempre que se indique su autor y su primera publicación en esta revista.
Los autores/as podrán adoptar otros acuerdos de licencia no exclusiva de distribución de la versión de la obra publicada (p. ej.: depositarla en un archivo telemático institucional o publicarla en un volumen monográfico) siempre que se indique la publicación inicial en esta revista.
Se permite y recomienda a los autores/as difundir su obra a través de Internet (p. ej.: en archivos telemáticos institucionales o en su página web) antes y durante el proceso de envío, lo cual puede producir intercambios interesantes y aumentar las citas de la obra publicada. (Véase El efecto del acceso abierto).























