


Publicado
Fisiopatología del síndrome de apnea-hipopnea obstructiva del sueño (SAHOS)
Pathophysiology of obstructive sleep apnea-hypopnea syndrome (OSAHS)
DOI:
https://doi.org/10.15446/revfacmed.v65n1Sup.60091Palabras clave:
Síndromes de apnea del sueño, Sistema respiratorio, Hipercapnia, Hipofaringe, Nervio hipogloso. (es)Sleep Apnea Syndromes, Respiratory System, Hypercapnia, Hypopharynx, Hypoglossal Nerve. (en)
El síndrome de apnea-hipopnea obstructiva del sueño (SAHOS) es una enfermedad caracterizada por la obstrucción recurrente de la vía aérea superior (VAS), con disminución en el flujo de aire, hipoxemia intermitente y despertares durante el sueño. En la fisiopatología del SAHOS se presentan dos factores esenciales: las alteraciones anatómicas y la disminución o ausencia del control neural.
Durante el estudio del SAHOS se debe identificar el sitio o sitios de obstrucción de la VAS, que pueden ir desde las alas nasales hasta la hipofaringe. Otro factor importante en este síndrome es el influjo nervioso en el tono muscular de la hipofaringe, así como los cambios en el pH sanguíneo y secundarios a los microdespertares. La posición corporal y el estadio de sueño son factores determinantes de la severidad. La fisiopatología del SAHOS debe ser entendida para poder estudiar de forma adecuada a un paciente y darle la mejor opción de tratamiento.
Obstructive sleep apnea-hypopnea syndrome (OSAHS) is a disease characterized by recurrent upper airway obstruction (UAO), with decreased airflow, intermittent hypoxemia, and awakening during sleep. Two essential factors are related to the pathophysiology of OSAHS: anatomical alterations and reduction or absence of neural control.
While studying OSAHS, the site or sites of obstruction of the UA should be identified; they may extend from the nasal wings to the hypopharynx. Another important factor in this syndrome is the nervous influence on muscle tone of the hypopharynx, as well as the changes in blood pH, which are secondary to micro-arousals. Body position and sleep stage determine the severity. The pathophysiology of OSAHS should be understood to properly study a patient and provide the best treatment option.
artículo de reflexión
DOI: https://doi.org/10.15446/revfacmed.v65n1Sup.60091
Fisiopatología del síndrome de apnea-hipopnea obstructiva del sueño (SAHOS)
Pathophysiology of obstructive sleep apnea-hypopnea syndrome (OSAHS)
Recibido: 16/09/2016. Aceptado: 24/04/2017.
Marco Venegas-Mariño1 • Juan Camilo García2
1 Somnarum - Bogotá D.C. - Colombia.
2 Clínica Foscal - Insueño - Bucaramanga - Colombia.
Correspondencia: Marco Venegas-Mariño. Carrera 19 No. 84-17, oficina 302. Teléfono: +57 1 6366514; celular: +57 3114741747. Bogotá D.C. Colombia. Correo electrónico: marcoaureliovenegas@gmail.com.
| Resumen |
El síndrome de apnea-hipopnea obstructiva del sueño (SAHOS) es una enfermedad caracterizada por la obstrucción recurrente de la vía aérea superior (VAS), con disminución en el flujo de aire, hipoxemia intermitente y despertares durante el sueño. En la fisiopatología del SAHOS se presentan dos factores esenciales: las alteraciones anatómicas y la disminución o ausencia del control neural.
Durante el estudio del SAHOS se debe identificar el sitio o sitios de obstrucción de la VAS, que pueden ir desde las alas nasales hasta la hipofaringe. Otro factor importante en este síndrome es el influjo nervioso en el tono muscular de la hipofaringe, así como los cambios en el pH sanguíneo y secundarios a los microdespertares. La posición corporal y el estadio de sueño son factores determinantes de la severidad. La fisiopatología del SAHOS debe ser entendida para poder estudiar de forma adecuada a un paciente y darle la mejor opción de tratamiento.
Palabras clave: Síndromes de apnea del sueño; Sistema respiratorio; Hipercapnia; Hipofaringe; Nervio hipogloso (DeCS).
Venegas-Mariño M, García JC. Fisiopatología del síndrome de apnea-hipopnea obstructiva del sueño (SAHOS). Rev. Fac. Med. 2017;65:S25-8. Spanish. doi: https://doi.org/10.15446/revfacmed.v65n1Sup.60091.
| Abstract |
Obstructive sleep apnea-hypopnea syndrome (OSAHS) is a disease characterized by recurrent upper airway obstruction (UAO), with decreased airflow, intermittent hypoxemia, and awakening during sleep. Two essential factors are related to the pathophysiology of OSAHS: anatomical alterations and reduction or absence of
neural control.
While studying OSAHS, the site or sites of obstruction of the UA should be identified; they may extend from the nasal wings to the hypopharynx. Another important factor in this syndrome is the nervous influence on muscle tone of the hypopharynx, as well as the changes in blood pH, which are secondary to micro-arousals. Body position and sleep stage determine the severity. The pathophysiology of OSAHS should be understood to properly study a patient and provide the best treatment option.
Keywords: Sleep Apnea Syndromes; Respiratory System; Hypercapnia; Hypopharynx; Hypoglossal Nerve (MeSH).
Venegas-Mariño M, García JC. [Pathophysiology of obstructive sleep apnea-hypopnea syndrome (OSAHS)]. Rev. Fac. Med. 2017;65:S25-8. Spanish. doi: https://doi.org/10.15446/revfacmed.v65n1Sup.60091.
Introducción
El síndrome de apnea-hipopnea obstructiva del sueño (SAHOS) es una enfermedad que se caracteriza por la obstrucción o colapso recurrente de la vía aérea superior (VAS), con disminución en el flujo de aire, hipoxemia intermitente y despertares durante el sueño (1-4).
Dos factores esenciales deben ser tenidos en cuenta a la hora de estudiar la fisiopatología del SAHOS: las alteraciones anatómicas y la disminución o ausencia del control neural (5,6). A lo largo de la VAS existen estructuras rígidas y dinámicas cuya interacción genera permeabilidad, obstrucción o colapso de la vía aérea —dependiendo de la parte del ciclo respiratorio o etapa del sueño en que se encuentre el individuo—, lo que a su vez genera estabilidad en el proceso respiratorio (5,7).
Desarrollo
Factores anatómicos y musculares
La VAS es una estructura formada por nariz, faringe y laringe; se ha documentado que alrededor de 30 pares de músculos agonistas y antagonistas interactúan en el complejo comportamiento de la misma. Durante la vigilia, esta interacción está dada por la corteza cerebral, cuya actividad se deprime en el sueño e incrementa la regulación químico-neural de la musculatura faríngea. A continuación se describen las estructuras que pueden estar involucradas en la obstrucción del paso del aire en el SAHOS.
La nariz consta de estructuras rígidas, como el septum nasal y la pirámide ósea, que brindan un soporte importante; dichas estructuras pueden sufrir modificaciones y generar obstrucción. También es posible evaluar estructuras dinámicas, como las válvulas nasales, que pueden presentar eventos de colapso según la conformación de la unión septal con los cartílagos laterales. Los cornetes, aunque son estructuras rígidas en su mayor parte, presentan cambios obstructivos en los procesos de alergia (2).
La faringe es una estructura muy importante a evaluar, es un cilindro constituido por tejido musculofacial delgado que se engrosa al nivel de la línea media en su porción posterior, constituyendo la fascia bucofaríngea; este aspecto se debe tener en cuenta, pues, debido a dicha conformación blanda, representa la porción más dinámica del tracto respiratorio superior. Tres grandes segmentos la conforman en sentido rostro caudal —nasofaringe, orofaringe e hipofaringe— y en cada uno de estos se puede dar origen a diferentes tipos de obstrucción. Debido a sus funciones de fonación, deglución y respiración, la faringe requiere ser blanda y elástica (7); este hecho facilita eventos de obstrucción y colapso.
La obstrucción en la nasofaringe se produce en su mayoría por la hipertrofia adenoidea, pero también se da por otras alteraciones como la atresia de coanas, los tumores de origen linfoide, la disminución del diámetro secundario a malformaciones craneofaciales, entre otras (2). La orofaringe, en cambio, tiene uno de los componentes que brindan el mayor dinamismo del tracto respiratorio superior. La pared faríngea lateral y el paladar blando son los componentes que, con mayor frecuencia, tienen características de colapsabilidad dada la ausencia de soportes rígidos a este nivel (2,4,8).
Por otro lado, a nivel de la hipofaringe se encuentra la lengua, un grupo muscular importante en el que se incluye el músculo geniogloso, mayor dilatador de la vía aérea. Esta capacidad contráctil puede estar disminuida en los pacientes con SAHOS. También se encuentra la epiglotis, que en algunas oportunidades ofrece grados de colapsabilidad importantes.
Cualquier factor que comprometa la anatomía de la VAS o la función muscular —como músculos dilatadores disfuncionales— también predispone al SAHOS. El músculo dilatador más estudiado es el geniogloso y su adecuada contracción parece ser necesaria y suficiente para mantener la vía aérea abierta durante el sueño. La fatiga, el trauma neural y la miopatía pueden causar mal funcionamiento en personas con SAHOS (4,9).
La laringe posee un esqueleto cartilaginoso que le otorga rigidez suficiente para mantener la permeabilidad, aunque en algunas entidades puede brindar componentes obstructivos importantes.
Vale la pena resaltar que la hipoxia y el ronquido generan daño en la placa neuromuscular, lo que aumenta la fatigabilidad muscular; esto ocurre, en especial, en los músculos dilatadores, cuya actividad durante el sueño es esencial para mantener la permeabilidad de la VAS. En pacientes con SAHOS se observa una menor actividad neuromuscular con mayor colapso e hipoxia que acentúa dicha alteración neuromuscular (7).
Para comprender el dinamismo de la VAS se tiene que entender el modelo de Starling (Figura 1), donde la vía aérea —a nivel de la hipofaringe— es un tubo colapsable al interior de una cámara rígida —región cervical—. La presión por arriba de la faringe equivale a la atmosférica y la porción por debajo a la traqueal. Al mismo tiempo, se generan dos tipos de presiones: la intraluminal, que tiende a abrir la VAS, y la extraluminal, que tiende a cerrarla; la diferencia entre estas dos da como resultado la presión transmural, que determina el diámetro de la VAS (10-12). La presión a la cual se genera una obstrucción o colapso se llama presión crítica, siendo más positiva en pacientes con SAHOS que en individuos sanos (7).
La longitud de la VAS también es un factor importante, pues es más larga y genera mayor predisposición a la obstrucción en el caso de los hombres; sin embargo, su diámetro pareciera no tener repercusiones, dado que en los hombres es mayor. A pesar de lo anterior, la enfermedad tiene una prevalencia más alta en el género masculino (7).
Otro aspecto a tener en cuenta es la posición supina, que genera una redistribución de fluidos y tejidos blandos en dirección anteroposterior originando mayor tendencia al colapso. Si esto se asocia a una disminución del volumen pulmonar, hay un incremento importante en la predisposición al colapso de la VAS (7,9)
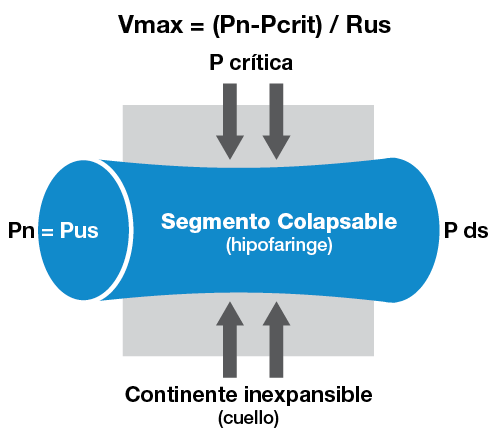
Figura 1. Modelo de Starling.
V: flujo aéreo; Pn: presión nasal, P ds: presión vías inferiores (traqueal); Rus: resistencia vías aéreas superiores; Pus: presión de las vías aéreas superiores.
Fuente: (13).
Factores dinámicos y neurológicos
Al observar los factores mecánicos y dinámicos de la faringe se pensó, durante algún tiempo, que estos explicaban por completo la fisiopatología del SAHOS. Sin embargo, observaciones posteriores han demostrado que el proceso es mucho más complejo que esto.
Como se observa con el modelo de Starling, la contracción del diafragma genera presión subatmosférica en la vía aérea durante la inspiración espontánea, lo que arrastra el flujo de aire al interior de la misma. Cuando se crea una presión intraluminal subatmosférica, las vías respiratorias inferiores permanecen permeables debido al soporte intramural de los anillos cartilaginosos en el árbol traqueobronquial. La hipofaringe carece de dicho soporte y depende de la configuración maleable de los tejidos blandos; su permeabilidad es, de esta manera, vulnerable a diversos factores como el tono muscular, la masa tisular y la cantidad de tejido adiposo.
Durante la vigilia, la hipofaringe se mantiene permeable debido a la actividad de numerosos músculos dilatadores, pero, después del inicio del sueño —cuando se reduce la actividad muscular—, la vía aérea se reduce en su diámetro y colapsa en los casos de SAHOS (8,14).
Una variable muy importante es la estabilidad del sistema de control respiratorio. Cuando el estímulo neurológico respiratorio central aumenta o disminuye, la actividad de los músculos dilatadores de la VAS varía, de tal manera que los momentos de disminución del estímulo neurológico se asocian a la reducción de la actividad dilatadora de los músculos de la VAS, a el aumento de la resistencia de la misma y a la predisposición al colapso. Así, la inestabilidad del control respiratorio —conocido como high loop gain— es, quizás, un factor causal en algunos de los casos de SAHOS.
Otro factor potencialmente importante es la propensión a despertarse —umbral de despertar—. Con el cese del flujo aéreo hay incremento de la presión arterial de dióxido de carbono (PaCO2) y disminución de la presión arterial de oxígeno (PaO2). Cuando esto ocurre, los quimioreceptores periféricos sensibles a la hipoxemia y los quimioreceptores centrales sensibles a la hipercapnia envían una señal de alarma al sistema nervioso central (SNC), haciendo que este incremente el impulso respiratorio central y, de manera secundaria, el tono muscular de la vía aérea para que se dilate de nuevo. Cuando el impulso central no es suficiente para dilatar la vía aérea ocurre activación de la corteza cerebral, lo que se traduce en un alertamiento o microalertamiento lo suficientemente largo para elevar el tono de los músculos estriados con dilatación de la vía aérea y finalización del evento obstructivo. La frecuente repetición de este fenómeno explica el fraccionamiento del sueño, el sueño poco reparador y la somnolencia diurna excesiva (SDE) al día siguiente.
Es bien conocido que durante el sueño REM (rapid eye movement) hay una tendencia general al incremento del índice de apnea e hipopnea (IAH) en comparación con el sueño Non-REM (non-rapid eye movement). Este hecho se explica por atonía de la musculatura estriada durante el sueño REM, la cual involucra los músculos faríngeos y respiratorios accesorios, respetando el diafragma y los músculos motores oculares externos, y ocasiona mayor colapso de la VAS.
Del mismo modo, se ha observado que durante el sueño REM ocurren mecanismos glutamatérgicos y GABAérgicos y se genera un poderoso sistema inhibitorio premotor glicerinérgico que contribuye a una disminución específica en la actividad sobre la motoneurona del nervio hipogloso mayor —XII par craneano—. En contraposición, durante el sueño de ondas lentas (N3) se observa la tendencia a una disminución marcada en el IAH, lo cual no se ha explicado de manera clara hasta el momento.
Los mecanoreceptores tienen un papel importante en la apnea obstructiva: se localizan dentro de las paredes faríngeas regulando, de manera específica, las motoneuronas del XII par craneal y se activan por la presión negativa intraluminal generada durante la inspiración. Estos receptores trasmiten dicha información aferente por vía del brazo superior del nervio laríngeo interno y las premotoneuronas del geniogloso localizadas cerca del obex median el reflejo. Este último es muy importante en la medida en que la activación de los músculos hipoglosos, causada por una caída en la presión, debe contrarrestar el colapso faríngeo. La activación de este reflejo disminuye y en ocasiones se suprime durante el sueño, lo cual es de gran importancia en la génesis de la apnea obstructiva (8).
Después del despertar o microdespertar, se incrementa el tono de la musculatura estriada, se permite el paso de aire y cesa la apnea. Sin embargo, la presión negativa al final de la apnea obstructiva es muy elevada, lo cual permite el ingreso de una gran cantidad de aire —fase hiperpneica—, presentándose el intercambio gaseoso de una manera muy rápida; la concentración de CO2 en la sangre puede caer por debajo del umbral de apnea, lo que el SNC interpreta como una hiperventilación y responde generando una apnea central. Los individuos con bajo umbral de despertar se pueden alertar incluso antes de que los músculos dilatadores puedan reabrir la vía aérea.
El volumen pulmonar también puede ser un factor contribuyente. En animales y en el ser humano el área transversal de la VAS se incrementa cuando el volumen pulmonar aumenta de forma natural o con incrementos pasivos en la capacidad residual funcional. Al contrario, la vía aérea es más pequeña y colapsa más fácil cuando el volumen pulmonar es pequeño. Esta relación existe, quizás, debido a que las vías aéreas superiores e inferiores se encuentran ligadas de forma mecánica, por lo que, con volúmenes pulmonares altos, las estructuras mediastinales se desplazan caudalmente, produciendo endurecimiento y dilatación de la vía aérea faríngea.
El incremento del volumen pulmonar también puede estabilizar el sistema de control respiratorio y, de esta forma, amortiguar los gases sanguíneos en los cambios de la ventilación. La capacidad residual funcional cae al pasar de la vigilia al sueño en personas de peso normal y, así, se presume que contribuye al colapso relacionado al sueño en el SAHOS. Sin embargo, incluso durante la vigilia, la obesidad reduce a menudo la capacidad residual funcional, especialmente en la posición supina. De otra parte, aún no es claro si el volumen pulmonar cae más en la transición de vigilia a sueño en pacientes obesos con SAHOS.
La retención de líquidos y el cambio de la distribución de los fluidos de los miembros inferiores al cuello durante la noche también pueden afectar la mecánica de la vía aérea. El edema puede ser especialmente problemático en casos de exceso de volumen de líquido extracelular, como en la insuficiencia cardíaca, enfermedad renal terminal e hipertensión arterial.
Conflicto de intereses
Ninguno declarado por los autores.
Financiación
Ninguna declarada por los autores.
Agradecimientos
A la Asociación Colombiana de Medicina Interna (ACMI® - Médicos para adultos), la Asociación Colombiana de Neurología (ACN) y la Asociación Colombiana de Sociedades Científicas (ACSC) por permitir a los autores usar sus instalaciones como lugar de reunión de trabajo.
Referencias
1.Chang ET, Yang MC, Wang HM, Lai HL. Snoring in a sitting position and neck circumference are predictors of sleep apnea in Chinese patients. Sleep Breath. 2014;18(1):133-6. http://doi.org/bnkb.
2.Schellenberg JB, Maislin G, Schwab RJ. Physical Findings and the Risk for Obstructive Sleep Apnea. The Importance of Oropharyngeal Structures. Am J Respir Crit Care Med. 2000;162(2 Pt 1):740-8. http://doi.org/bnkc.
3.Stradling JR, Crosby JH. Predictors and prevalence of obstructive sleep apnoea and snoring in 1001 middle aged men. Thorax. 1991;46(2):85-90. http://doi.org/bfdz7n.
4.Yagi H, Nakata S, Tsuge H, Yasuma F, Noda A, Morinaga M, et al. Morphological examination of upper airway in obstructive sleep. Auris Nasus Larynx. 2009;36(4):444-9. http://doi.org/bvrbtr.
5.Isaacs RS, Sykes JM. Anatomy and physiology of the upper airway. Anesthesiol Clin North America. 2002;20(4):733-45. http://doi.org/fnzpht.
6.Huang R, Li X, Rong Q. Control mechanism for the upper airway collapse in patients with obstructive sleep apnea syndrome: a finite element study. Sci China Life Sci. 2013;56(4):366-72. http://doi.org/bkrk.
7.Bilston LE, Gandevia SC. Biomechanical properties of the human upper airway and their effect on its behavior during breathing and in obstructive sleep apnea. J Appl Physiol. 2014;116(3):314-24. http://doi.org/bnkd.
8.Ramírez JM, García AJ 3rd, Anderson TM, Koschnitzky JE, Peng YJ, Kumar GK, et al. Central and peripheral factors contributing to obstructive sleep apneas. Respir Physiol Neurobiol. 2013;189(2):344-53. http://doi.org/bnkh.
9.Ishikawa T, Isono S, Aiba J, Tanaka A, Nishino T. Prone position increases collapsibility of the passive pharynx in infants and small children. Am J Respir Crit Care Med. 2002;166(5):760-764. http://doi.org/cnmmgj.
10.Marcus CL, McColley SA, Carroll JL, Loughlin GM, Smith PL, Schwartz AR. Upper airway collapsibility in children with obstructive sleep apnea syndrome. J Appl Physiol. 1994;77(2):918-24.
11.McNicholas WT, Coffey M, Boyle T. Effects of nasal airflow on breathing during sleep in normal humans. Am Rev Respir Dis. 1993;147(3):620-623. http://doi.org/bnkg.
12.Isono S, Feroah TR, Hajduk EA, Brabt R, Whitelaw WA, Remmers JE. Interaction of cross-sectional area, driving pressure, and airflow of passive velopharynx. J Appl Physiol. 1997;83(3):851-9.
13.Durán CJ, Rey J, De La Torre G, Aguirregomoscorta JM. Síndrome de apneas-hipopneas durante el sueño. In: Villasante C, editor. Enfermedades respiratorias. Madrid: Aula Médica; 2002. p. 265-81.
14.Barceló X, Mirapeix RM, Bugés J, Cobos A, Domingo C. Oropharyngeal examination to predict sleep apnea severity. Arch Otolaryngol Head Neck Surg. 2011;137(10):990-6. http://doi.org/d7b368.
Recibido: 16 de septiembre de 2016; Aceptado: 24 de abril de 2017
Resumen
El síndrome de apnea-hipopnea obstructiva del sueño (SAHOS) es una enfermedad caracterizada por la obstrucción recurrente de la vía aérea superior (VAS), con disminución en el flujo de aire, hipoxemia intermitente y despertares durante el sueño. En la fisiopatología del SAHOS se presentan dos factores esenciales: las alteraciones anatómicas y la disminución o ausencia del control neural.
Durante el estudio del SAHOS se debe identificar el sitio o sitios de obstrucción de la VAS, que pueden ir desde las alas nasales hasta la hipofaringe. Otro factor importante en este síndrome es el influjo nervioso en el tono muscular de la hipofaringe, así como los cambios en el pH sanguíneo y secundarios a los microdespertares. La posición corporal y el estadio de sueño son factores determinantes de la severidad. La fisiopatología del SAHOS debe ser entendida para poder estudiar de forma adecuada a un paciente y darle la mejor opción de tratamiento.
Palabras clave:
Síndromes de apnea del sueño, Sistema respiratorio, Hipercapnia, Hipofaringe, Nervio hipogloso (DeCS).Abstract
Obstructive sleep apnea-hypopnea syndrome (OSAHS) is a disease characterized by recurrent upper airway obstruction (UAO), with decreased airflow, intermittent hypoxemia, and awakening during sleep. Two essential factors are related to the pathophysiology of OSAHS: anatomical alterations and reduction or absence of neural control.
While studying OSAHS, the site or sites of obstruction of the UA should be identified; they may extend from the nasal wings to the hypopharynx. Another important factor in this syndrome is the nervous influence on muscle tone of the hypopharynx, as well as the changes in blood pH, which are secondary to micro-arousals. Body position and sleep stage determine the severity. The pathophysiology of OSAHS should be understood to properly study a patient and provide the best treatment option.
Keywords:
Sleep Apnea Syndromes, Respiratory System, Hypercapnia, Hypopharynx, Hypoglossal Nerve (MeSH).Introducción
El síndrome de apnea-hipopnea obstructiva del sueño (SAHOS) es una enfermedad que se caracteriza por la obstrucción o colapso recurrente de la vía aérea superior (VAS), con disminución en el flujo de aire, hipoxemia intermitente y despertares durante el sueño 1-4.
Dos factores esenciales deben ser tenidos en cuenta a la hora de estudiar la fisiopatología del SAHOS: las alteraciones anatómicas y la disminución o ausencia del control neural 5,6. A lo largo de la VAS existen estructuras rígidas y dinámicas cuya interacción genera permeabilidad, obstrucción o colapso de la vía aérea -dependiendo de la parte del ciclo respiratorio o etapa del sueño en que se encuentre el individuo-, lo que a su vez genera estabilidad en el proceso respiratorio 5,7.
Desarrollo
Factores anatómicos y musculares
La VAS es una estructura formada por nariz, faringe y laringe; se ha documentado que alrededor de 30 pares de músculos agonistas y antagonistas interactúan en el complejo comportamiento de la misma. Durante la vigilia, esta interacción está dada por la corteza cerebral, cuya actividad se deprime en el sueño e incrementa la regulación químico-neural de la musculatura faríngea. A continuación se describen las estructuras que pueden estar involucradas en la obstrucción del paso del aire en el SAHOS.
La nariz consta de estructuras rígidas, como el septum nasal y la pirámide ósea, que brindan un soporte importante; dichas estructuras pueden sufrir modificaciones y generar obstrucción. También es posible evaluar estructuras dinámicas, como las válvulas nasales, que pueden presentar eventos de colapso según la conformación de la unión septal con los cartílagos laterales. Los cornetes, aunque son estructuras rígidas en su mayor parte, presentan cambios obstructivos en los procesos de alergia 2.
La faringe es una estructura muy importante a evaluar, es un cilindro constituido por tejido musculofacial delgado que se engrosa al nivel de la línea media en su porción posterior, constituyendo la fascia bucofaríngea; este aspecto se debe tener en cuenta, pues, debido a dicha conformación blanda, representa la porción más dinámica del tracto respiratorio superior. Tres grandes segmentos la conforman en sentido rostro caudal -nasofaringe, orofaringe e hipofaringe- y en cada uno de estos se puede dar origen a diferentes tipos de obstrucción. Debido a sus funciones de fonación, deglución y respiración, la faringe requiere ser blanda y elástica 7; este hecho facilita eventos de obstrucción y colapso.
La obstrucción en la nasofaringe se produce en su mayoría por la hipertrofia adenoidea, pero también se da por otras alteraciones como la atresia de coanas, los tumores de origen linfoide, la disminución del diámetro secundario a malformaciones craneofaciales, entre otras 2. La orofaringe, en cambio, tiene uno de los componentes que brindan el mayor dinamismo del tracto respiratorio superior. La pared faríngea lateral y el paladar blando son los componentes que, con mayor frecuencia, tienen características de colapsabilidad dada la ausencia de soportes rígidos a este nivel 2,4,8.
Por otro lado, a nivel de la hipofaringe se encuentra la lengua, un grupo muscular importante en el que se incluye el músculo geniogloso, mayor dilatador de la vía aérea. Esta capacidad contráctil puede estar disminuida en los pacientes con SAHOS. También se encuentra la epiglotis, que en algunas oportunidades ofrece grados de colapsabilidad importantes.
Cualquier factor que comprometa la anatomía de la VAS o la función muscular -como músculos dilatadores disfuncionales- también predispone al SAHOS. El músculo dilatador más estudiado es el geniogloso y su adecuada contracción parece ser necesaria y suficiente para mantener la vía aérea abierta durante el sueño. La fatiga, el trauma neural y la miopatía pueden causar mal funcionamiento en personas con SAHOS 4,9.
La laringe posee un esqueleto cartilaginoso que le otorga rigidez suficiente para mantener la permeabilidad, aunque en algunas entidades puede brindar componentes obstructivos importantes.
Vale la pena resaltar que la hipoxia y el ronquido generan daño en la placa neuromuscular, lo que aumenta la fatigabilidad muscular; esto ocurre, en especial, en los músculos dilatadores, cuya actividad durante el sueño es esencial para mantener la permeabilidad de la VAS. En pacientes con SAHOS se observa una menor actividad neuromuscular con mayor colapso e hipoxia que acentúa dicha alteración neuromuscular 7.
Para comprender el dinamismo de la VAS se tiene que entender el modelo de Starling (Figura 1), donde la vía aérea -a nivel de la hipofaringe- es un tubo colapsable al interior de una cámara rígida -región cervical-. La presión por arriba de la faringe equivale a la atmosférica y la porción por debajo a la traqueal. Al mismo tiempo, se generan dos tipos de presiones: la intraluminal, que tiende a abrir la VAS, y la extraluminal, que tiende a cerrarla; la diferencia entre estas dos da como resultado la presión transmural, que determina el diámetro de la VAS 10-12. La presión a la cual se genera una obstrucción o colapso se llama presión crítica, siendo más positiva en pacientes con SAHOS que en individuos sanos 7.

Figura 1: Modelo de Starling. V: flujo aéreo; Pn: presión nasal, P ds: presión vías inferiores (traqueal); Rus: resistencia vías aéreas superiores; Pus: presión de las vías aéreas superiores.
La longitud de la VAS también es un factor importante, pues es más larga y genera mayor predisposición a la obstrucción en el caso de los hombres; sin embargo, su diámetro pareciera no tener repercusiones, dado que en los hombres es mayor. A pesar de lo anterior, la enfermedad tiene una prevalencia más alta en el género masculino 7.
Otro aspecto a tener en cuenta es la posición supina, que genera una redistribución de fluidos y tejidos blandos en dirección anteroposterior originando mayor tendencia al colapso. Si esto se asocia a una disminución del volumen pulmonar, hay un incremento importante en la predisposición al colapso de la VAS 7,9.
Factores dinámicos y neurológicos
Al observar los factores mecánicos y dinámicos de la faringe se pensó, durante algún tiempo, que estos explicaban por completo la fisiopatología del SAHOS. Sin embargo, observaciones posteriores han demostrado que el proceso es mucho más complejo que esto.
Como se observa con el modelo de Starling, la contracción del diafragma genera presión subatmosférica en la vía aérea durante la inspiración espontánea, lo que arrastra el flujo de aire al interior de la misma. Cuando se crea una presión intraluminal subatmosférica, las vías respiratorias inferiores permanecen permeables debido al soporte intramural de los anillos cartilaginosos en el árbol traqueobronquial. La hipofaringe carece de dicho soporte y depende de la configuración maleable de los tejidos blandos; su permeabilidad es, de esta manera, vulnerable a diversos factores como el tono muscular, la masa tisular y la cantidad de tejido adiposo.
Durante la vigilia, la hipofaringe se mantiene permeable debido a la actividad de numerosos músculos dilatadores, pero, después del inicio del sueño -cuando se reduce la actividad muscular-, la vía aérea se reduce en su diámetro y colapsa en los casos de SAHOS 8,14.
Una variable muy importante es la estabilidad del sistema de control respiratorio. Cuando el estímulo neurológico respiratorio central aumenta o disminuye, la actividad de los músculos dilatadores de la VAS varía, de tal manera que los momentos de disminución del estímulo neurológico se asocian a la reducción de la actividad dilatadora de los músculos de la VAS, a el aumento de la resistencia de la misma y a la predisposición al colapso. Así, la inestabilidad del control respiratorio -conocido como high loop gain- es, quizás, un factor causal en algunos de los casos de SAHOS.
Otro factor potencialmente importante es la propensión a despertarse -umbral de despertar-. Con el cese del flujo aéreo hay incremento de la presión arterial de dióxido de carbono (PaCO2) y disminución de la presión arterial de oxígeno (PaO2). Cuando esto ocurre, los quimioreceptores periféricos sensibles a la hipoxemia y los quimioreceptores centrales sensibles a la hipercapnia envían una señal de alarma al sistema nervioso central (SNC), haciendo que este incremente el impulso respiratorio central y, de manera secundaria, el tono muscular de la vía aérea para que se dilate de nuevo. Cuando el impulso central no es suficiente para dilatar la vía aérea ocurre activación de la corteza cerebral, lo que se traduce en un alertamiento o microalertamiento lo suficientemente largo para elevar el tono de los músculos estriados con dilatación de la vía aérea y finalización del evento obstructivo. La frecuente repetición de este fenómeno explica el fraccionamiento del sueño, el sueño poco reparador y la somnolencia diurna excesiva (SDE) al día siguiente.
Es bien conocido que durante el sueño REM (rapid eye movement) hay una tendencia general al incremento del índice de apnea e hipopnea (IAH) en comparación con el sueño Non-REM (non-rapid eye movement). Este hecho se explica por atonía de la musculatura estriada durante el sueño REM, la cual involucra los músculos faríngeos y respiratorios accesorios, respetando el diafragma y los músculos motores oculares externos, y ocasiona mayor colapso de la VAS.
Del mismo modo, se ha observado que durante el sueño REM ocurren mecanismos glutamatérgicos y GABAérgicos y se genera un poderoso sistema inhibitorio premotor glicerinérgico que contribuye a una disminución específica en la actividad sobre la motoneurona del nervio hipogloso mayor -XII par craneano-. En contraposición, durante el sueño de ondas lentas (N3) se observa la tendencia a una disminución marcada en el IAH, lo cual no se ha explicado de manera clara hasta el momento.
Los mecanoreceptores tienen un papel importante en la apnea obstructiva: se localizan dentro de las paredes faríngeas regulando, de manera específica, las motoneuronas del XII par craneal y se activan por la presión negativa intraluminal generada durante la inspiración. Estos receptores trasmiten dicha información aferente por vía del brazo superior del nervio laríngeo interno y las premotoneuronas del geniogloso localizadas cerca del obex median el reflejo. Este último es muy importante en la medida en que la activación de los músculos hipoglosos, causada por una caída en la presión, debe contrarrestar el colapso faríngeo. La activación de este reflejo disminuye y en ocasiones se suprime durante el sueño, lo cual es de gran importancia en la génesis de la apnea obstructiva 8.
Después del despertar o microdespertar, se incrementa el tono de la musculatura estriada, se permite el paso de aire y cesa la apnea. Sin embargo, la presión negativa al final de la apnea obstructiva es muy elevada, lo cual permite el ingreso de una gran cantidad de aire -fase hiperpneica-, presentándose el intercambio gaseoso de una manera muy rápida; la concentración de CO2 en la sangre puede caer por debajo del umbral de apnea, lo que el SNC interpreta como una hiperventilación y responde generando una apnea central. Los individuos con bajo umbral de despertar se pueden alertar incluso antes de que los músculos dilatadores puedan reabrir la vía aérea.
El volumen pulmonar también puede ser un factor contribuyente. En animales y en el ser humano el área transversal de la VAS se incrementa cuando el volumen pulmonar aumenta de forma natural o con incrementos pasivos en la capacidad residual funcional. Al contrario, la vía aérea es más pequeña y colapsa más fácil cuando el volumen pulmonar es pequeño. Esta relación existe, quizás, debido a que las vías aéreas superiores e inferiores se encuentran ligadas de forma mecánica, por lo que, con volúmenes pulmonares altos, las estructuras mediastinales se desplazan caudalmente, produciendo endurecimiento y dilatación de la vía aérea faríngea.
El incremento del volumen pulmonar también puede estabilizar el sistema de control respiratorio y, de esta forma, amortiguar los gases sanguíneos en los cambios de la ventilación. La capacidad residual funcional cae al pasar de la vigilia al sueño en personas de peso normal y, así, se presume que contribuye al colapso relacionado al sueño en el SAHOS. Sin embargo, incluso durante la vigilia, la obesidad reduce a menudo la capacidad residual funcional, especialmente en la posición supina. De otra parte, aún no es claro si el volumen pulmonar cae más en la transición de vigilia a sueño en pacientes obesos con SAHOS.
La retención de líquidos y el cambio de la distribución de los fluidos de los miembros inferiores al cuello durante la noche también pueden afectar la mecánica de la vía aérea. El edema puede ser especialmente problemático en casos de exceso de volumen de líquido extracelular, como en la insuficiencia cardíaca, enfermedad renal terminal e hipertensión arterial.
Conflicto de intereses
Ninguno declarado por los autores.
Financiación
Ninguna declarada por los autores.
Agradecimientos
A la Asociación Colombiana de Medicina Interna (ACMI® -Médicos para adultos), la Asociación Colombiana de Neurología (ACN) y la Asociación Colombiana de Sociedades Científicas (ACSC) por permitir a los autores usar sus instalaciones como lugar de reunión de trabajo.
Referencias
Referencias
Chang ET, Yang MC, Wang HM, Lai HL. Snoring in a sitting position and neck circumference are predictors of sleep apnea in Chinese patients. Sleep Breath. 2014;18(1):133-6. http://doi.org/bnkb.
Schellenberg JB, Maislin G, Schwab RJ. Physical Findings and the Risk for Obstructive Sleep Apnea. The Importance of Oropharyngeal Structures. Am J Respir Crit Care Med. 2000;162(2 Pt 1):740-8. http://doi.org/bnkc.
Stradling JR, Crosby JH. Predictors and prevalence of obstructive sleep apnoea and snoring in 1001 middle aged men. Thorax. 1991;46(2):85-90. http://doi.org/bfdz7n.
Yagi H, Nakata S, Tsuge H, Yasuma F, Noda A, Morinaga M, et al. Morphological examination of upper airway in obstructive sleep. Auris Nasus Larynx. 2009;36(4):444-9. http://doi.org/bvrbtr.
Isaacs RS, Sykes JM. Anatomy and physiology of the upper airway. Anesthesiol Clin North America. 2002;20(4):733-45. http://doi.org/fnzpht.
Huang R, Li X, Rong Q. Control mechanism for the upper airway collapse in patients with obstructive sleep apnea syndrome: a finite element study. Sci China Life Sci. 2013;56(4):366-72. http://doi.org/bkrk.
Bilston LE, Gandevia SC. Biomechanical properties of the human upper airway and their effect on its behavior during breathing and in obstructive sleep apnea. J Appl Physiol. 2014;116(3):314-24. http://doi.org/bnkd.
Ramírez JM, García AJ 3rd, Anderson TM, Koschnitzky JE, Peng YJ, Kumar GK, et al. Central and peripheral factors contributing to obstructive sleep apneas. Respir Physiol Neurobiol. 2013;189(2):344-53. http://doi.org/bnkh.
Ishikawa T, Isono S, Aiba J, Tanaka A, Nishino T. Prone position increases collapsibility of the passive pharynx in infants and small children. Am J Respir Crit Care Med. 2002;166(5):760-764. http://doi.org/cnmmgj.
Marcus CL, McColley SA, Carroll JL, Loughlin GM, Smith PL, Schwartz AR. Upper airway collapsibility in children with obstructive sleep apnea syndrome. J Appl Physiol. 1994;77(2):918-24.
McNicholas WT, Coffey M, Boyle T. Effects of nasal airflow on breathing during sleep in normal humans. Am Rev Respir Dis. 1993;147(3):620-623. http://doi.org/bnkg.
Isono S, Feroah TR, Hajduk EA, Brabt R, Whitelaw WA, Remmers JE. Interaction of cross-sectional area, driving pressure, and airflow of passive velopharynx. J Appl Physiol. 1997;83(3):851-9.
Durán CJ, Rey J, De La Torre G, Aguirregomoscorta JM. Síndrome de apneas-hipopneas durante el sueño. In: Villasante C, editor. Enfermedades respiratorias. Madrid: Aula Médica; 2002. p. 265-81.
Barceló X, Mirapeix RM, Bugés J, Cobos A, Domingo C. Oropharyngeal examination to predict sleep apnea severity. Arch Otolaryngol Head Neck Surg. 2011;137(10):990-6. http://doi.org/d7b368.
Cómo citar
APA
ACM
ACS
ABNT
Chicago
Harvard
IEEE
MLA
Turabian
Vancouver
Descargar cita
Licencia
Derechos de autor 2017 Revista de la Facultad de Medicina

Esta obra está bajo una licencia Creative Commons Reconocimiento 3.0 Unported.
-


















