



Publicado
Reformulación del cuestionario de Michel para tamizaje de migraña
Reformulation of Michel's Questionnaire for migraine screening
Palabras clave:
cefalea migrañosa, diagnóstico, tamizaje masivo, métodos. (es)migraine headache, diagnosis, mass screening, methods (en)
Antecedentes. Al estimar la prevalencia de migraña es importante conocer la capacidad discriminativa de la prueba empleada. El cuestionario de diagnóstico estandarizado para migraña de Michel es una herramienta útil en este sentido, pero es posible mejorar su capacidad diagnóstica ajustando los puntos asignados a cada ítem evaluado.
Material y métodos. Se aplicó el cuestionario a 170 estudiantes de psicología seleccionados al azar, con posterior evaluación por neurólogo para corroborar el diagnóstico de migraña. Se utilizó la metodología de Kraemer para reasignar el puntaje del cuestionario con base a la asociación de un modelo saturado de regresión binomial de los ítems del cuestionario. Se estimaron las curvas receptor-operador (ROC) para el sistema de puntuación original y para el sistema hallado, comparándolos por el método de máxima verosimilitud.
Resultados: Con los puntajes originales el área bajo ROC fue de 0.8529; el mejor puntaje discriminatorio 13 puntos, con sensibilidad de 58.6 por ciento (IC95% 44.9%-71.4%), especificidad 89.3 por ciento (IC 95% 82.0%-94.3%) y concordancia de 78.8 por ciento (IC 95% 71.9%-84.7%). Con el nuevo puntaje el área bajo ROC pasó a 0.907; la mejor capacidad de discriminación está en 18 puntos, con sensibilidad de 65.5 por ciento (IC95% 51.9%-77.5%), especificidad de 92.0 por ciento (IC95% 85.3%-93.3%) y concordancia de 84.7 por ciento (IC95% 76.4%-89.3%). La ROC del nuevo sistema de puntuación es mejor que la original (p=0.016).
Conclusiones. La reformulación del cuestionario optimiza la capacidad discriminatoria del cuestionario.
Background. For estimating the migraine prevalence is very important to know the discrimative property of a scale. Michel's Standardized Diagnostic Questionnaire is a useful tool for this proposal. However, it is possible to improve its diagnostic capacity after adjusting overall punctuation by item analysis.
Materials and methods. One-hundred and seventy students of psychology selected at ramdon filled out the Michel's Questionnaire, and after a neurologist made an interview in order to identify a migraine headache. Kraemer's method was used for reassigning a new score taking into account the association of a satured binomial regression model. Area under receptor-operator curve (ROC) was calcuted for the original and new score,
comparing by likelihood methods.
Results. For the original punctuation, the area under ROC was 0.853, and 13 was the best discriminatory score with sensitivity of 58.6% (95%CI 44.9%-71.4%), specificity 89.3% (95%CI 82.0%-94.3%), and concordance of 78.8% (95%CI 91.9%-84.7%). For the new way of punctuation, the area under ROC was 0.907 (95%CI), the best discriminatory score 18, with sensitivity in 65.5% (95%CI 51.9%-77.5%), specificity 92.0% (85.3%-93.3%), and concordance of 84.7% (95%CI 76.4%-89.3%). The area under ROC from the new punctuation was better than original one (p=0.016).
Conclusions. This reformulation of the Michel's questionnaire improves the discriminatory capacity of this scale.
INVESTIGACION ORIGINAL
Luis Alfonso Díaz Martínez 1 , Mauricio Rueda Sánchez 1.
1.Profesor Asociado,Grupo de Neuropsiquiatría, Centro de Investigaciones Biomédicas; Facultad de Medicina, Universidad Autónoma de Bucaramanga, Colombia.
Correspondencia: ldiaz6@unab.edu.co
Resumen
Antecedentes. Al estimar la prevalencia de migraña es importante conocer la capacidad discriminativa de la prueba empleada. El cuestionario de diagnóstico estandarizado para migraña de Michel es una herramienta útil en este sentido, pero es posible mejorar su capacidad diagnóstica ajustando los puntos asignados a cada ítem evaluado.
Material y métodos. Se aplicó el cuestionario a 170 estudiantes de psicología seleccionados al azar, con posterior evaluación por neurólogo para corroborar el diagnóstico de migraña. Se utilizó la metodología de Kraemer para reasignar el puntaje del cuestionario con base a la asociación de un modelo saturado de regresión binomial de los ítems del cuestionario. Se estimaron las curvas receptor-operador (ROC) para el sistema de puntuación original y para el sistema hallado, comparándolos por el método de máxima verosimilitud.
Resultados: Con los puntajes originales el área bajo ROC fue de 0.8529; el mejor puntaje discriminatorio 13 puntos, con sensibilidad de 58.6 por ciento (IC95% 44.9%-71.4%), especificidad 89.3 por ciento (IC 95% 82.0%-94.3%) y concordancia de 78.8 por ciento (IC 95% 71.9%-84.7%). Con el nuevo puntaje el área bajo ROC pasó a 0.907; la mejor capacidad de discriminación está en 18 puntos, con sensibilidad de 65.5 por ciento (IC95% 51.9%-77.5%), especificidad de 92.0 por ciento (IC95% 85.3%-93.3%) y concordancia de 84.7 por ciento (IC95% 76.4%-89.3%). La ROC del nuevo sistema de puntuación es mejor que la original (p=0.016).
Conclusiones. La reformulación del cuestionario optimiza la capacidad discriminatoria del cuestionario.
Palabras clave : cefalea migrañosa, diagnóstico, tamizaje masivo, métodos.
Díaz LA, Rueda M. Reformulación del cuestionario de Michel para tamizaje de migraña.Rev Fac Med Univ Nac Colomb. 2006; 54: 240-247.
Summary
Background. For estimating the migraine prevalence is very important to know the discrimative property of a scale. Michel's Standardized Diagnostic Questionnaire is a useful tool for this proposal. However, it is possible to improve its diagnostic capacity after adjusting overall punctuation by item analysis.
Materials and methods. One-hundred and seventy students of psychology selected at ramdon filled out the Michel's Questionnaire, and after a neurologist made an interview in order to identify a migraine headache. Kraemer's method was used for reassigning a new score taking into account the association of a satured binomial regression model. Area under receptor-operator curve (ROC) was calcuted for the original and new score,
comparing by likelihood methods.
Results. For the original punctuation, the area under ROC was 0.853, and 13 was the best discriminatory score with sensitivity of 58.6% (95%CI 44.9%-71.4%), specificity 89.3% (95%CI 82.0%-94.3%), and concordance of 78.8% (95%CI 91.9%-84.7%). For the new way of punctuation, the area under ROC was 0.907 (95%CI), the best discriminatory score 18, with sensitivity in 65.5% (95%CI 51.9%-77.5%), specificity 92.0% (85.3%-93.3%), and concordance of 84.7% (95%CI 76.4%-89.3%). The area under ROC from the new punctuation was better than original one (p=0.016).
Conclusions. This reformulation of the Michel's questionnaire improves the discriminatory capacity of this scale.
Key words : migraine headache, diagnosis, mass screening, methods.
Díaz LA, Rueda M. Reformulation of Michel's Questionnaire for migraine screening. Rev Fac Med Univ Nac Colomb. 2006; 54: 240-247.
Introducción
La migraña es un síndrome con una variedad de síntomas neurológicos y no neurológicos y no simplemente una cefalea (1). La prevalencia de migraña en la población general ronda en el 10 por ciento, siendo mayor en mujeres que en hombres, con un pico de incidencia entre los adolescentes, sin diferencias en cuanto al nivel educativo (2). Hay un patrón de herencia en donde el ser hijo de migrañoso implica un mayor riesgo de desarrollar la entidad que quién no lo es (2). En Colombia, los datos de prevalencia de migraña entre adultos, a partir de estudios neuroepidemiológicos , muestran que ésta oscila entre 4.2 y 10.2 por ciento, siendo también mayor entre mujeres que entre hombres, así como más frecuente en la zona andina que en la costa Atlántica (3,4).
El diagnóstico de migraña es eminentemente clínico y se fundamenta en la aplicación de los criterios de la Sociedad Internacional de Cefalea (IHS por su siglas en inglés). Estos criterios son ampliamente aceptados, pero tienen el inconveniente de que deben ser evaluados por una persona entrenada, lo cual demanda tiempo, tanto el requerido para lograr un óptimo entrenamiento como para aplicar los criterios paciente a paciente (5).
Dada la necesidad de evaluar rápidamente y con certeza grandes poblaciones de pacientes, se ha planteado la utilización de encuestas auto-aplicadas en donde las personas puedan informar la presencia o no de las principales características clínicas que definen el trastorno.
Michel y colaboradores en Francia estudiaron 166 trabajadores de los ferrocarriles de ese país y que sufrieran al menos un episodio de cefalea cada tres meses (6), entre quienes se aplicó un cuestionario diagnóstico estandarizado con el cual clasificaron a los individuos con o sin migraña. Los sujetos también fueron examinados por un neurólogo enmascarado al resultado del cuestionario y quien los clasificó como sujetos con y sin migraña; este diagnóstico fue considerado como el estándar de oro y a partir de este diagnóstico calcularon la sensibilidad y especificidad del cuestionario. Finalmente, usaron un modelo de regresión logística para medir la asociación entre el diagnóstico de referencia de migraña y los criterios individuales de la IHS (5), determinando mediante una curva receptor-operado (ROC, por sus siglas en inglés) el punto de corte óptimo para el diagnóstico de migraña del cuestionario (6). La sensibilidad se encontró en 44 por ciento, con una especificidad del 92.7 por ciento. Los criterios "presencia de ataques", "al menos cinco ataques en la vida", Resumen
El diagnóstico de migraña es eminentemente clínico y se fundamenta en la aplicación de los criterios de la Sociedad Internacional de Cefalea (IHS por su siglas en inglés). Estos criterios son ampliamente aceptados, pero tienen el inconveniente de que deben ser evaluados por una persona entrenada, lo cual demanda tiempo, tanto el requerido para lograr un óptimo entrenamiento como para aplicar los criterios paciente a paciente (5).
Dada la necesidad de evaluar rápidamente y con certeza grandes poblaciones de pacientes, se ha planteado la utilización de encuestas auto-aplicadas en donde las personas puedan informar la presencia o no de las principales características clínicas que definen el trastorno.
Michel y colaboradores en Francia estudiaron 166 trabajadores de los ferrocarriles de ese país y que sufrieran al menos un episodio de cefalea cada tres meses (6), entre quienes se aplicó un cuestionario diagnóstico estandarizado con el cual clasificaron a los individuos con o sin migraña. Los sujetos también fueron examinados por un neurólogo enmascarado al resultado del cuestionario y quien los clasificó como sujetos con y sin migraña; este diagnóstico fue considerado como el estándar de oro y a partir de este diagnóstico calcularon la sensibilidad y especificidad del cuestionario. Finalmente, usaron un modelo de regresión logística para medir la asociación entre el diagnóstico de referencia de migraña y los criterios individuales de la IHS (5), determinando mediante una curva receptor-operado (ROC, por sus siglas en inglés) el punto de corte óptimo para el diagnóstico de migraña del cuestionario (6). La sensibilidad se encontró en 44 por ciento, con una especificidad del 92.7 por ciento. Los criterios "presencia de ataques", "al menos cinco ataques en la vida", "agravación por el esfuerzo físico" y "fotofobia y fonofobia" no estuvieron asociados estadísticamente con el estado de migraña y fueron excluidos del puntaje. Después de eliminar estos criterios no informativos, el puntaje se estableció a partir de cinco criterios, todos pertenecientes a la definición de migraña de la IHS : duración entre cuatro y 72 horas, localización unilateral, intensidad que impide las actividades diarias, dolor tipo pulsatil y presencia de náuseas o vómito, asignando en caso de ser la respuesta positiva cuatro puntos a los tres primeros aspectos y cinco puntos a los dos últimos. La suma de los puntos refleja la probabilidad de ser un migrañoso. De acuerdo al análisis de la ROC , Michel y colaboradores propusieron que los pacientes con cefalea con un puntaje igual o mayor a 17 fueran considerados como migraña y que aquellos con menos o igual a 10 como no migrañosos. Los sujetos entre 11 y 16 debian ser considerados como indeterminados y deben ser evaluados por especialista para un diagnóstico certero de migraña (6).
Recientemente, se realizó un estudio de validación del cuestionario de Michel en población universitaria colombiana por medio de un proceso de muestreo transversal (7), a partir del cual se logró establecer la asociación entre las preguntas que contiene el cuestionario y el diagnóstico clínico de migraña de tal manera que es posible reformular la manera como se agrupan las respuestas y el valor del puntaje que se le asigna a cada una, con lo que fue posible mejorar el desempeño de esta prueba diagnóstica. En este artículo se presenta en detalle cuáles son los elementos de análisis que llevan a esta propuesta.
Material y métodos
El estudio se realizó entre los estudiantes de la facultad de Psicología de la Universidad Autónoma de Bucaramanga, Colombia. Se incluyeron todos los individuos de ambos géneros entre 16 y 30 años de edad matriculados durante el segundo semestre académico de 2002 y que aceptaron participar en el proyecto luego de obtener su consentimiento informado. El estudio fue aprobado previamente por el Comité de Ética en Investigación de la Facultad de Medicina de la Universidad.
Se aplicó la versión en español del cuestionario diagnóstico estandarizado de migraña de Michel en 357 estudiantes, luego se seleccionaron, al azar y de forma independiente a los resultados del cuestionario, a 188 de ellos para verificación prospectiva del diagnóstico. Esta evaluación de la validez de criterio se hizo por medio de una entrevista clínica especializada como estándar de referencia, enmascarando al clínico y al estudiante respecto al resultado inicial del cuestionario. Esta entrevista se realizó en un lapso de dos a tres semanas luego de la aplicación del cuestionario.
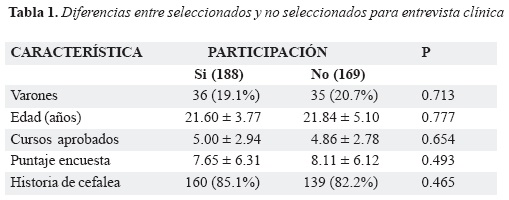
Para establecer la existencia de posible sesgo de selección en cada momento en que se reducía el número de personas, se compararon aquellas incluidas versus las no incluidas en cuanto a los parámetros comunes existentes en cada momento. Estos momentos fueron al aplicar el cuestionario (aceptantes vs no aceptantes), al seleccionar los estudiantes para entrevista clínica (seleccionados vs no seleccionados) y al acudir a la misma (asistentes vs no asistentes). Para establecer la significancia de las diferencias se utilizaron las pruebas X 2 y t de Student (8).
Se estimaron los indicadores de capacidad diagnóstica, sensibilidad, especificidad y valores predictivos positivo y negativo, así como el análisis del comportamiento de la ROC para los distintos puntos de corte resultantes (9). Posteriormente se utilizó la metodología de Kraemer para asignar un puntaje a cada respuesta positiva del cuestionario con base a la fuerza de asociación resultante de la estimación de un modelo de regresión binomial hecho a partir de todas las respuestas al cuestionario como variables independientes, frente al diagnóstico de migraña hecho por el clínico como variable dependiente (10); previamente se había estimado la fuerza de la asociación por medio del cálculo de la razón de prevalencia (RP) y su intervalo de confianza del 95 por ciento (IC95%). El modelo multivariado se realizó con base a las recomendaciones de Greenland (11), validando sus hallazgos por medio del análisis de bondad de ajuste propuesto por Tsiatis (12).
Finalmente, se estimaron las curvas ROC para el sistema de puntuación original propuesto por Michel y para el sistema hallado, comparándolos por el método de máxima verosimilitud. En todos los casos de prueba estadística se utilizó como un nivel de significancia inferior a 0.05. El análisis se realizó en Stata 9.0 (13).
Resultados
De los 405 estudiantes activos en la facultad de psicología, 48 (11.9%) no participaron en la encuesta de tamizaje. Nueve (18.8%) de los estudiantes que no participaron en la encuesta eran varones, mientras que 71 (19.9%) lo eran entre quienes sí participaron (p= 0.853); a su vez, quienes no participaron habían aprobado 5.08 (DE 2.66) niveles, promedio que es estadísticamente similar a los que habían aprobado los estudiantes que participaron (4.84, DE 2.86; p= 0.748).
De los 357 estudiantes que contestaron la encuesta, 144 (40.3%) manifestaron haber sufrido al menos un episodio de cefalea durante el último año. Se seleccionaron al azar 188 (52.7%) de los estudiantes que contestaron el cuestionario, de los cuales se evaluaron 170 (90.4%). No existió diferencia en la proporción de varones e historia de cefalea entre los estudiantes que fueron escogidos para entrevista clínica frente a los que no, así como tampoco en la edad, cursos aprobados y puntaje del cuestionario; igual ocurrió entre los asistentes a la entrevista clínica frente a los que no asistieron (Tabla 1).
Los 170 estudiantes evaluados por el clínico tenían entre 17 y 39 años (rango intercuartil [RIQ] entre 19 y 23 años). Estaban matriculados entre 1º y 10º nivel, con RIQ entre 2º y 7º nivel. El puntaje de la encuesta de tamizaje osciló entre 0 y 22 puntos (RIQ entre 0 y 5 puntos), con tan sólo un 25% de las personas entre 13 y 22 puntos.
Se hizo el diagnóstico de migraña en 58 de los 170 estudiantes evaluados (34.1%, IC95% 27.0%-41.8%). Todas las características de la cefalea detectadas por la encuesta de tamizaje se asociaron con la presencia de migraña (Tabla 2).

En cuanto a la capacidad del cuestionario de Michel para discriminar a los pacientes con migraña de los que no, se tiene que a partir de 17 o más puntos (puntaje recomendado originalmente por los autores), esta prueba tiene una sensibilidad de 37.9 por ciento (IC95% 25.8%-51.7%), especificidad de 99.1 por ciento (IC95% 94.4%-100%), lo que dada la prevalencia de migraña en la población estudiada implica un valor predictivo positivo de 95.7 por ciento (IC95% 76.0%-99.8%) y negativo de 75.5 por ciento (IC 95% 67.6%-82.1%).
El área bajo la curva ROC es de 0.853 (IC95% 0.803-0.922). El mejor puntaje discriminatorio o de concordancia fue 13 puntos, para el cual la sensibilidad fue 58.6% (IC95% 44.9%-71.4%), especificidad 89.3% (IC 95% 82.0%-94.3%) y concordancia 78.8% (IC 95% 71.9%-84.7%).
El modelo más adecuado para explicar la asociación entre las preguntas del cuestionario y tener migraña se puede ver en la tabla 3; es de resaltar que este modelo integra las preguntas sobre sufrir de fotofobia, sonofobia o náusea durante los episodios de cefalea en un solo ítem llamado «manifestaciones autonómicas». Este modelo ajusta adecuadamente dado que las asociaciones no se modifican cuando al modelo se incorpora el término de pronóstico generado por el modelo original (12).
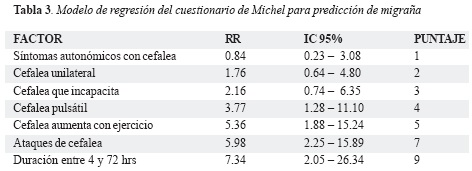
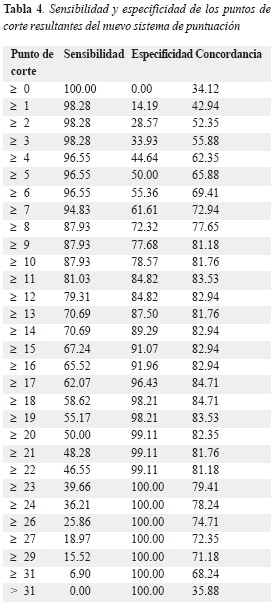
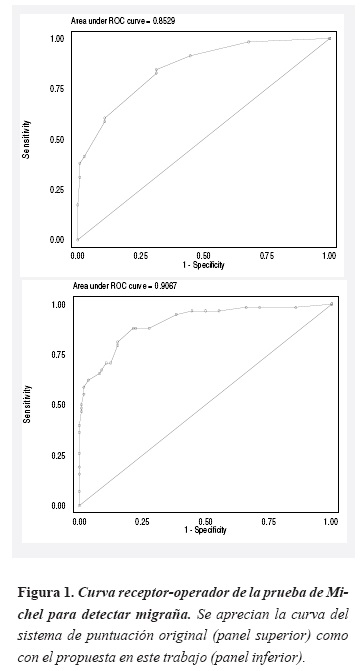
A partir de este modelo de regresión se asignaron puntos a cada respuesta positiva según lo propuesto por Kraemer (10), generándose una nueva escala de puntaje para predecir migraña que se ve en la columna final de la tabla 3. El área bajo la curva de ROC es de 0.907 (IC 95% 0.858-0.956). La mejor capacidad de discriminación se encontró en 18 puntos, con sensibilidad de 65.5 por ciento (IC95% 51.9%-77.5%), especificidad de 92.0 por ciento (IC95% 85.3%-93.3%) y concordancia de 84.7 por ciento (IC95% 76.4%-89.3%); en la tabla 4 se pueden apreciar los indicadores de desempeño de algunos puntajes clave. Esta manera de generar una escala de puntaje implica una curva ROC más capaz frente a la originalmente establecida (p = 0.016, figura 1).
Discusión
El diagnóstico de migraña es enteramente clínico y se basa en los criterios de la IHS (5). No existe un marcador biológico de la enfermedad, lo cual plantea un problema en estudios como el presente, ya que para generar un adecuado referente (estándar de oro), se requiere de un neurólogo o un médico entrenado para aplicar los criterios diagnósticos sin sesgo, lo que en estudios poblacionales resulta costoso.
La mayoría de los estudios de prevalencia de migraña han utilizado cuestionarios diagnósticos; sin embargo, para poder utilizar adecuadamente una herramienta de este tipo, es necesario conocer de antemano la sensibilidad, especificidad, valor predictivo positivo y valor predictivo negativo entre la población objetivo para así corregir los estimados crudos de prevalencia hallados, lo que pocas veces se hace (14). Es evidente que los presentes resultados obligan a realizar este ajuste, ya que a pesar de que las preguntas del cuestionario diagnóstico de migraña esencialmente son los criterios de la IHS de migraña hechos preguntas, no se alcanzan valores predictivos del 100 por ciento, con una apreciable proporción de falsos positivos y negativos. Esto implica que cuando el cuestionario va a ser utilizado en estudios de prevalencia, éste debe validarse en la población a la que se va a aplicar y la prevalencia debería calcularse restando los falsos positivos y sumando los falsos negativos a los individuos que contestaron el cuestionario por encima del punto de corte.
Por otro lado, una prueba de tamizaje adecuada ha de tener una muy buena sensibilidad, lo que en el cuestionario de Michel, aún en la reformulación de puntaje propuesta, es deficiente. Esto es explicable por la alta prevalencia de migraña en la población estudiada (14). La población en la que se hizo la validez de criterio es eminentemente joven y con predominio de mujeres, lo cual explica la muy alta prevalencia encontrada en la entrevista con el neurólogo. Con todo, el cuestionario de Michel es completo en la medida que todas las preguntas estuvieron asociadas con el diagnóstico clínico de migraña, lo que está en concordancia con el análisis de factores realizado. Esto es particularmente válido si se tiene en cuenta que no se presentó sesgo de selección (15).
El cuestionario de diagnóstico estandarizado de Michel es sencillo de aplicar dado básicamente por la mínima cantidad de preguntas, lo que facilita las respuestas al autoadministrarse. Pero, ¿por qué se ve afectada tan seriamente la sensibilidad? Por un lado está el efecto que tiene sobre los indicadores clínicos de sensibilidad y especificidad la muy alta prevalencia de migraña en la población estudiada (16).
El diagnóstico de migraña con base en un cuestionario tiene tres problemas. Primero, pueden ocurrir diferentes tipos de cefaleas en el mismo sujeto causando confusión en las respuestas; si bien, lo mismo puede ocurrir durante una entrevista clínica, el médico y el paciente tienen la oportunidad de aclarar la pregunta o la respuesta. Segundo, es posible que la naturaleza episódica de los síntomas de migraña haga que los individuos tengan variabilidad en la forma de evocación de la información, de tal manera que sujetos con episodios recientes contesten afirmativamente mientras que aquellos con episodios remotos los hayan olvidado y contesten en forma negativa. Finalmente, la variabilidad de los ataques de migraña puede influenciar la reproducibilidad ya que los sujetos pueden informar los síntomas basados en sus ataques más severos (1,2).
La sensibilidad, especificidad y los valores predictivos positivo y negativo del cuestionario de Michel hallados en este trabajo difieren un poco de los que originalmente se informaron en la población de trabajadores de los ferrocarriles franceses, pero los intervalos de confianza se sobreponen, por lo que creemos que las diferencias no son significativas. Desafortunadamente no tenemos los datos de Michel para comparar las curvas receptor-operador.
El replanteamiento que acá se propone del sistema de puntuación de cada pregunta permite generar una mejor ROC en la población estudiada, con un punto de corte con mejor sensibilidad y porcentaje de acuerdo y una pequeña disminución de la especificidad. Creemos que la variación entre los resultados de Michel y los nuestros se debe a las diferencias entre las poblaciones en quienes se validaron ya que en nuestra población predominaron las mujeres en una razón 4:1 y eran más jóvenes, ninguno de más de 30 años, comparado con la población de Michel que tenía una razón mujer a hombre de 1.2:1 y una edad promedio cercana a los 40 años.
Conclusión
El comportamiento de una herramienta diagnóstica basada en un cuestionario, puede variar dependiendo de la prevalencia de la enfermedad en la población en donde se aplique; por esto es recomendable que cuando se vaya a realizar un estudio de prevalencia utilizando una herramienta como el cuestionario diagnóstico de migraña de Michel, los investigadores previamente validen el cuestionario en la población en donde la van ha aplicar.
Agradecimientos
Es estudio fue copatrocinado por Colciencias y la Universidad Autónoma de Bucaramanga (Contrato 175-2002).
Referencias
1. Silberstein SD, Saper JR, Freitag FG . Migraine: diagnosis and treatment. In: Silberstein SD , Lipton RB, Dalessio DJ. Wolff's headache and other head pain. Oxford , Oxford University Press, 7 th ed, 2001:121-237.
2. Rasmussen BK, Steward WF . Epidemiology of migraine. In: Olsen J, Tfelt-Hansen P, Welch KMA (eds). The headaches. Philadelphia, Lippincott Williams & Wilkins, 2 ed, 2000: 227-233.
3. Pradilla G, Rosselli DA, Bautista LE, Vesga BE, León FE, Gómez A . Estudio nacional de prevalencia de enfermedades neurológicas EPINEURO. Bogotá, Ministerio de Salud, 1995.
4. Pradilla G, Vesga BE, Díaz LA, Baldovino ME, Salazar CM . Estudio neuroepidemiológico en la comunidad urbana de Piedecuesta, Santander.Acta Med Colomb. 2002; 27:407-420.
5. Headache Classification Committee of International Headache Society . Proposed classification and diagnostic criteria for headache disorders, cranial neuralgias, and facial pain.Cephalalgia. 1988; 8 (Suppl 7): 9-96.
6. Michel P, Henry P, Letenneur L, Jogeiz M, Corson A, Dartigues JF . Diagnostic screening for assessment of the HIS criteria for migraine by general practitioners.Cephalalgia. 1993; 13 (suppl 12): 54-59.
7. Rueda-Sánchez M, Díaz-Martínez LA . Validation of Michel´s questionnaire for migraine screening in a Colombian university population.Cephalalgia. 2004; 24:894-899.
8. Altman DG . Practical statistics for medical research. London , Chapman & Hall, 1991.
9. Beck JR, Shultz EK . The use of relative operating characteristic (ROC) curves in test perfomance evaluation.Arch Pathol Lab Med. 1986; 110:13-20.
10. Kraemer HC. Evaluating medical test. Objective and quantitative guidelines. Newbury Park , Sage publications, 1992.
11. Greenland S . Modeling and variable selection in epidemiologic analysis.Am J Public Health.1989; 79:340-349.
12. Tsiatis AA . A note on a goodness-of-fit test for the logistic regression model.Biometrika. 1980; 67:250-2511.
13. StataCorp LP . Stata: Release 9. College Station , 2005.
14. Diamond GA . Reverend Bayes' silent majority. An alternative factor affecting sensitivity and specificity of exercise electrocardiography.Am J Cardiol. 1988; 57:1175-1180.
15. Staquet M, Rozencweig M, Lee YJ, Muggia FM . Methodology for the assessment of new dichotomous diagnostic test.J Chron Dis. 1981; 34:599-610.
16. Hanley JA, McNeil BJ . The meaning and use of the area under a receiver operating characteristic (ROC) curve.Radiology. 1982; 43:29-36.
Referencias
Silberstein SD, Saper JR, Freitag FG . Migraine: diagnosis and treatment. In: Silberstein SD , Lipton RB, Dalessio DJ. Wolff's headache and other head pain. Oxford , Oxford University Press, 7 th ed, 2001:121-237.
Rasmussen BK, Steward WF . Epidemiology of migraine. In: Olsen J, Tfelt-Hansen P, Welch KMA (eds). The headaches. Philadelphia, Lippincott Williams & Wilkins, 2 ed, 2000: 227-233.
Pradilla G, Rosselli DA, Bautista LE, Vesga BE, León FE, Gómez A . Estudio nacional de prevalencia de enfermedades neurológicas EPINEURO. Bogotá, Ministerio de Salud, 1995.
Pradilla G, Vesga BE, Díaz LA, Baldovino ME, Salazar CM . Estudio neuroepidemiológico en la comunidad urbana de Piedecuesta, Santander.Acta Med Colomb. 2002; 27:407-420.
Headache Classification Committee of International Headache Society . Proposed classification and diagnostic criteria for headache disorders, cranial neuralgias, and facial pain.Cephalalgia. 1988; 8 (Suppl 7): 9-96.
Michel P, Henry P, Letenneur L, Jogeiz M, Corson A, Dartigues JF . Diagnostic screening for assessment of the HIS criteria for migraine by general practitioners.Cephalalgia. 1993; 13 (suppl 12): 54-59.
Rueda-Sánchez M, Díaz-Martínez LA . Validation of Michel´s questionnaire for migraine screening in a Colombian university population.Cephalalgia. 2004; 24:894-899.
Altman DG . Practical statistics for medical research. London , Chapman & Hall, 1991.
Beck JR, Shultz EK . The use of relative operating characteristic (ROC) curves in test perfomance evaluation.Arch Pathol Lab Med. 1986; 110:13-20.
Kraemer HC. Evaluating medical test. Objective and quantitative guidelines. Newbury Park , Sage publications, 1992.
Greenland S . Modeling and variable selection in epidemiologic analysis.Am J Public Health.1989; 79:340-349.
Tsiatis AA . A note on a goodness-of-fit test for the logistic regression model.Biometrika. 1980; 67:250-2511.
StataCorp LP . Stata: Release 9. College Station , 2005.
Diamond GA . Reverend Bayes' silent majority. An alternative factor affecting sensitivity and specificity of exercise electrocardiography.Am J Cardiol. 1988; 57:1175-1180.
Staquet M, Rozencweig M, Lee YJ, Muggia FM . Methodology for the assessment of new dichotomous diagnostic test.J Chron Dis. 1981; 34:599-610.
Hanley JA, McNeil BJ . The meaning and use of the area under a receiver operating characteristic (ROC) curve.Radiology. 1982; 43:29-36.
Cómo citar
APA
ACM
ACS
ABNT
Chicago
Harvard
IEEE
MLA
Turabian
Vancouver
Descargar cita
Visitas a la página del resumen del artículo
Descargas
Licencia
Derechos de autor 2006 Revista de la Facultad de Medicina

Esta obra está bajo una licencia internacional Creative Commons Atribución 4.0.
-


















